

Ⅰ. Introduction
The dental implant first introduced by Branemark et al. was placed in the fully healed alveolar ridge of an edentulous patient.1 At that time, the placement of the implant was delayed after 6−8 months from extraction.2 To date, implant treatment has been extended to recover the partial edentulous alveolar ridge by implant prosthetics of single and multiple teeth.3 Dental implants, being a common treatment, have raised the argument that the delayed placement has caused some problems such as more bone resorptions in the extraction socket4 and elongated treatment duration and times, increasing the risks of infection.5To overcome these complications, Schulte et al.6 first introduced the concept of “immediate implant placement” after extractions. For the timing of placement, Hammerle et al.7 suggest four stages of classification following the healing process of the extraction socket. Chen and Buser et al.8 define four types of healing procedures: immediate (type 1), early (type 2, soft tissue healing), delayed (type 3, partial bone healing), and late (type 4), considered common criteria at this time. The survival rate difference of the implant between the immediate placement and the delayed placement after complete healing of the extraction socket was not clinically significant, as it has been accepted as an ordinary treatment.9 However, in the upper posterior area, the residual alveolar ridge may decrease width and height due to periodontitis related alveolar bone resorptions, alveolar bone recession after extractions, and sinus-pneumatization. These problems make surgeons difficult to treat with immediate implant placement.10 In this case, elevation of the maxillary sinus membrane with immediate implant placement would be available in limited indications.
The maxillary sinus elevation technique as a modification of the Caldwell-Luc operations were first reported by Tatum et al.,11 escalating the membrane of the maxillary sinus with bone graft. Summers et al.,12 continuously applied osteotome to the crestal approach. The crestal approach has the advantages of reduced postoperative discomfort due to a smaller surgical area; however, it has some disadvantages, such as more headache or benign paroxysmal positional vertigo due to the impact of the osteotome and the restriction of sinus-elevated height. To overcome these disadvantages, the hydraulic sinus lift technique was devised using water pressure to elevate the sinus membrane.13 Hydraulic sinus lift technique has limited indications as requiring at least 4−8 mm of residual alveolar bone; however, it is advantageous in smaller operating areas and has minimal side effects.14
This case report describes implant placement immediately after extraction of the upper left second molar with elevation of the maxillary sinus membrane with the hydraulic sinus lift technique.
Ⅱ. Case Report
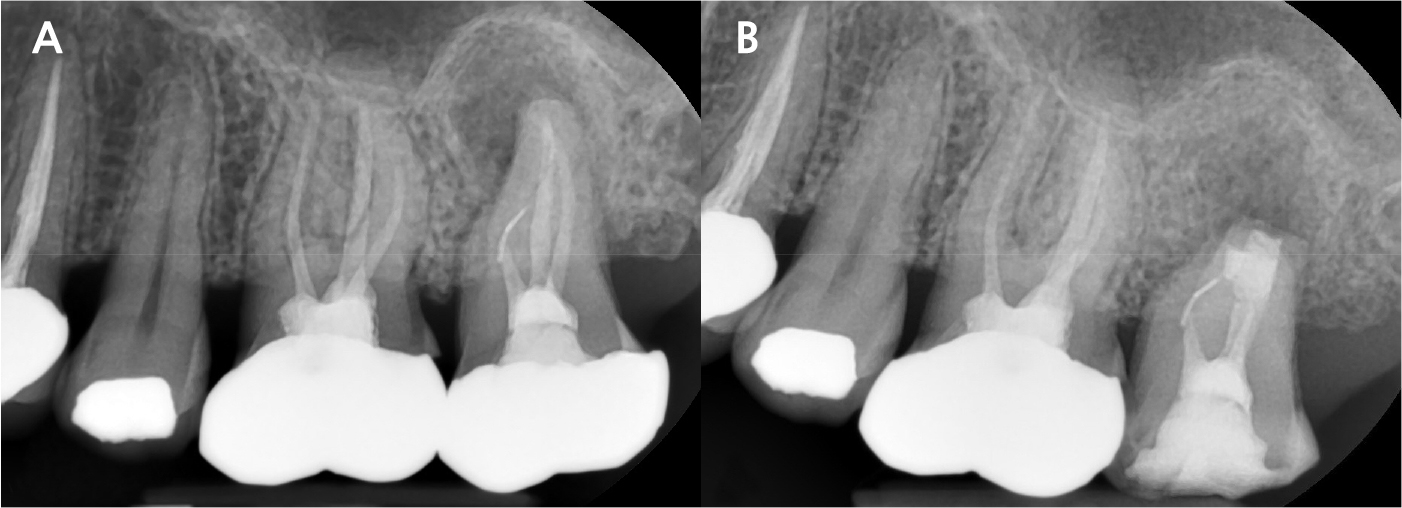
A 43-year-old female needing implant treatment and extraction of the upper left molar visited the clinic. Her upper left second molar showed second degree of tooth mobility and had a treated history of intentional replantation (Table 1). The apical lesion of this tooth disappeared after the intentional replantation (Fig. 1A, 1B). There are no signs of additional infection or periodontitis-related inflammation (Fig. 2). The alveolar bone height of this site was more than 5 mm, which facilitates the treatment plan to conduct the immediate implant placement with elevation of the maxillary sinus membrane using hydraulic pressure.
