

Ⅰ. Introduction
Ⅱ. Materials and Methods
1. Study Design
2. Sample Selection
3. Computer-guided Implant Surgery
4. Questionnaire
Ⅲ. Results
1. Demographic Results of Patients
2. Demographics Results of Surgery
3. Results of the Survey
Ⅳ. Discussion
Ⅴ. Conclusion
Ⅰ. Introduction
Technology of dental implant has substantially developed ensuring the implant survival rate from approximately 80% in the 1980s up to 99% currently.1,2 As a result, implant penetration has increased, and the importance of long-term success has been underlined not only for implant survival but also for fewer complications. To reduce complications, not only basic patient oral hygiene and periodic check-ups but also avoiding implant mal-positioning to fabricate an adequate implant prosthesis are important.3
Originally, implant positioning and angulation have depended entirely on the individual clinician's spatial ability and clinical experiences. Several computer software programs have been developed since the late 1980s as part of an effort to accurately place implants according to the planned position, angulation, and depth.4 When implant guide systems such as Simplant (Dentsply Sirona, Charlotte, NC, USA) and Nobelguide® (Nobel Biocare, Gothenburg, Sweden) were first introduced in the early 2000s, such systems presented with high production costs and difficulties in the preparation process. With the development of software and three-dimension (3D) printing technology, several implant guide systems have been developed and studied.5 According to a previous study on the accuracy of the template for implant surgery fabricated with the milling machine, the coronal deviation, apical deviation, and angular deviation of the implant were 0.31 ± 0.09 mm, 0.36 ± 0.10, and 1.62 ± 0.75° (mean ± SD), respectively. Implant guide surgery with the template by milling has a degree of accuracy suitable for implant placement.6 A study reported that the guide system was more accurate than free-hand implant placement in terms of mean coronal deviation (0.9 mm vs. 2.4 mm), mean apical deviation (0.6 mm vs. 2.4 mm), and mean angular deviation (4.2° vs. 9.8°) (p < .05).7
Fontin et al.8 established the concept of computer-guided surgery (CGS). Based on the autonomy given to the surgeon, they classified CGS into passive, semi-active, and active types. Currently, the most widely used type is the semi-active CGS. A similar classification, including static, dynamic, and robotic CGS according to the degree of computer intervention, was suggested by Park et al.5 The static CGS can be further subdivided into a fixed sleeve and a non-sleeve for guiding drills and fixtures, or additive manufacturing using 3D printing and subtractive manufacturing using a milling machine.9
The conventional steps of surgical template fabrication in static CGS consist of 1) 3D scanning of the mouth (intraoral) or the plaster model made by pouring the impression, 2) cone-beam computed tomography (CBCT) imaging of the future implant site, 3) registration of the 3D reconstructed CBCT image and scan image, 4) implant positioning and template design using virtual planning software, and 5) template fabrication via 3D printing. Although static CGS has the advantage of obtaining accurate surgical results,10 it is difficult to register the CBCT image with the scanned image. Errors can be accumulated in the process of impression, scanning,11 image registration, and 3D printing, which can negatively affect the fitness of the printed template.12 Model-free, and zero-setup static CGS system (VARO Guide®; Neobiotech, Seoul, Korea), had simplified steps. The first step was replaced by intraoral adaptation and light-curing of the surgical template (PreGuide) filled with light-cured resin. In the second step, CBCT is taken with the an occluded template. Since six radiopaque markers are embedded in the PreGuide and captured in the CBCT images, the template position can be simply registered with minimal error. In addition, owing to the simpler steps compared to the conventional CGS system, it can be more helpful to complete the diagnosis, template fabrication, and implant placement in one visit.
The purpose of this study was to evaluate the surgeon’s satisfaction with the software’s ease of use, accuracy, template production process, and subjective template accuracy and ease of surgery through questionnaires for surgeons who have applied the VARO Guide® CGS system.
Ⅱ. Materials and Methods
1. Study Design
A survey was conducted among surgeons who used the CGS system between June 2020 and January 2021 at the Department of Periodontology, Dankook University Dental Hospital (DKUDH IRB 2022-10-008).
2. Sample Selection
Patients eligible for implant placement were selected through the following inclusion and exclusion criteria.
