

Ⅰ. Introduction
Ⅱ. Case Presentation
1. Case 1: Vestibuloplasty
2. Case 2: Soft Tissue Augmentation
3. Case 3: ARP
Ⅲ. Discussion
Ⅳ. Conclusion
Ⅰ. Introduction
In periodontal and implant surgery, restoration of soft tissue defects is essential to achieve long-term stable outcomes and esthetics. The most widely used clinical procedure is autologous tissue grafting, which is typically performed on the hard palate.1 Free gingival grafts (FGG) and connective tissue grafts (CTG) are highly effective in increasing keratinized tissue, covering gingival recession defects, and increasing the soft tissue volume of collapsed alveolar ridges.2 Their inherent tissue-specific cellular composition profoundly affects postoperative biological healing and ultimate treatment outcomes.3
Despite their clinical excellence, autogenous grafts require a second surgical site, which increases procedural complexity and patient morbidity.4,5,6 Anatomical limitations also restrict the harvestable amount of soft tissue to an adequate thickness.6 Consequently, porcine-derived collagen matrices have gained interest because of their biocompatibility and ability to serve as tissue-conductive scaffolds, eliminating donor-site morbidity.7,8
Extensive research has validated the histological integration and clinical prognosis of pioneering xenogeneic matrices, such as Mucograft or Fibro-Gide (Geistlich Pharma AG, Wolhusen, Switzerland).6,9 However, literature evaluating the clinical application of Collagen Graft x1D® (Genoss; Suwon, South Korea) across diverse surgical indications remains relatively scarce.
Therefore, this case series aimed to evaluate the clinical feasibility of Collagen Graft x1D across vestibuloplasty, soft tissue augmentation, and alveolar ridge preservation (ARP).
Ⅱ. Case Presentation
This retrospective case series, involving patients treated at the Department of Periodontology, National Health Insurance Service Ilsan Hospital, was conducted in accordance with the Declaration of Helsinki. As this report consists of a retrospective description of three completely anonymized clinical cases obtained during routine standard of care, it does not constitute human participants research requiring formal Institutional Review Board (IRB) approval. Specific written informed consent for publication was not obtained. However, all clinical and radiographic images were strictly anonymized and cropped to ensure complete patient privacy, making personal identification impossible.
1. Case 1: Vestibuloplasty
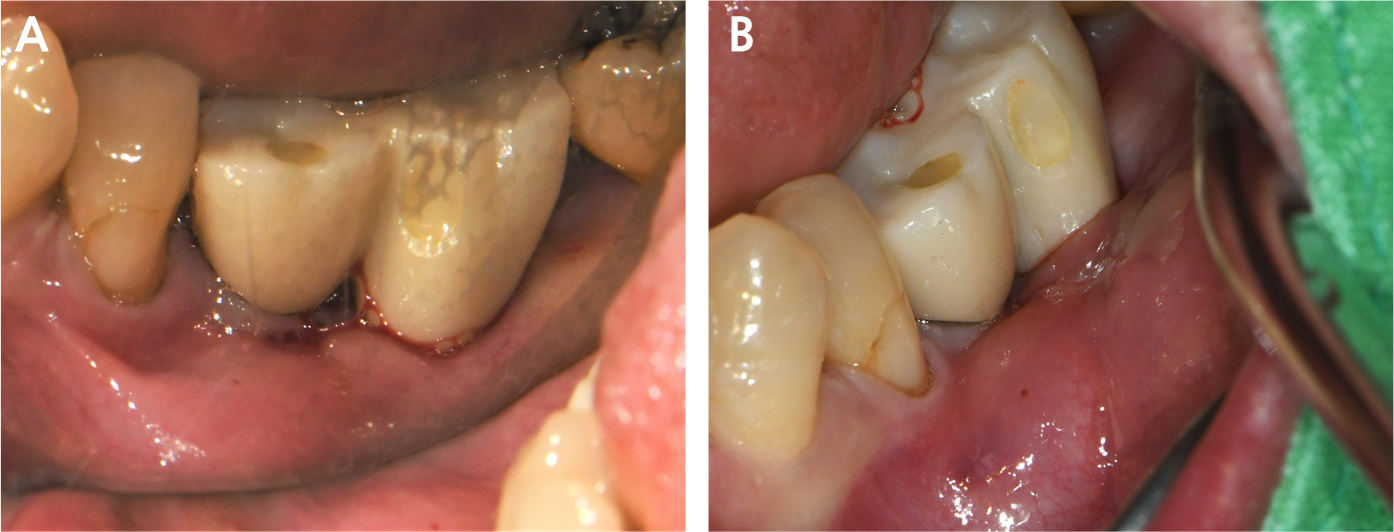
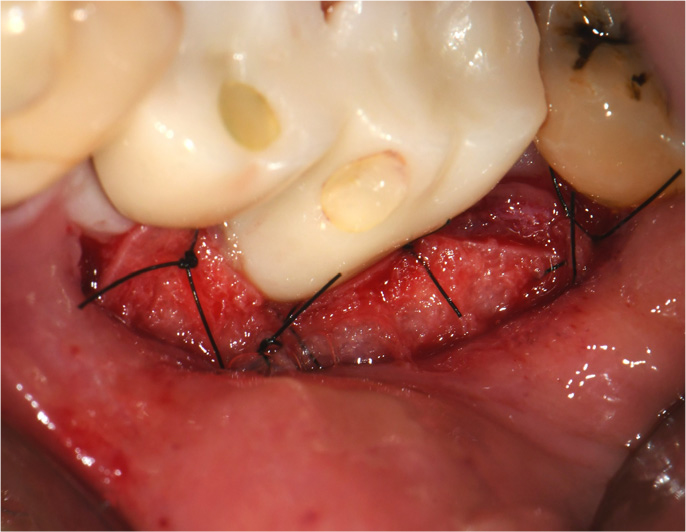
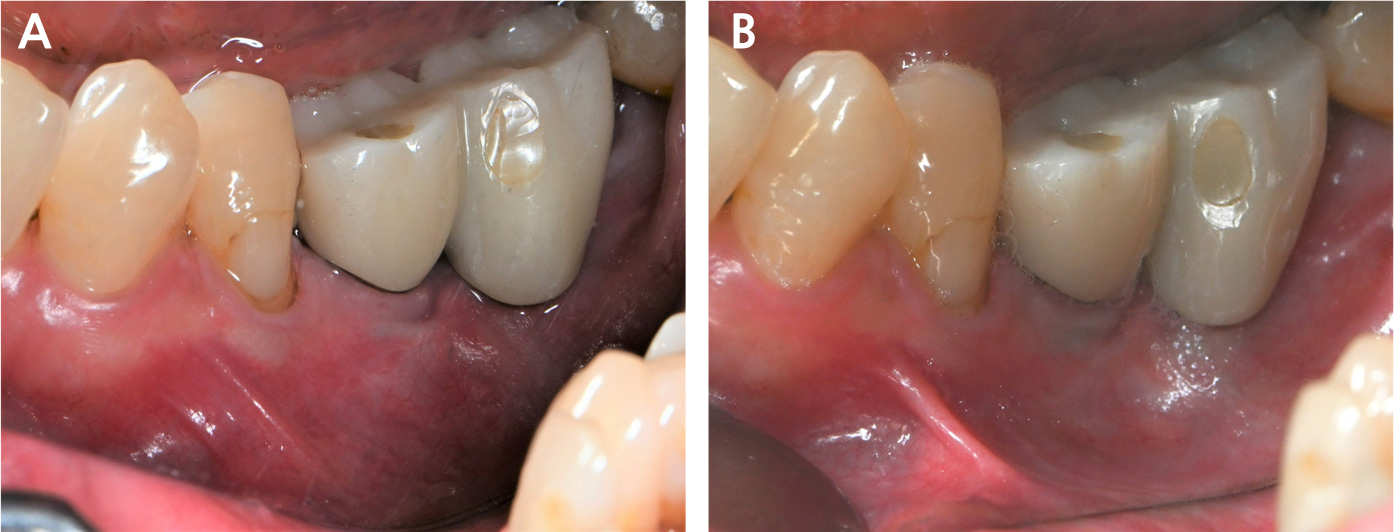
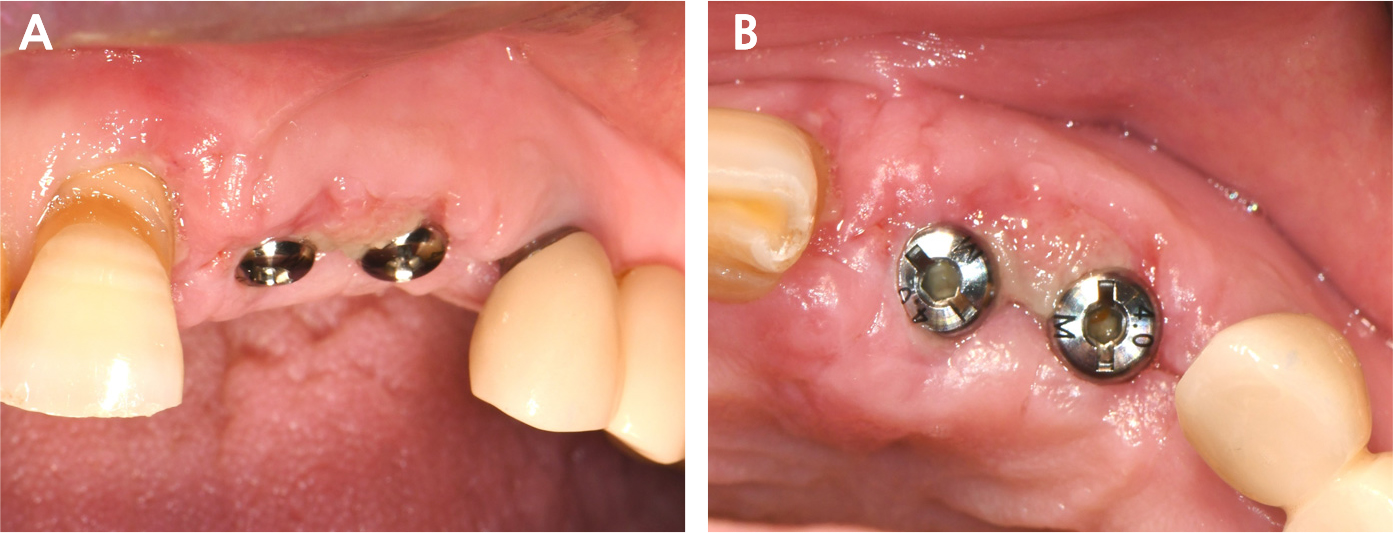
A 55-year-old female presented with recurrent swelling and pain around implants #35 and #36. Examination revealed no attached buccal mucosa, a shallow vestibule exacerbating muscle pull, and an 8 mm periodontal probing depth (PD) with swelling (Fig. 1). Under local anesthesia, a partial-thickness flap was positioned apically, preserving the underlying periosteum. A trimmed collagen matrix was placed over the exposed periosteum and secured with periosteal sutures (Fig. 2). Healing was uneventful. At 4 and 14 months, a clinically functional zone of the attached mucosa appeared to be maintained, accompanied by a reduction in PD from 8 mm to a stable 5 mm, resolving the inflammation (Fig. 3).
