

Ⅰ. Introduction
Maxillary sinus augmentation is a widely accepted and predictable procedure for implant placement in the atrophic posterior maxilla. Owing to alveolar bone resorption and sinus pneumatization, lateral sinus grafting has become an essential technique for achieving adequate bone height and implant stability. Over the past decades, various surgical approaches, grafting materials, and healing protocols have been introduced, resulting in considerable variations in clinical practice. Although numerous studies have reported favorable outcomes with both lateral and crestal approaches,1 standardized clinical guidelines remain lacking, particularly regarding procedural details and decision-making.
In Korea, several studies have investigated differences in implant survival rates based on surgical approach, particularly lateral versus crestal technique. One study showed that radiographic comparisons between the lateral and crestal approaches revealed no significant clinical difference in graft height gain over time.2 Another study reported that the lateral window technique achieved favorable bone healing even when using xenografts or synthetic bone alone, without the need for autogenous grafts.3
However, no study has focused on clinical consensus or standardized protocols specific to the lateral window technique. As most sinus augmentation surgeries are performed by oral and maxillofacial surgeons, understanding their clinical decision-making, grafting preferences, and treatment criteria is necessary to support evidence-based standardization and improve long-term outcomes.
Therefore, this study aimed to evaluate current trends and preferences among experienced oral and maxillofacial surgeons (with 10 years of clinical experience). By analyzing survey data from this group, this study sought to provide evidence-based insights and contribute to the development of unified clinical protocols for lateral sinus augmentation.
Ⅱ. Materials and Methods
This study was designed as a cross-sectional survey to assess clinical trends in lateral sinus augmentation among experienced oral and maxillofacial surgeons in Korea. A structured 12-item multiple-choice questionnaire was distributed electronically to 42 surgeons aged 36‒57 years, all employed at university hospitals with >10 years of clinical experience (Table 1).
The questionnaire evaluated clinical decision-making factors, including annual sinus grafts performed, preferred indications for the lateral window approach, instruments used, grafting materials, use of growth factors, timing of implant placement, and response to sinus membrane perforation. All participants voluntarily completed the survey, and responses were anonymized for analysis. Frequency distributions were calculated to summarize clinician preferences and practice patterns.

Ⅲ. Results
In total, 42 oral and maxillofacial surgeons participated in the survey (Fig. 1). Most respondents (66.7%, n=28) reported performing 1‒50 sinus graft procedures annually, while 33.3% (n=14) performed 51‒100 procedures. Regarding the residual bone height (RBH) at which clinicians initiated the lateral sinus approach, the most common threshold was 4 mm (n=15, 35.7%), followed by 3 mm (n=12, 28.6%) and 5 mm (n=7, 16.7%). Most clinicians (n=29, 69.0%) preferred using a low-speed carbide or diamond bur for lateral wall osteotomy; others reported using dedicated drills (n=8), piezoelectric devices (n=1), and high-speed burs (n=2). For implant placement with RBH <3 mm, 25 respondents (59.5%) performed simultaneous placement, whereas 17 (40.5%) preferred a staged approach. Xenografts were the most commonly used bone graft material (n=17), followed by allogeneic (n=12), synthetic (n=8), and autogenous (n=5) bones. Notably, 13 respondents selected “Mix,” indicating use of combinations of ≥ two graft materials, often xenografts combined with either allografts or autografts. Five clinicians reported using no graft in specific cases, likely when primary stability or natural bone formation was deemed sufficient. Use of BMP-2 or other growth factors was limited, with only six surgeons (14.3%) indicating routine use. The most common healing period before implant placement was 6 months (n=14), followed by 5 (n=5) and 3 (n=5) months. For sinus membrane perforations >1 cm, most surgeons opted to repair or proceed (n=19, 45.2%), whereas others decided case by case (n=8, 19.0%) and delayed surgery (n=15, 35.7%). To repair sinus membrane perforations, most surgeons used absorbable membranes (n=23), followed by fibrin gel (n=15) and sutures (n=4). The most commonly used implant type was the internal connection implant (n=28), followed by tissue-level implants (n=8) and others (n=6). Regarding smoking, 31 respondents (73.8%) performed surgery only after smoking cessation, six (14.3%) did not, and five (11.9%) advised stopping immediately before and after surgery. Regarding alcohol consumption, 18 respondents (42.9%) recommended abstinence around surgery, whereas 17 (40.5%) did not consider it crucial (Table 2).