Inclusion criteria were the following:
・Patients over the age of 18
・Patients who had undergone tooth extraction more than three months prior
・Patients who agreed to place the implant using the CGS system
・Patients with bone height ≥ 8 mm from anatomical structures (e.g., maxillary sinus and inferior alveolar nerve)
Exclusion criteria were the following:
・Patients with uncontrolled systemic disease contraindicated for oral surgery
・Pregnant women
・Patients with poor oral hygiene
3. Computer-guided Implant Surgery
1) Tray adaptation and CBCT imaging
First, one of the following three types of PreGuide, a polycarbonate ready-made tray filled with light-cured resin with radiopaque markers, was selected according to the following implant sites: maxillary right/mandibular left, maxillary left/mandibular right, and anterior regions. The inner surface of the tray was covered with a polyvinyl membrane to prevent the formation of an undercut of the resin during light-curing. In the initial try-in state, the tray was light-cured in the buccal and palatal directions. To enhance the fit, the inner surface of the template was relined by adding a light-curing resin and light-curing it after removing the membrane. CBCT (Alphard 3,030 3D CT scanner; Asahi Roentgen Industries, Kyoto, Japan) was taken with biting the trays.
2) Preparation of surgical templates
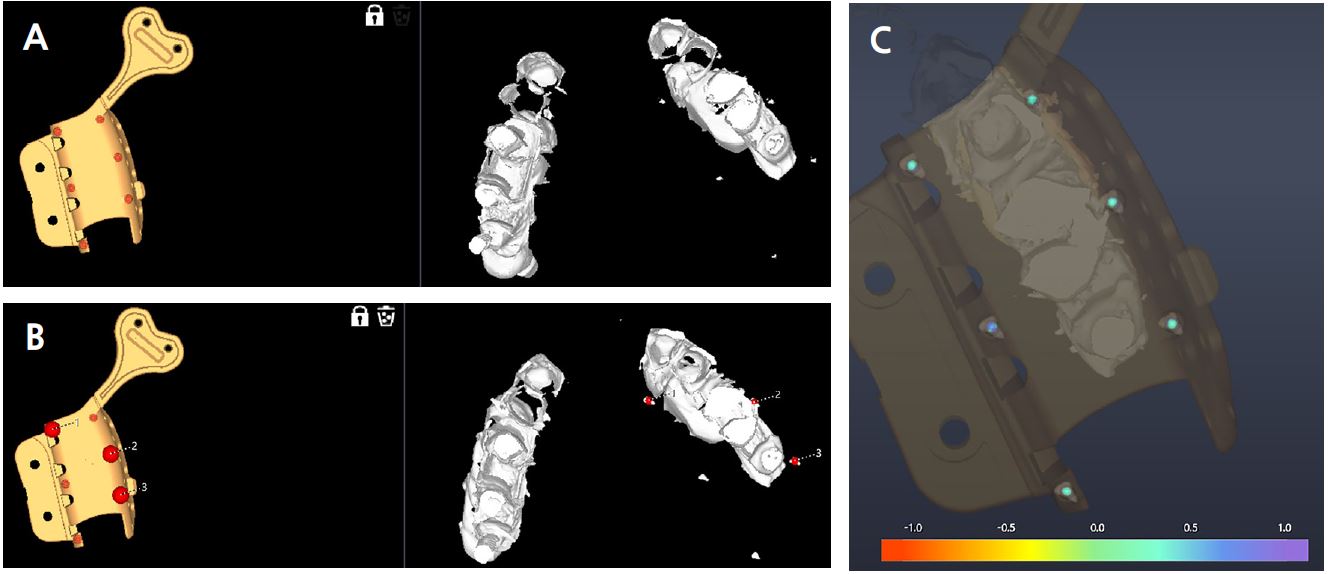
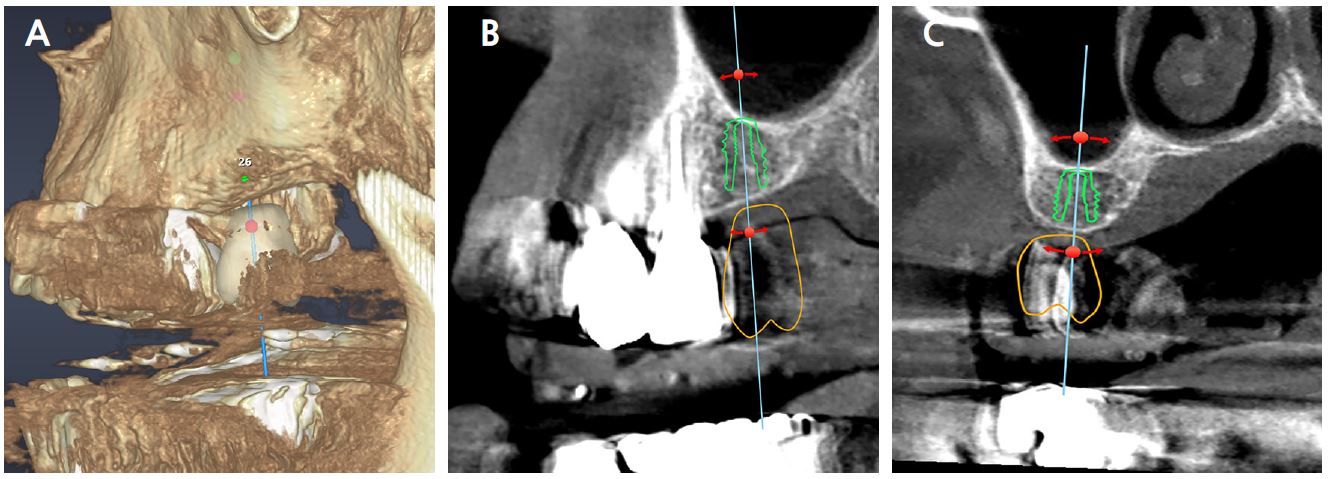
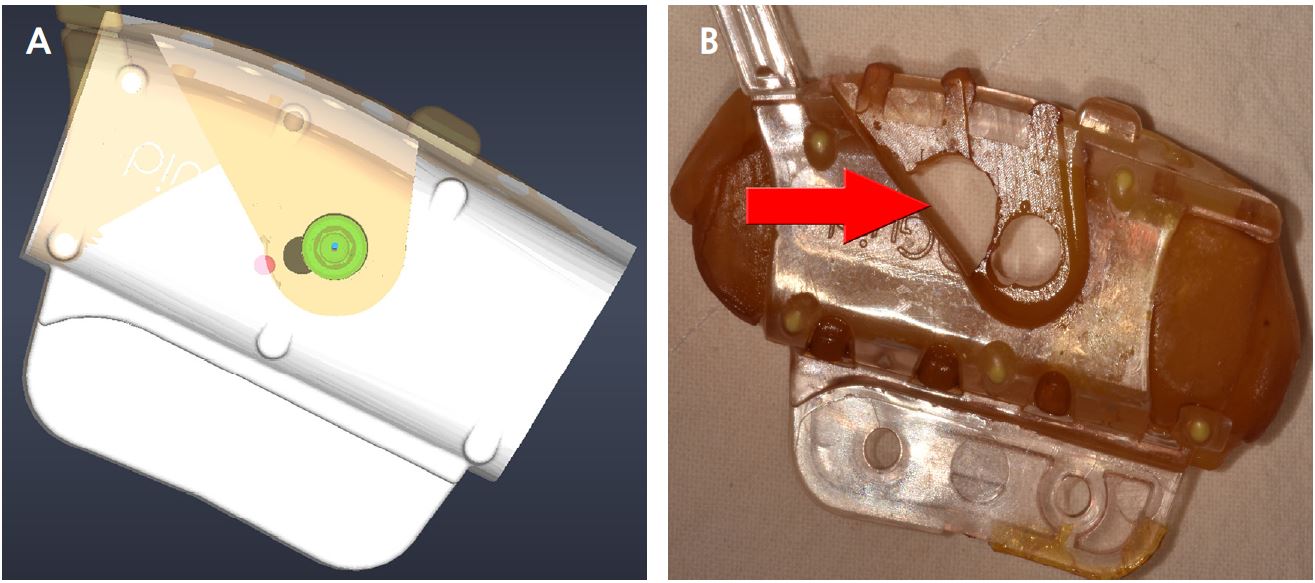
The implant planning software (VARO Plan; Neobiotech, Seoul, Korea) can register the CBCT raw file and the Digital Imaging and Communications in Medicine (DICOM) file. The 3D tray image can be located on the 3D reconstructed CBCT by marking the positions of three or more radiopaque markers captured in CBCT (Fig. 1). The final position of the implant was determined after simulating the fixture position, which considered the anatomical structures and shape of the prosthesis (Fig. 2). The 3D images of PreGuide with a drill hole (non-sleeve), irrigation hole, and vertical stop for the implant’s vertical position were converted into standard tessellation language (STL), an international standard data file format that represents 3D objects. The surgical template was fabricated by boring the PreGuide hole according to the STL file using a milling machine (VARO Mill; Neobiotech) (Fig. 3).