Table 1.
Patient’s information

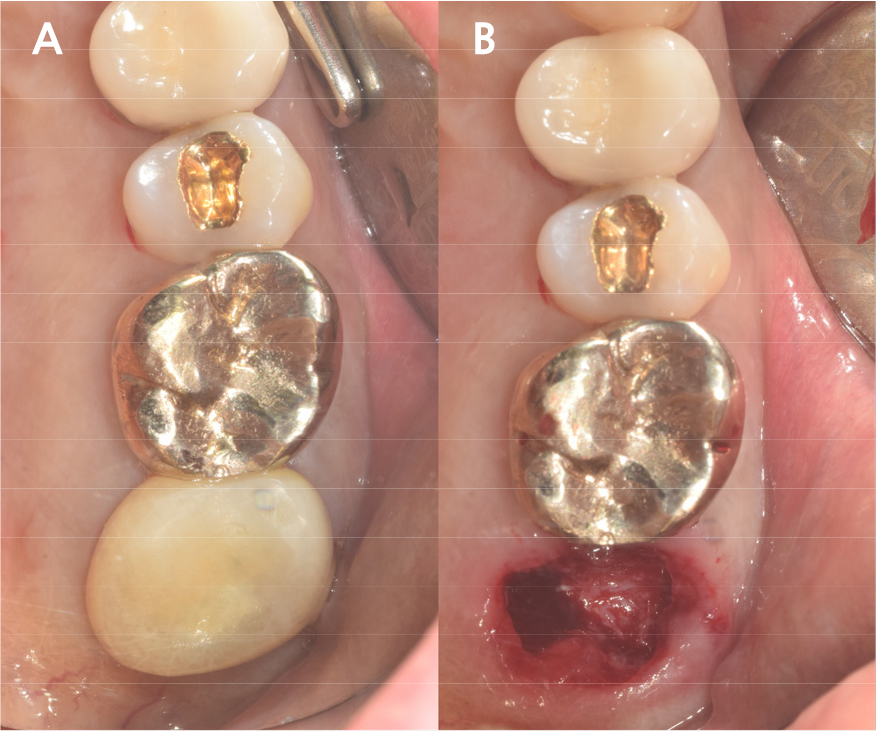
Under local anesthesia with 2% lidocaine (1:100,000 epinephrine; Huons, Seongnam, Korea), the upper left second molar was extracted with minimal damage to the alveolar bone and treated with subgingival curettage to remove apical lesions on periapical radiographs (Fig. 3A, 3B). Consequently, the maxillary sinus membrane was elevated using the hydraulic sinus lift technique through the extraction socket. Before elevation, using the sinus lift kit (CRESTAL APPROACH Sinus KIT; Shinheung, Seoul, Korea), no signs of perforation on the maxillary sinus membrane were verified.