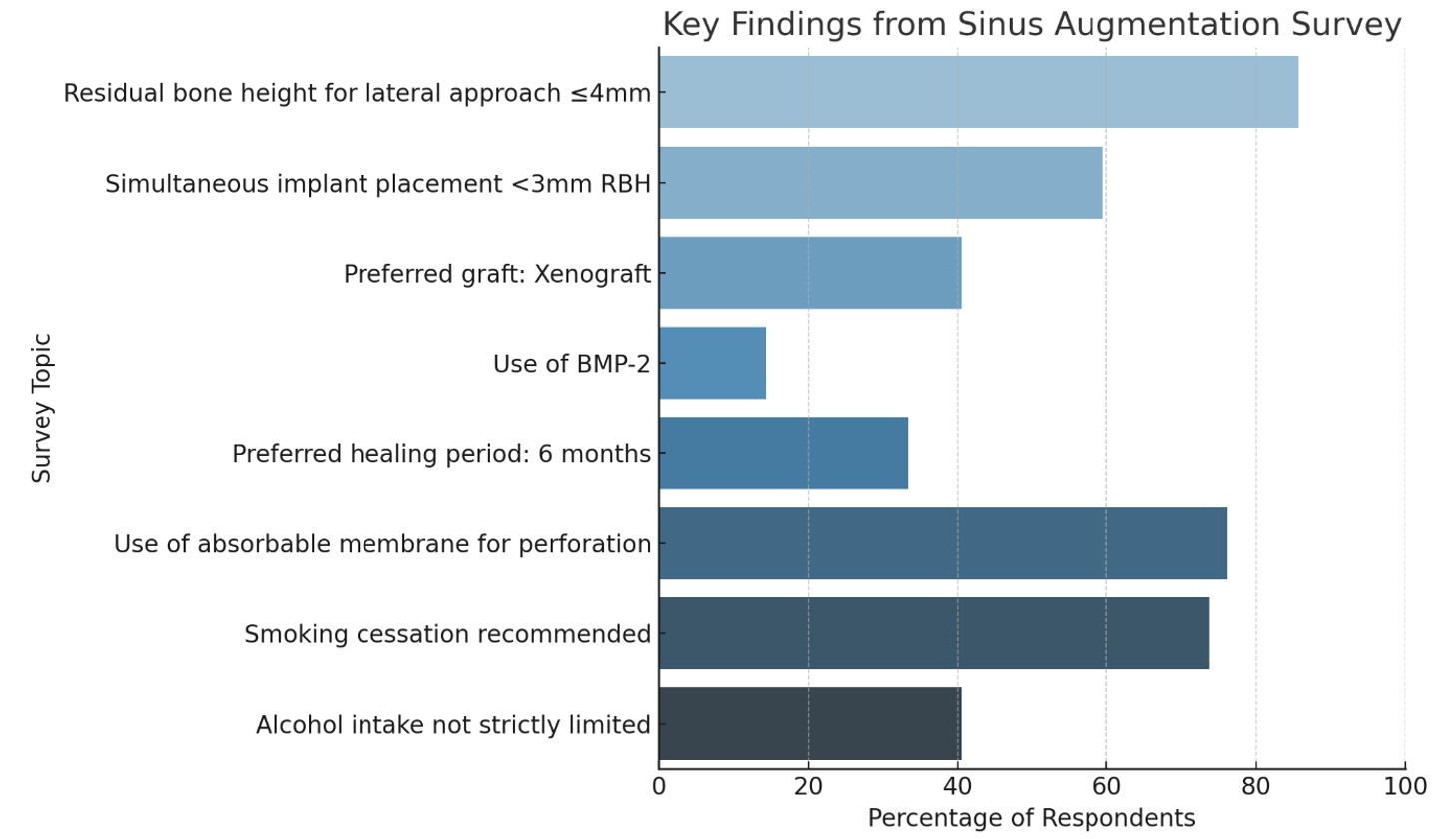
Table 2.
Results of the survey
Ⅳ. Discussion
Maxillary sinus augmentation is a well-established standard procedure for implant placement in the posterior maxilla when vertical bone height is insufficient. Although reported frequencies vary across studies, its use has steadily increased over the past decades, and it has become widely adopted in daily clinical practice. This is largely attributable to maxillary sinus pneumatization and alveolar bone resorption following tooth loss, both of which contribute to reduced bone height in the posterior maxilla, necessitating sinus grafting for successful implant placement.4 In this survey, most participants (66.7%) reported performing between 1 and 50 sinus grafts annually, while none performed >100. This reflects the procedural distribution among Korean oral and maxillofacial surgeons, suggesting that sinus grafting is moderately common but concentrated among surgeons with specific case volumes.