3) Implant placement using the surgical template
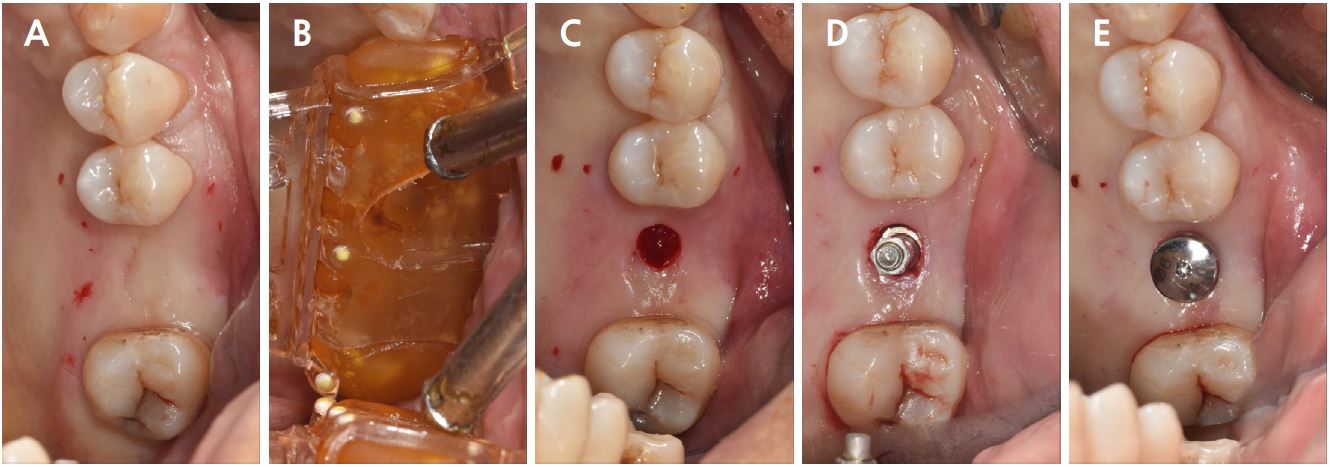
Depending on the presence of dehiscence or fenestration after planned implant location, the need for ridge augmentation procedure, the surgeon decided whether the flap should be elevated. If the surgeon planned to elevate the flap, the surgical template was adapted after elevating the flap. If flapless surgery was planned, the soft tissue covering the future implant site was removed using a tissue punch, after adapting the guide without elevating the flap. Osteotomy was performed using a CGS-specified drill kit, with a drill base fitted to a non-sleeve hole. The implant was placed using the adapted template (Fig. 4).
4. Questionnaire
A survey was conducted according to the number of templates used instead of the number of implants placed. The questionnaire consisted of 15 questions to evaluate convenience and accuracy in the planning and surgical stages of CGS. For each question group with the same number of choices, internal consistency was evaluated using Cronbach's α.
Ⅲ. Results
1. Demographic Results of Patients
The patients consisted of six men (54.5%) and five women (45.5%) with a mean age of 59.1 years. Most implants were placed in the maxilla (Table 1).
Table 1.
Demographic results of patients
2. Demographics Results of Surgery
A total of six surgeons participated in the questionnaire after the surgery: one patient was treated by a faculty member with more than eight years of clinical experience, and two 3rd-, one 2nd-, and two 1st-year residents treated a total of 11 patients and placed 16 implants using the CGS system (Table 2).