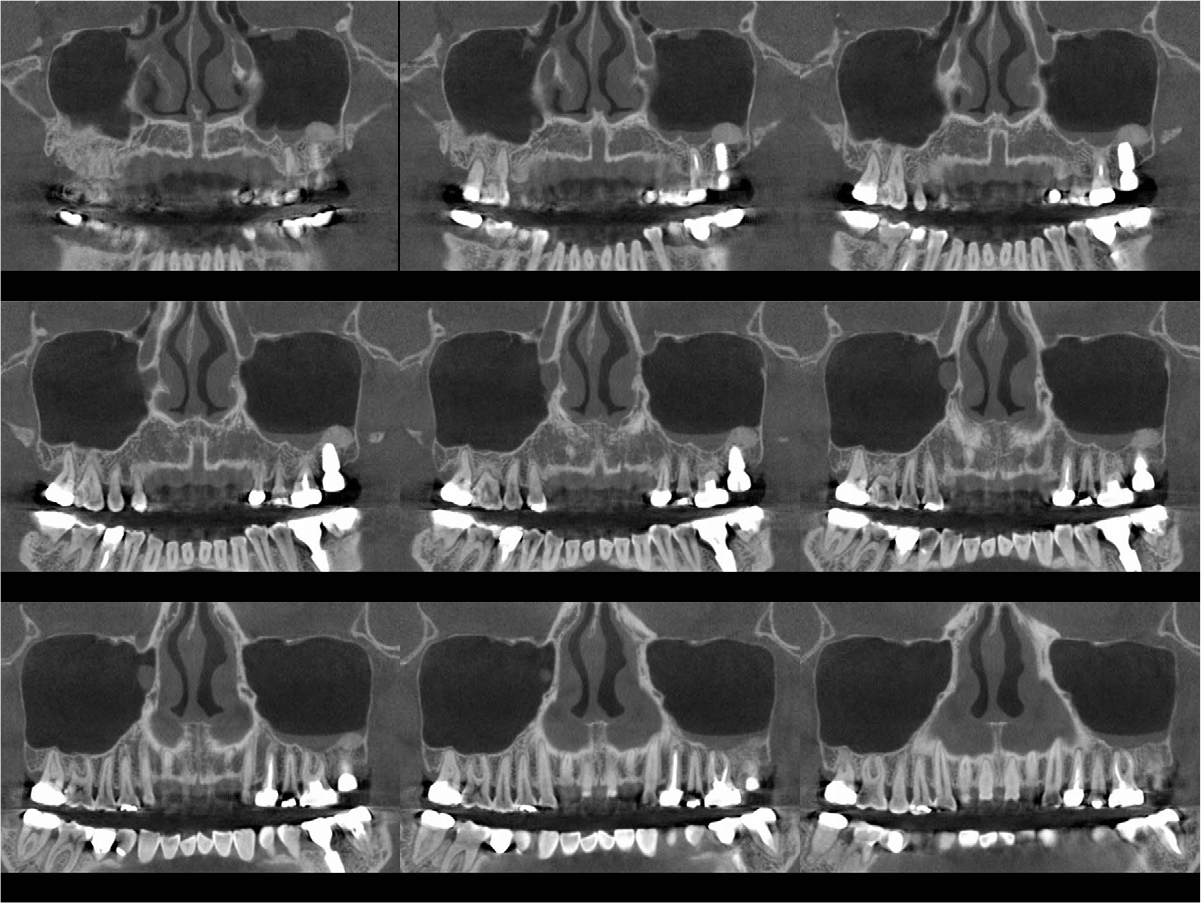
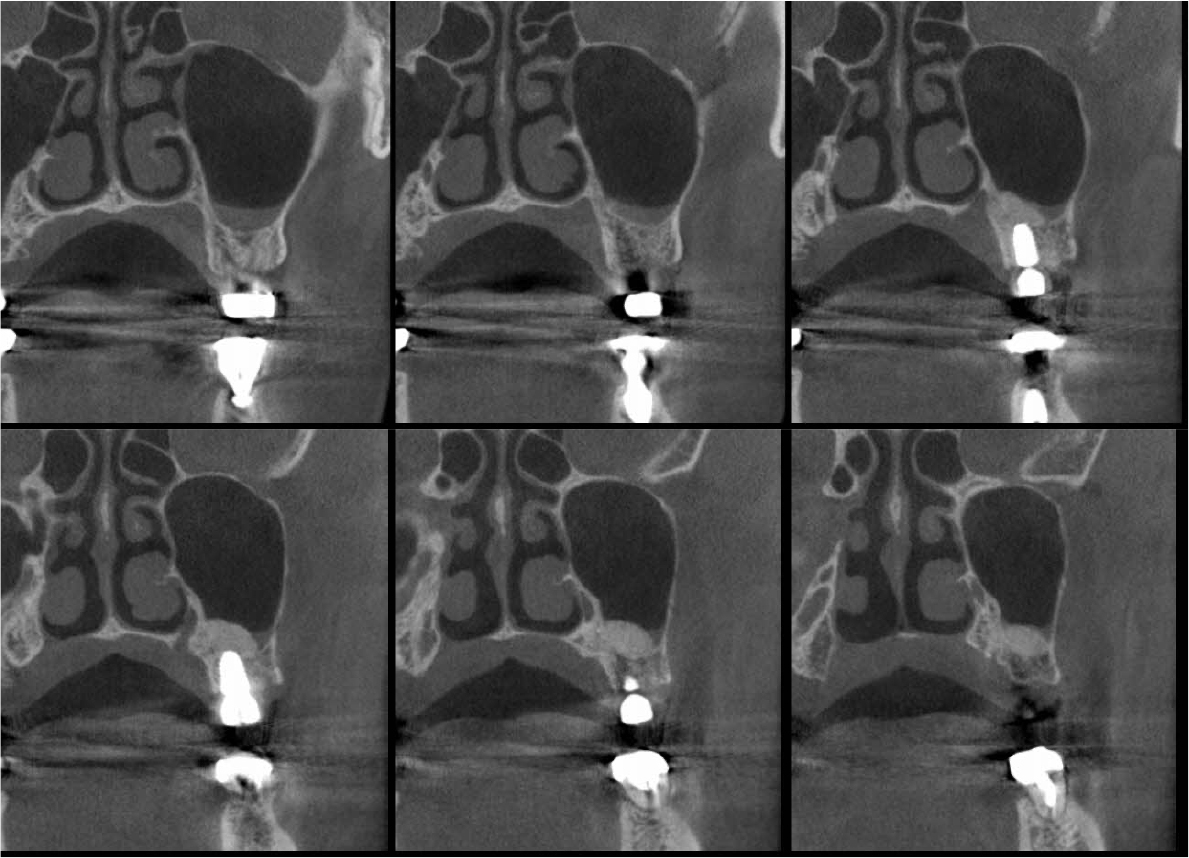
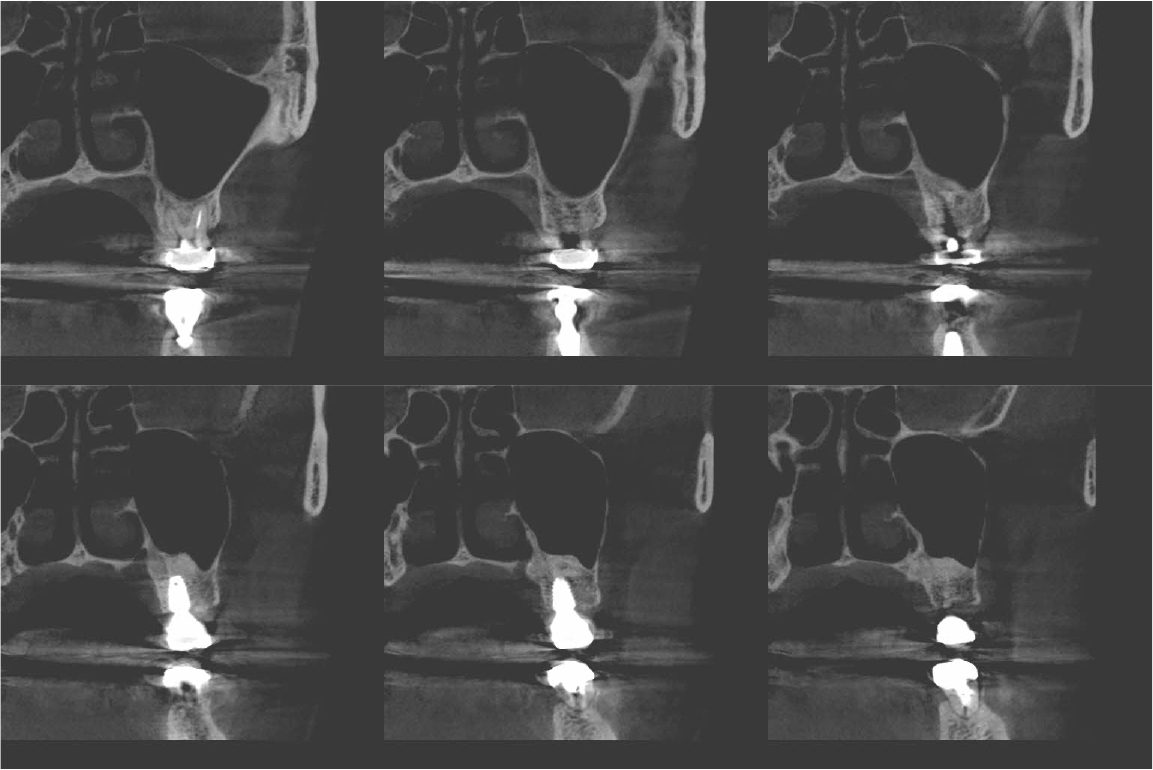
An implant with 5.0 mm diameter and 8.0 mm length (Superline; Dentium, Seoul, Korea) was placed with 0.5 cc of eproteinized bovine bone mineral (DBBM; Bio-Oss®, Geistlich, Wolhusen, Switzerland) by sinus elevation. The implant stability quotient (ISQ) after placement was 64 continually and the healing abutment was placed (6.5 mm diameter, height M size) (Fig. 4A, 4B). Postoperative antibiotics (Sultamox Tab. 500 mg; Alvogen, Seoul, Korea) and analgesics (Somalgen Tab. 370 mg; Alvogen), digestive agent (Beszyme Tab. 470 mg; Dong-A ST, Seoul, Korea) were prescribed for 5 days (30 min after meal). Gargle agent (G.U.M® Dental Rinse S; Sunstar, Osaka, Japan) with no toothbrushing was prescribed to drain and protect the operation area for 2 weeks. Postoperative cone-beam computed tomography (CBCT) showed a dome-shaped