According to a recent study in 2023, the lateral sinus approach combined with simultaneous implant placement can be successfully performed even when RBH is <3 mm.5 Another study demonstrated that for RBH of 4‒5 mm, a staged approach beginning with a crestal sinus lift followed by a lateral window technique was feasible; in such protocols, the injection of only 0.3 mL of graft material during the initial stage resulted in an average vertical bone height gain of 6.7 mm.6 In this survey, many clinicians reported initiating the lateral sinus approach at 4 mm (35.7%), followed by 3 mm (28.6%) and 5 mm (16.7%). This reflects a clinical preference for a relatively conservative threshold, with most surgeons initiating lateral window access when RBH is < 5 mm. These findings indicate that experienced oral and maxillofacial surgeons in Korea tend to perform the lateral approach even in cases with less residual bone than that suggested by international consensus.
In the lateral approach for maxillary sinus elevation, various instruments such as straight handpieces with round burs, piezoelectric devices, and dedicated sinus lift kits (including diamond tips, chisels, and membrane elevators) are commonly used. Recently, piezoelectric devices and specialized kits have gained prominence for enhancing surgical safety and outcomes.7 However, low-speed carbide or diamond burs remained the most preferred instruments (69.0%), likely owing to their controlled cutting and minimal thermal damage. Although piezoelectric and dedicated drills have been used by some clinicians, they were less favored, possibly because of the increased time requirements or limited access.
Based on recent studies, simultaneous implant placement is generally recommended when RBH is ≥3 mm, though cases with 1‒2 mm may be considered based on the surgeon's experience, with reported success rates exceeding 95% in selected cases.5 Consistent with these findings, over half of the respondents (59.5%) in this survey placed implants simultaneously even when RBH was < 3 mm, reflecting either confidence in achieving primary stability or reliance on graft stability and technique. However, a considerable proportion of clinicians still preferred a staged approach, suggesting that clinical decision-making remains influenced by case-specific factors, anatomical limitations, and personal surgical philosophy.
In cases with RBH < 5 mm, the standard protocol involves combining xenograft with autogenous bone to support new bone formation.5 Histological studies have shown that new bone typically begins forming along the walls of the maxillary sinus and gradually extends toward the implant surface, underscoring the importance of graft materials that facilitate osteoconduction.8 In this survey, xenografts were the most frequently selected material (40.5%), followed by allografts and synthetic substitutes, often used in combination. This reflects global clinical trends favoring xenografts for their biocompatibility, slow resorption rates, and structural stability. In contrast, no clinicians selected autografts alone, suggesting they are typically combined with other materials. This preference may reflect a strategy to leverage the osteogenic potential of autogenous bone while compensating for its limited volume and associated surgical burden through combination grafting. These findings indicate that although clinicians recognize the biological advantages of autografts, practical and procedural factors drive the routine use of mixed grafting approaches in lateral sinus augmentation.
In cases where BMP-2 was used, implant placement was successful even with as little as 3 mm of residual bone, achieving a survival rate of 98.4%.9 Implant placement could be performed as early as 18 weeks post-grafting, compared to the traditional 24-week healing period (6 months).10 The main reported side effect was transient postoperative edema, likely related to pro-angiogenic and vascular- permeability-enhancing effects of BMP-2.8 Despite this potential, only a few clinicians (14.3%) reported using BMP-2 or similar growth factors in practice, indicating limited adoption, possibly due to factors such as high cost, regulatory restrictions, or the absence of robust evidence supporting routine use. These results suggest that clinicians should adopt a cautious approach when considering the application of biologics in sinus augmentation.
A meta-analysis has demonstrated that implant survival rates do not differ significantly when implants are placed after a healing period of 4‒6 months, regardless of the graft material used, including autografts, xenografts, or synthetic substitutes.11 In this survey, the preferred healing period was 6 months (33.3%), consistent with conventional protocols for sinus augmentation. However, the variability observed in healing preferences reflects differing clinical opinions on graft maturation timelines, likely influenced by factors such as the surgeon's experience, choice of graft material, and patient-specific considerations, including bone quality and healing capacity.
Several studies have addressed clinical protocols for managing sinus membrane perforations, including the use of collagen membranes for repair. A study comparing cases with and without membrane repair during maxillary sinus membrane perforation found that failure to repair significantly increased the need for postoperative interventions, including antibiotic prescription (11.3% vs. 1.4%) and additional bone grafting procedures (11.3% vs. 3.4%).12 Clinicians were categorized based on their responses to large membrane perforations. Although 45.2% chose to repair and proceed, 35.7% opted to abort the procedure. This variation highlights the lack of standardized protocols and underscores the importance of intraoperative judgment.