2. Case 2: Soft Tissue Augmentation
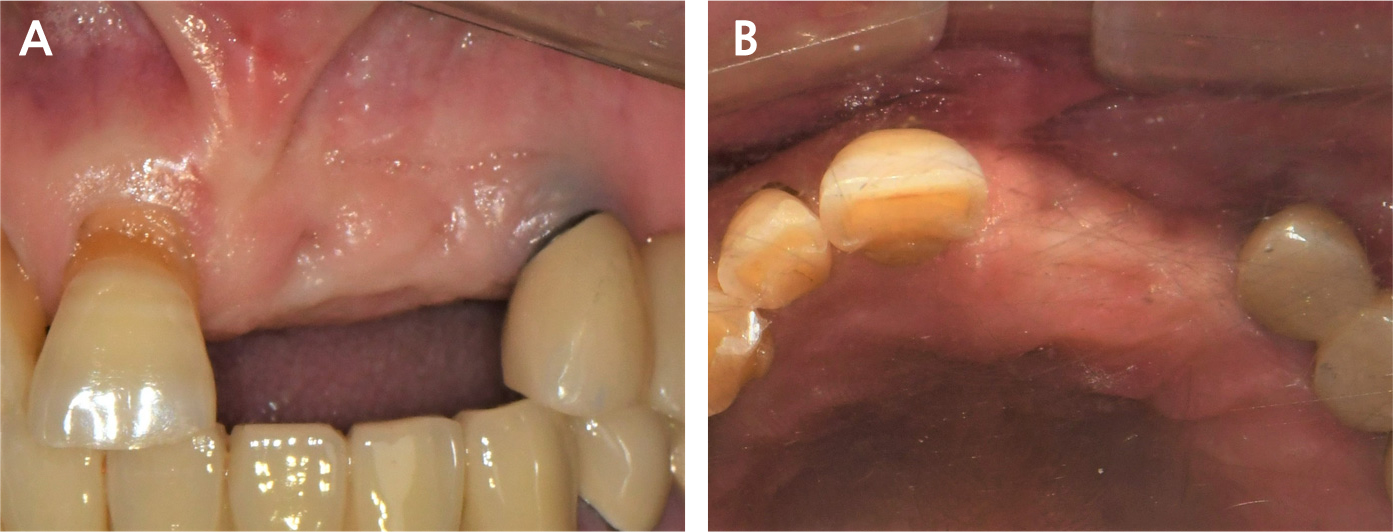
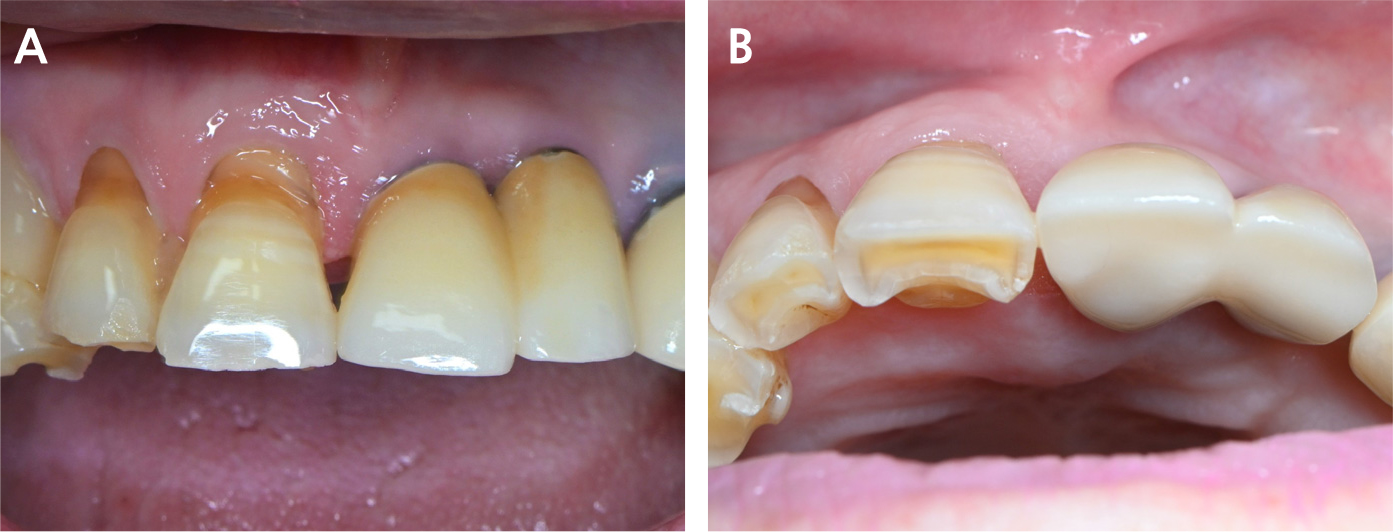
A 78-year-old female presented for restoring teeth #21 and #22. Loss of the edentulous soft tissue volume and labial bone resorption were also observed (Fig. 4). Following flap elevation and implant placement, the matrix was adapted between the labial bone and the flap for volume expansion, followed by primary closure. At 8 and 14 months, the site showed favorable remodeling. A descriptive clinical assessment based on the Pink Esthetic Score (PES) suggested a consistent score of 11/14 for implant #21, indicating volume maintenance without significant shrinkage (Figs. 5 to 7).10

3. Case 3: ARP
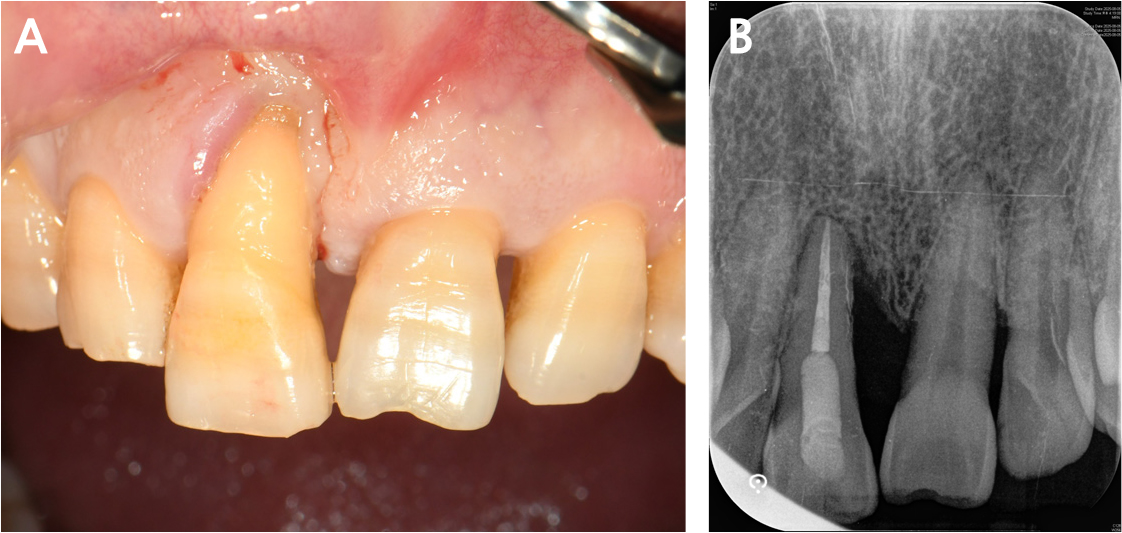
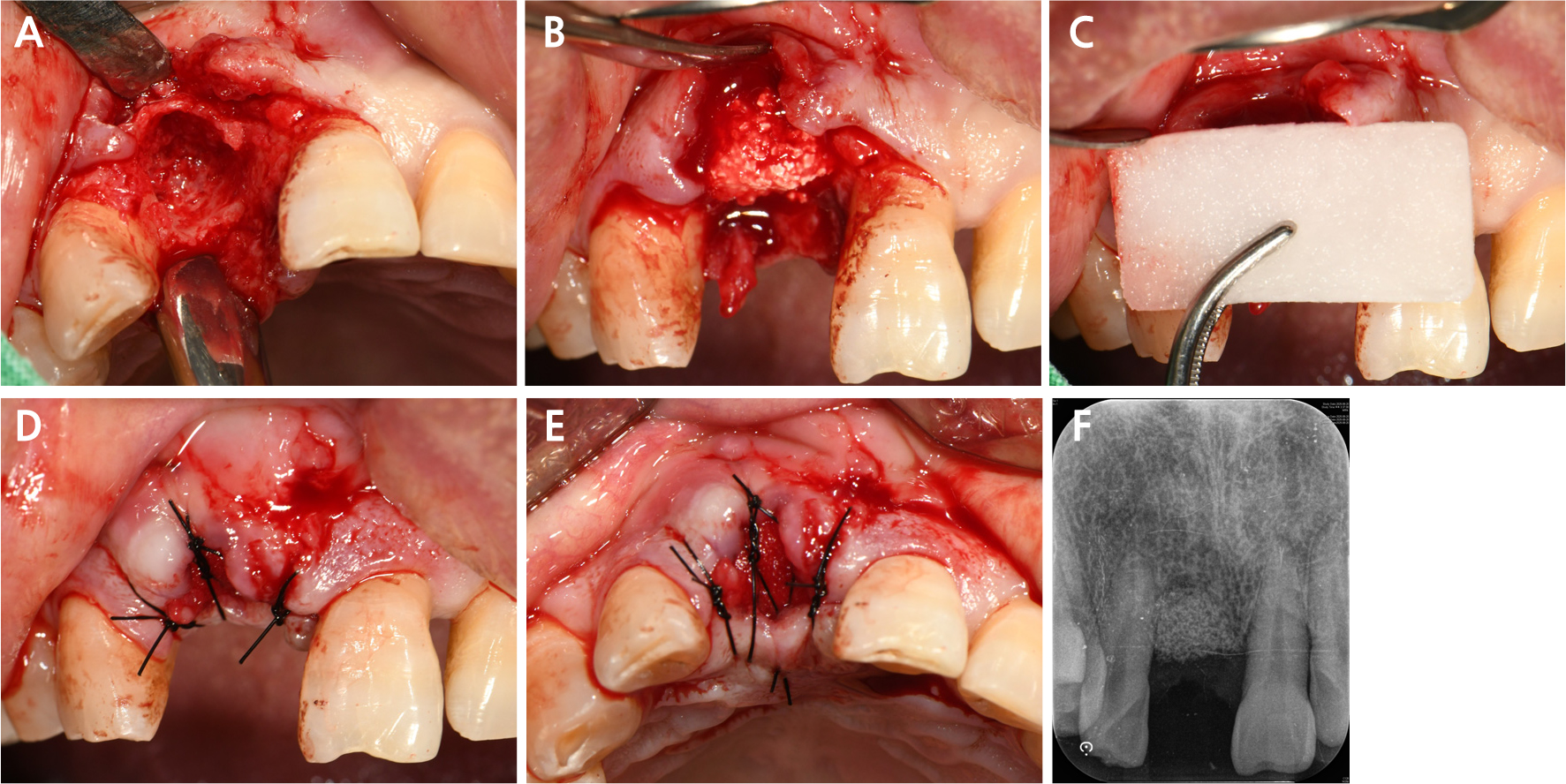
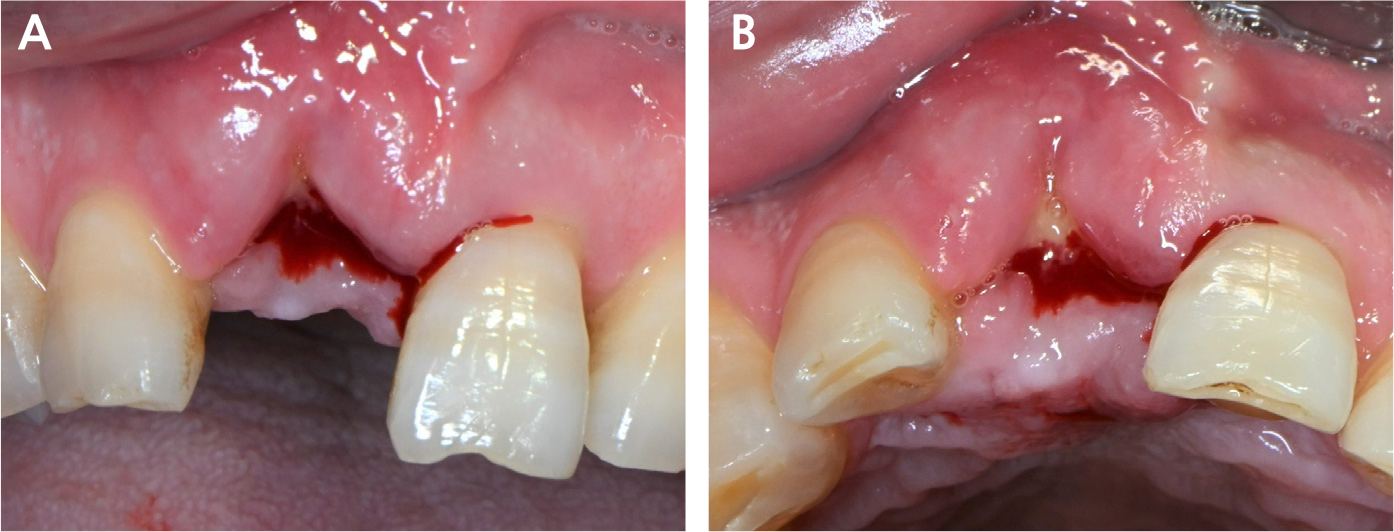
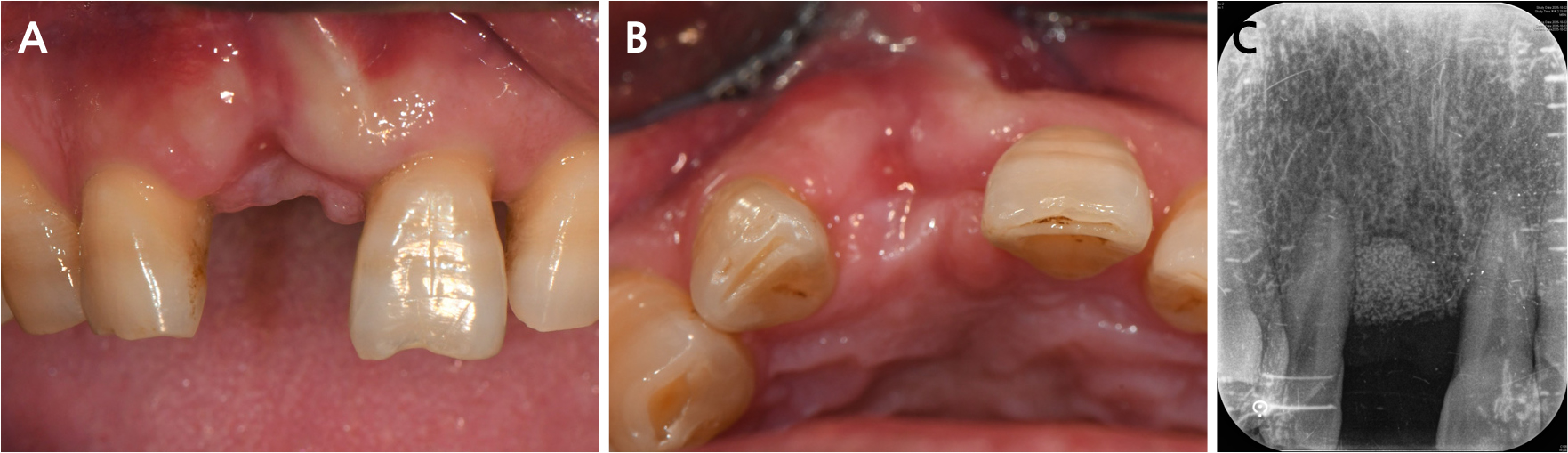