elevated membrane with a heterogeneous bone graft surrounding dental implants (Figs. 5 and 6). After 14 days, favorable healing gingiva was confirmed with the stitch-out process (Fig. 7).
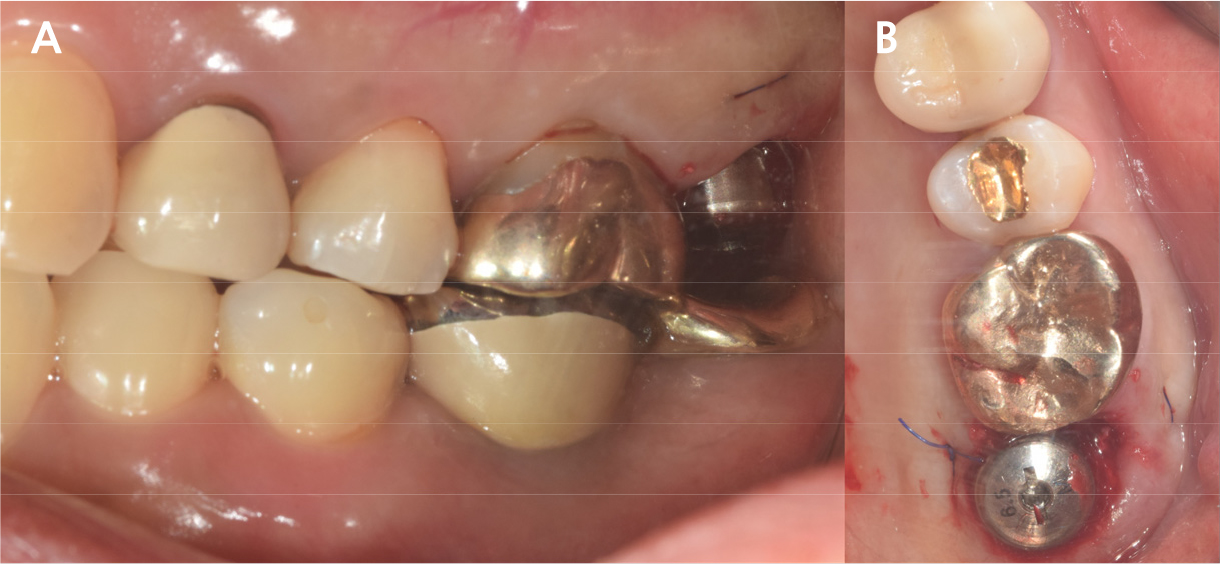

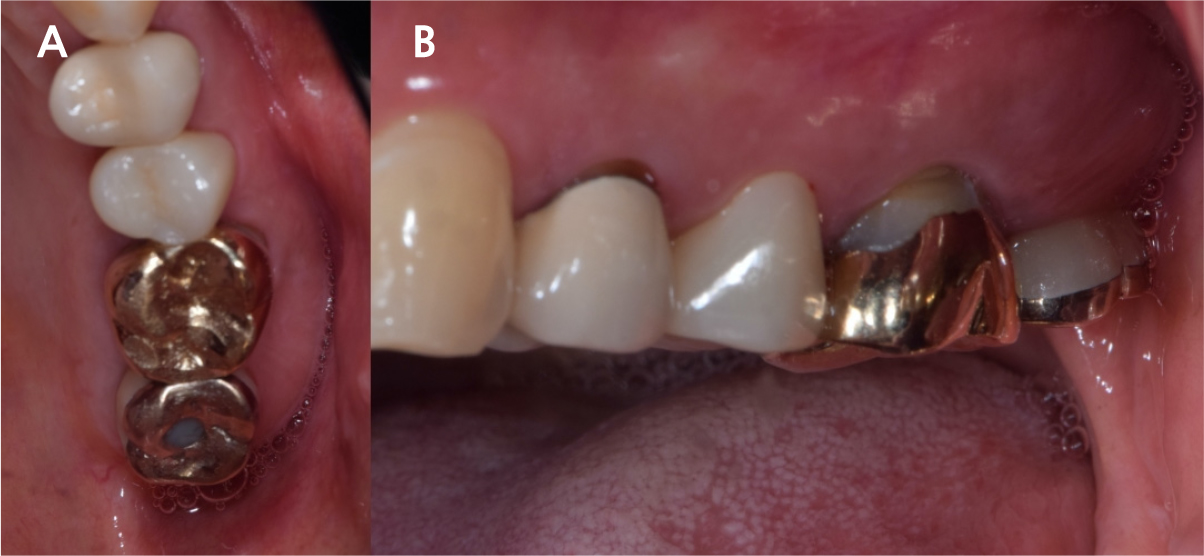
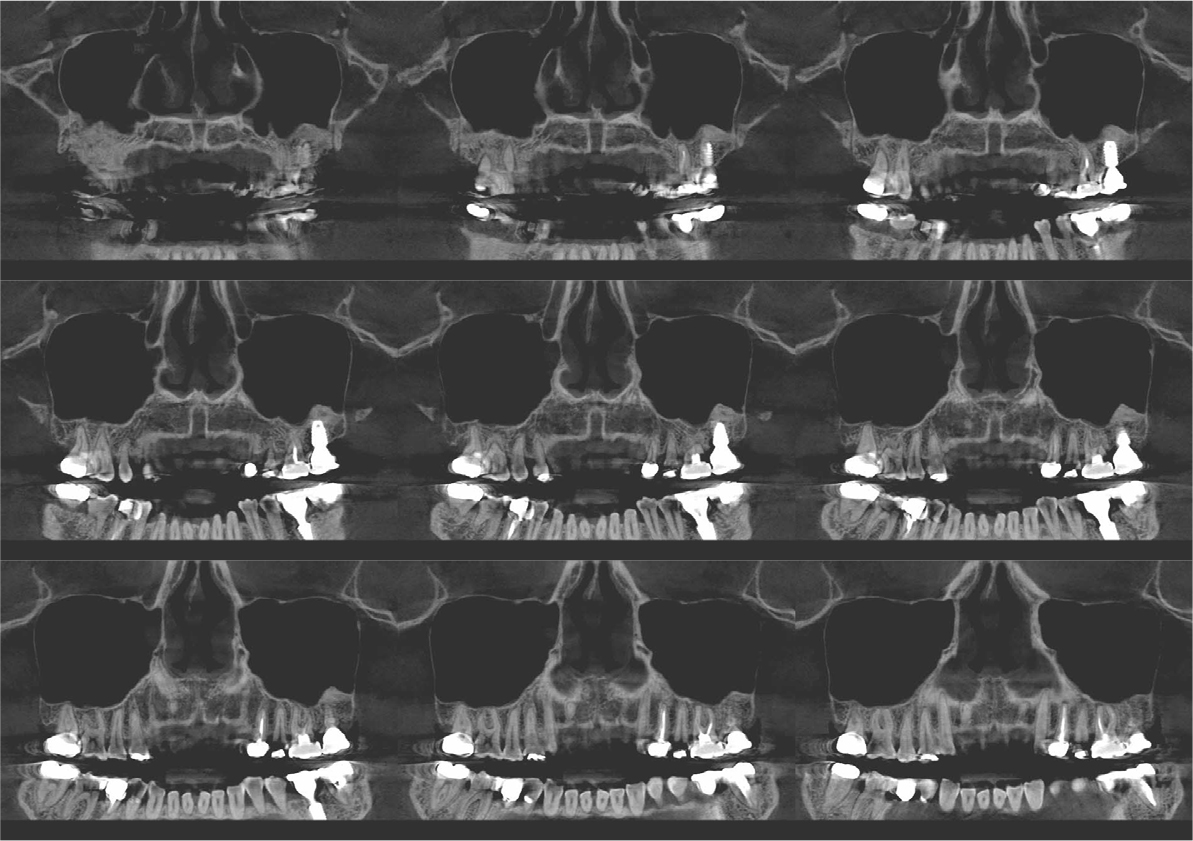
After 4 months of the first surgery, the ISQ value was 71, showing favorable stability, the prosthesis was placed consecutively, and healing progress was observed (Fig. 8A, 8B). After 5 months, the final prosthesis was completed (Fig. 9A, 9B). Supported treatment was initiated and radiographs were taken after 6 months (Figs. 10, 11, 12). In the radiograph analysis, the alveolar bone surrounding the dental implant was stable, with ossified bone verified. In a 6-month interval, the supported treatment was conducted in April 2022, showing no signs of peri-implant gingivitis or bone resorption (Figs. 13 and 14).




Ⅲ. Discussion