Small sinus membrane perforations (<5 mm) may heal spontaneously; however, restoration using a collagen membrane is generally recommended to prevent the influx of bone graft materials. For medium-sized perforations (approximately 5‒10 mm), clinicians may employ reinforcement techniques, such as covering the defect with a collagen membrane and securing it using titanium pins to ensure membrane stability and prevent graft migration. This technique effectively prevents graft material leakage while promoting mucosal regeneration.13 For large perforations (>10 mm) or complete mucosal defects, a combination of repair techniques may be required—including layered collagen membranes, autologous soft tissue (such as palatal connective tissue or buccal fat pad), suturing, block grafts, or staged reoperation after initial closure.14 Absorbable membranes were the most commonly used material (54.8%), often combined with other methods such as fibrin glue or suturing. These practices reflect current consensus on membrane regeneration and stabilization techniques, emphasizing biocompatibility and ease of application.
Most clinicians preferred internal connection implants (66.7%), reflecting their popularity in terms of stability and long-term success. The relatively low use of tissue-level and other implant types may reflect clinicians' training background or manufacturer preference. However, to date, no studies have specifically addressed the clinical outcomes or differences between internal and external connection implants in the context of maxillary sinus augmentation, indicating the need for further research to clarify whether implant connection type influences success in this surgical setting.
Implant survival rates decrease significantly in heavy smokers, particularly those who smoke >15 cigarettes per day, following lateral sinus augmentation. In cases where residual bone height is <4 mm, smokers face a 3.8-fold increased risk of implant failure compared to non-smokers.15 Reflecting this clinical risk, most surgeons in this survey (73.8%) required patients to cease smoking before surgery, demonstrating a high level of awareness regarding the negative impact of smoking on graft integration and postoperative healing. However, some respondents adopted more lenient protocols, suggesting differing beliefs about the short-term consequences of smoking on implant success.
Alcohol consumption, alongside smoking, is a lifestyle-related risk factor that negatively affects bone regeneration. Studies have shown that alcohol intake significantly reduces vital bone formation, with alcohol-consuming groups demonstrating a 23% decrease in new bone formation and delayed resorption of residual graft material during the osseointegration phase compared to non-drinkers. However, no significant difference in implant survival rates was observed at the 2-year follow-up, suggesting a limited long-term impact.16
In this survey, clinicians' responses regarding alcohol intake were more evenly distributed. Although 42.9% of clinicians recommended abstinence before and after surgery, 40.5% did not consider alcohol a significant risk factor. This variation in clinical opinion highlights the need for further research and continuing education regarding the nuanced effects of alcohol on graft healing and implant outcomes.
In this study, several meaningful correlations were identified among the questionnaire items, suggesting clinical decision patterns among experienced oral and maxillofacial surgeons in Korea. First, a moderately positive correlation was observed between the type of graft material used and the healing period before implant placement. Surgeons who used a greater variety or combination of grafting materials tended to adopt longer healing periods, potentially reflecting a more cautious approach when using composite or synthetic grafts, where slower or more complex bone maturation is anticipated. In addition, a noticeable correlation existed between the instrument used for lateral wall osteotomy and graft material. This suggests that the choice of instrumentation, such as low-speed burs or piezoelectric devices, may influence or reflect grafting preferences. Clinicians who favor minimally traumatic cutting techniques may also prefer materials that promote more predictable healing. Interestingly, the use of BMP-2 or growth factors showed minimal correlation with other variables, suggesting that the decision to use biologics may depend more on individual surgeon philosophy or institutional access than on procedural factors. Overall, these relationships indicate that while certain procedural decisions are interconnected—particularly those involving graft material and healing strategy—others are more isolated. Understanding these decision-making clusters can help guide standardized protocols and inform future clinical recommendations.
Ⅴ. Conclusion
This survey of 42 experienced oral and maxillofacial surgeons in Korea revealed key trends and variations in lateral sinus augmentation. Most clinicians initiated the lateral approach at RBH ≤4 mm, and over half placed implants simultaneously, even when bone height was <3 mm. Xenografts were the most preferred graft material, whereas autografts were typically used in combination. The use of BMP-2 was limited, despite supportive clinical evidence. A 6-month healing period was most commonly adopted, and membrane perforation was mainly managed with absorbable membranes. Most clinicians emphasized smoking cessation, while opinions regarding alcohol intake varied.
These survey findings suggest that Korean oral and maxillofacial surgeons tend to favor minimizing the number of surgical stages by performing simultaneous implant placement, even with <3 mm of residual bone, especially when using xenografts. In addition, although attitudes toward alcohol appear relatively lenient owing to cultural factors, smoking cessation is strongly recommended. These trends reflect the evolution of surgical approaches within established protocols and highlight the importance of individualized treatment planning. Furthermore, to develop a more comprehensive consensus, future studies should include not only oral and maxillofacial surgeons but also practitioners from various dental specialties who perform sinus augmentation procedures.