Table 2.
Demographic results of surgery
3. Results of the Survey
1) Planning process
Regarding the question about the convenience of the process of importing the CT DICOM file into the planning software, “very convenient” was the highest at 54.5% and “neutral” and “lightly convenient” were 27.3% and 18.2%, respectively. When asked about the convenience of the process of registering CT data and PreGuide in the planning software, “slightly convenient” was the highest response at 54.5% and “very convenient” was 36.4%. The answers to the accuracy of registering the CT data and the PreGuide were “very accurate” and “slightly accurate”, respectively, with 45.5 %. Regarding whether a temporary prosthesis was needed, 36.4% answered that it was necessary. Concerning the question about the convenience of the milling process, “neutral” ranked highest with 54.5% (Table 3).
Table 3.
Result of survey
| Domain | Question | Answer expressed in n (%) | ||||||||
|
Very inconvenient |
Slightly inconvenient | Neutral |
Slightly convenient |
Very convenient | ||||||
|
Planning process | 1 |
Is the process of importing the CBCT DICOM file into the planning software (VARO Plan) convenient? | 0 (0%) | 0 (0%) | 3 (27.4%) | 2 (18.2%) | 6 (54.5%) | |||
| 2 |
Is the process of matching CBCT DICOM file and PreGuide convenient? | 0 (0%) | 0 (0%) | 1 (9.1%) | 6 (54.5%) | 4 (36.4%) | ||||
| 3 |
Is the process of matching CT DICOM file and PreGuide correct? |
Very inaccurate 0 (0%) |
Slightly inaccurate 0 (0%) |
Neutral 1 (9.0%) |
Slightly accurate 5 (45.5%) |
Very accurate 5 (45.5%) | ||||
| 4 |
Is it convenient to locate or modify the implant in the planning software? | 0 (0%) | 0 (0%) | 1 (9.1%) | 3 (27.3%) | 5 (45.5%) | ||||
| 5 |
Did this case need immediate loading using a temporary prosthesis? |
Yes 4 (36.4%) |
No 7 (63.6%) | |||||||
| 6 |
How about the convenience of the milling process by converting the NC file* (3D file)? | 0 (0%) | 0 (0%) | 5 (45.5%) | 6 (54.5) | 0 (0%) | ||||
|
Operation process | 7 |
What is the level of fitness after the template is adapted? |
Insufficient gap 0 (0%) |
Adequate gap 8 (72.7%) |
Excessive gap 3 (27.3%) | |||||
| 8 |
What is the degree of movement of the template during drilling? |
No movement 6 (54.5%) |
Neutral movement 3 (27.3%) |
Severe movement 2 (18.2%) | ||||||
| 9 | How is the fitness in the sleeve of the template? |
Insufficient gap 0 (0%) |
Adequate gap 11 (100%) |
Excessive gap 0 (0%) | ||||||
| 10 |
Is it possible to change the surgical plan depending on the situation during the surgery? (Example: length, diameter, depth of the implant) |
Yes 11 (100%) |
No 0 (%) | |||||||
| 11 |
How about the amount of coolant through the irrigation hole during implant placement? |
Very excessive 0 (0%) |
Slightly excessive 0 (0%) |
Neutral 6 (54.5%) |
Slightly insufficient 5 (45.5%) |
Very insufficient 0 (0%) | ||||
| 12 |
How about the ease of insertion and removal of the drill into the sleeve? | 0 (0%) | 0 (0%) | 6 (54.5%) | 5 (45.5%) | 0 (0%) | ||||
| 13 |
What is the effect of the space constraint due to the template volume caused by the application of the guide system on surgery? | 0 (0%) | 5 (45.5%) | 2 (18.1%) | 4 (36.4%) | 0 (0%) | ||||
| 14 |
If an additional bone graft is required after guide surgery, how is the convenience of the GBR† | 0 (0%) | 0 (0%) | 3 (27.3%) | 2 (18.2%) | 6 (54.5%) | ||||
| 15 |
How was subjective feeling about the operation result compared to the initial plan? |
Very inaccurate 0 (0%) |
Slightly inaccurate 0 (0%) |
Neutral 2 (18.1%) |
Slightly accurate 4 (36.4%) |
Very accurate 5 (45.5%) | ||||
2) Surgical procedure
When questioned about the fitness after the template was installed, 72.7% answered that the fitness of the template was “adequate”. When asked about the movement of the template during drilling, 54.5% of the participants answered that there was “no movement”. All participants answered that the clearance between the sleeve and the drill was “adequate”. They replied that it was possible to change the length and diameter of the implant according to the clinical situation during surgery. The opinion regarding the amount of coolant through the irrigation hole was “insufficient” during implant placement, accounting for 45.5% of the responses. The opinion that the process of inserting and removing the drill from the sleeve is “very convenient” was 54.5%. Of the respondents, 54.5% answered the question about how much the volume caused by the template application had a restriction on the surgery as “very convenient”. When asked about the convenience of performing an additional bone graft after CGS, 54.5% answered that it was “very convenient”. When asked about the subjective feeling of the operation result compared to the initial plan, approximately 91.9% answered that it showed “high accuracy” (Table 3).