Numerous studies have evaluated protocols to increase the success rate of immediate implant placement after extraction. The primary stability of immediate implant placement has been reported to be the most important factor.15 Lioubavina-Hack et al.16 presented at least 3−5 mm residual alveolar bone under the extraction socket as the requirement for successful placement. In this case, a 5 mm residual bone height would be sufficient for primary stability; however, this is not a satisfactory vertical bony height for implant placement. Therefore, the alveolar crestal approach and hydraulic sinus lift technique with DBBM were used for the elevation of the maxillary sinus membrane. As favorable primary stability was guaranteed, the healing abutment was placed consecutively. The sinus membrane was not elevated symmetrically, as ordinary in the case of hydraulic sinus lift, but the fixture was surrounded by sufficient bone graft material verified by CBCT (Fig. 6).
Previous studies have evaluated the positional relationship between the surrounding bone and the fixtures. Vignoletti et al.17 and Caneva et al.18 have reported that buccal bone resorption was significantly lower in the case of implants placed close to the lingual wall. Chen et al.19 also reported that a bone graft between the fixture and the buccal wall, in case of sufficient residual buccal bone thickness, could inhibit horizontal bone resorption; however, vertical bone resorption would be inevitable. In this case, more than 2 mm of residual buccal bone and fixtures placed close to the lingual wall are confirmed by CBCT (Fig. 6). These findings would guarantee favorable surrounding alveolar bone volume after 4 years of implant placement.
In this case, we reduced the treatment time by sinus lift and consecutive immediate installation of implant approximately 3−4 months compared to previously suggested delayed placement.8 Considering the enabling factors for simultaneous procedures, the first was no alveolar septum due to the upper second molars having converging roots, allowing the crestal approach. The second was previous intentional replantations that preserve the apical alveolar bone, providing sufficient bone for favorable primary stability for immediate implant placement. The indications for the above treatment are limited; however, the benefits of reduced treatment time for surgical procedures and reduced duration of total treatment could be suggested to patients to reduce inconvenience.
Ⅳ. Conclusion
Even with a shortage of vertical bone height after extraction of the upper molar, an immediate implant can be placed with the sinus lift crestal approach technique by hydraulic pressure. Using this protocol, the treatment time for surgical procedures and the duration of total treatment are reduced for patients to reduce inconvenience.