A 57-year-old male with a history of thyroid cancer presented with a hopeless tooth #11, showing severe labial attachment loss and suppuration (Fig. 8). ARP was performed after atraumatic extraction. An alloplastic bone substitute (Osteon 3 Collagen; Genoss, Suwon, South Korea) was packed into the socket (Figs. 9A and 9B). The collagen matrix was applied over the socket and secured using horizontal mattress sutures for open healing (Figs. 9C to 9F). At 2 weeks, progressive epithelialization was observed without infection (Fig. 10). At 2 months, mucosal closure was maintained. The clinical examination suggested satisfactory labial contour preservation (Fig. 11). Proportional radiographic measurements (calibrating the vertical graft height against the adjacent reference tooth) indicated a stable height-to-tooth ratio (70.6% at baseline and 73.3% at 2 months), suggesting favorable vertical ridge preservation (Figs. 9F and 11C).
Ⅲ. Discussion
This case series evaluated a porcine matrix (Collagen Graft x1D), composed of cross-linked type I collagen with a bilayer structure comprising a dense and a porous layer, across vestibuloplasty, soft tissue augmentation, and ARP. A major clinical advantage is the favorable initial healing and rapid epithelialization. Eliminating the donor site reduced morbidity.11
Clinical performance is influenced by the healing environment. In open healing (Cases 1 and 3), the matrix acted as a protective template to guide epithelial migration. In Case 1, although exact millimeter measurements of the mucosal width were not recorded, a clinically functional zone of the attached mucosa was maintained throughout the 14-month observation period. This stable tissue boundary neutralized the muscle pull, reducing the PD from 8 to 5 mm. This aligns with previous studies showing xenogeneic matrices can maintain vestibular depth and mucosal dimensions comparably