The Cronbach's α for questions 1−4, 6, and 11−15 with five choices was 0.614, and that for questions 7−9 with three choices was 0.622.
Ⅳ. Discussion
The purpose of this study was to evaluate and investigate the convenience, accuracy, and actual usability of implant planning software and placement with surgical templates using the model-free, zero-setup CGS system by surveying the surgeons. Satisfaction with the accuracy and convenience of locating the tray on CBCT data using the planning software was high, and the ease of use and post-implantation accuracy using the VARO Guide® were high.
The Cronbach's α value, which determines the internal reliability of the questionnaire answers, can be calculated for questions with the same number of choices. The α value of questions 7, 8, and 9 with three choices was 0.622, which can be considered reliable. The α value of the remaining items with five choices was 0.614, which can be considered reliable.
Most of the answers to the questions on convenience and accuracy in the planning process scored above “neutral”. The method of existing planning software involves the registration of the CBCT image (DICOM file) and intraoral scan image. In this process, some systems permit manual fine-tuning of registration results, but some use a method of forcibly aligning to each image’s surface, that is surface-based registration. In contrast, the VARO Guide® does not require an impression model or intraoral scanned image for registration with CT. It registers the tray location using three of the six points embedded in the tray and landmark-based registration. Unlike the conventional CGS system, it is considered that a high score was obtained in terms of convenience and accuracy because it was not aligned with the average value of the crown and CBCT of the remaining teeth.13 When comparing the surface-based method to landmark-based method (X-ray template), it was found that landmark-based method was statistically and significantly accurate with negative errors of −0.220 and −0.179, respectively.14
However, there is an inherent error owing to the resin in the PreGuide that exists only in the VARO Guide®. Resin exhibits polymerization shrinkage. Since the resin contained in the PreGuide was positioned at the future implant site to obtain an impression and then light-cured outside the oral cavity, shrinkage may occur on the inner surface of the template. Therefore, errors in template fabrication may occur because of errors in PreGuide adaptation while performing CBCT.15
When asked about the convenience of locating or modifying implants, 63.6% answered that it was “very convenient”. If the implant plan needs to be modified, additional communication with a lab engineer using a call or video conference is required since the surgical template of a conventional CGS system is fabricated by the manufacturer’s lab. However, the CGS system used in this study seems to have a high score because the surgeon can directly modify the virtual implant position on the planning software.
Not only does CGS simplify implant surgery, it also has the advantage of immediate loading after implantation.16 Furthermore, 36.7% of the surgeons answered “yes” to the question of whether it was a case requiring immediate loading. As the VARO Guide® does not involve conventional or digital model fabrication, it is impossible to fabricate a temporary prosthesis through 3D printing. Compared to other guide systems, the disadvantage of the VARO Guide® is the absence of immediate loading by 3D printed prosthesis.
The surgical template can be manufactured using 3D printing or milling. A previous study that compared the 3D printing method (Osstem Guide; OSSTEM, Seoul, Korea) and the milling method Navisis (EZPlant, Goyang, Korea) reported that the milling method showed low position, angulation, and depth deviation.6 Additionally, when asked about the convenience of the milling process, 54.5% answered that it was “slightly convenient”. The milling-type template fabrication method that VARO Guide® chose can be considered high in terms of both accuracy and convenience.