to autogenous grafts.6 However, a biomechanical trade-off is that direct exposure to saliva and collagenases accelerates matrix dissolution during open healing.
Conversely, in closed healing (Case 2), the matrix was protected beneath a closed flap, stabilizing the initial blood clot and slowing enzymatic degradation. This protected integration allows for more predictable volume augmentation as a space binder. At this submerged site, a descriptive clinical assessment based on PES suggested a consistent score of 11/14 for up to 14 months, indicating acceptable volume retention without significant shrinkage.
Despite being chemically cross-linked–a modification generally intended to prolong volume stability and delay degradation–physical limitations inherent to its highly porous structure were clinically noted.12,13 The matrix exhibited rapid softening upon hydration, leading to decreased tensile strength and relatively fast postoperative absorption, particularly in open healing. This presents a biomechanical compromise: while high porosity maximizes early angiogenesis, it may still render the matrix susceptible to rapid structural collapse despite cross-linking.
The study limitations include the reliance on qualitative photographic evaluations without objective 3D volumetric measurements and omission of histological evaluations. Furthermore, given the small sample size and relatively short follow-up period, generalization of the long-term volume stability of the matrix requires further investigation.
Ⅳ. Conclusion
The porcine-derived collagen matrix appears to be a clinically feasible and less invasive alternative to autogenous grafts, minimizing patient morbidity. It shows biocompatibility, rapid epithelialization, and integration across diverse indications, providing satisfactory esthetic and functional soft tissue contours.