Since the VARO Guide® makes a template using the impression of teeth and oral mucosa obtained from resin, it has higher suitability compared to the existing template using 3D printing; therefore, no additional adjustment is required in the oral cavity after milling. This can reduce the number of patient visits and the accuracy of the implant, which matches the planned implant’s position, angulation, and depth.17
The surgeon's level of expertise in implant placement did not influence the level of satisfaction arising from the use of VARO Guide®. Rather than the level of experience, there was a difference in satisfaction according to the difficulty level of implant placement in the patient and whether the flap was elevated. A previous study comparing the accuracy between experts and beginners using the VARO Guide® in the previous model showed similar results, with no significant difference in accuracy and surgery time between experts and beginners.18
Another previous study showed that the effect of flap elevation on accuracy in guide system surgery is not statistically significant.19 However, the fit of the template decreases due to flap elevation, which may cause discomfort, such as having to hold the template during surgery. In this study, a survey showed that the fit of the template decreased because of flap elevation. Setting the incision line towards the palatal/lingual side of the implant platform position reduces the effect of flap elevation.
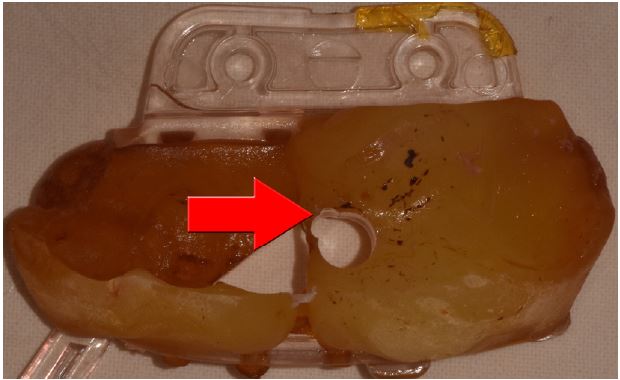
To prevent bone necrosis due to heat during osteotomy and implant placement, water cooling is essential.20 However, as the surgical field is physically blocked by the surgical template, sufficient coolant does not reach during these procedures. Previous studies also reported that the temperature increments of osteotomy under a surgical template were higher than those of a freehand osteotomy, which were 6.8°C, 9.0°C, 8.7°C at the depths of 3 mm, 6 mm, and 9 mm, respectively.11,21 In the present survey, 45.5% of the respondents said that the water through the irrigation hole was “slightly insufficient”. Owing to the non-sleeve characteristics of the VARO Guide®, it is difficult to form multiple irrigation holes without harming the stable fixation of the sleeve, and the insufficient amount of water can be a disadvantage as the position of the spout is determined by the manufacturer (Fig. 5). To overcome this, it is believed that using cold saline at approximately 5°C rather than at room temperature will help maintain temperatures below 47°C, which is a critical temperature for osteonecrosis.22
Post-implantation accuracy was not evaluated with 3D CBCT, but by the surgeon’s subjective feeling comparing panoramic view after the surgery, which is a limitation of this study. To precisely evaluate post-implantation accuracy, apical, coronal, and angulation deviations should be measured using 3D CBCT scans.
The insufficient number of CGS systems used and insufficient control of variables are the limitations of this study. The satisfaction and accuracy of CGS may vary depending on various variables, such as implant position in the dental arch (anterior or posterior), the number of implants using a single template, bone grafting, and flap elevation. However, these variables have not been fully considered. In the future, studies that increase the number of templates used, control variables, comparison with other systems, and 3D accuracy comparison are necessary.
Ⅴ. Conclusion
The following conclusions were drawn by evaluating the convenience and accuracy of the template production process, and the convenience and accuracy of the implant placement process, within the limits of this study targeting surgeons who placed implants on actual patients using the VARO Guide®.
1.Satisfaction with the ease of use of the planning software and implantation process and accuracy after implantation is high.
2.The flapless implant surgery has a relatively better fitness of the template; therefore, the surgeon's satisfaction level is high.
3.Since the irrigation hole has some limitations when using the VARO Guide®, it may be helpful to use a low-temperature coolant to place the implant.
