

Ⅰ. Introduction
Ⅱ. Case Reports
1. Case 1
2. Case 2
3. Fatigue strength test
Ⅲ. Discussion
Ⅳ. Conclusion
Ⅰ. Introduction
Clinicians frequently encounter the formidable challenge of prosthetic failure in implants with undocumented treatment histories.1 This challenge is exacerbated by the prevalence of contemporary dental implants that share analogous designs, engineered to optimize primary stability and osseointegration. Such design homogeneity renders accurate differentiation difficult, even for highly experienced clinicians, unless an implant exhibits a distinctive and readily discernible design. When implant identification proves elusive, fixture removal often becomes inevitable, potentially resulting in protracted and financially burdensome retreatment process.
To address this challenge, various dental implant identification frameworks have been developed, primarily relying on radiographic analyses, due to the impracticality of explanting osseointegrated fixatures.2, 3 Recent advances in deep learning have further enabled the development of precise and rapid identification methodologies.4
In South Korea, the Korean Academy of Oral and Maxillofacial Implantology (KAOMI) provides an “Implant Finder” service, allowing clinicians to submit radiographic images of unknown implants via designated social media platforms (e.g., KakaoTalk). Submitted images are cross-referenced with a comprehensive implant database, and identification results are returned through the same channel. Although the service demonstrates reliable and efficient identification, to the best of our knowledge, no reports have yet demonstrated its clinical application or successful outcomes.
This report presents two cases in which undocumented implants were successfully salvaged via multi- implant restorations facilitated by the KAOMI implant finder service, obviating the need for fixture removal. Written informed consent was obtained from both patients for the use of clinical data and images.
Ⅱ. Case Reports
1. Case 1
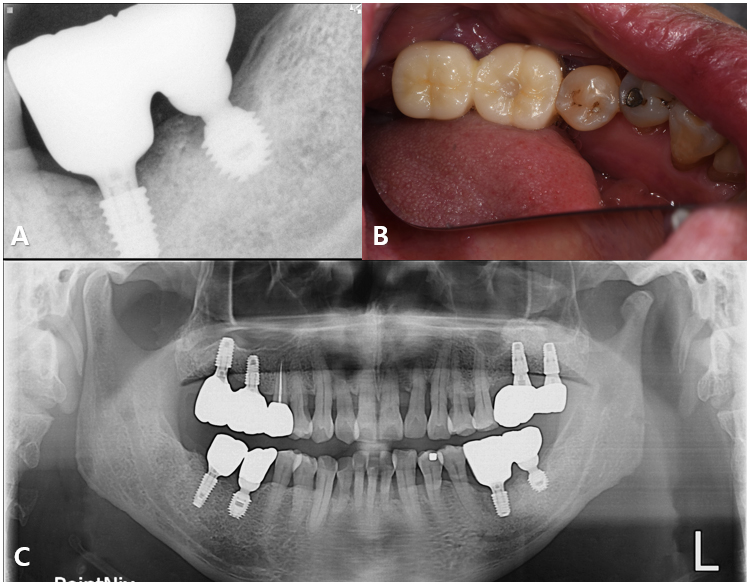
A 57-year-old male presented with suppuration and discomfort in the left mandibular molar region. Clinical and radiographic examinations revealed severe peri-implant inflammation and associated bone resorption around the fixture at site #36, while the implant at site 37 demonstrated stable peri-implant bone support.5 The two implants were restored with a splinted crown prosthesis (Fig. 1).
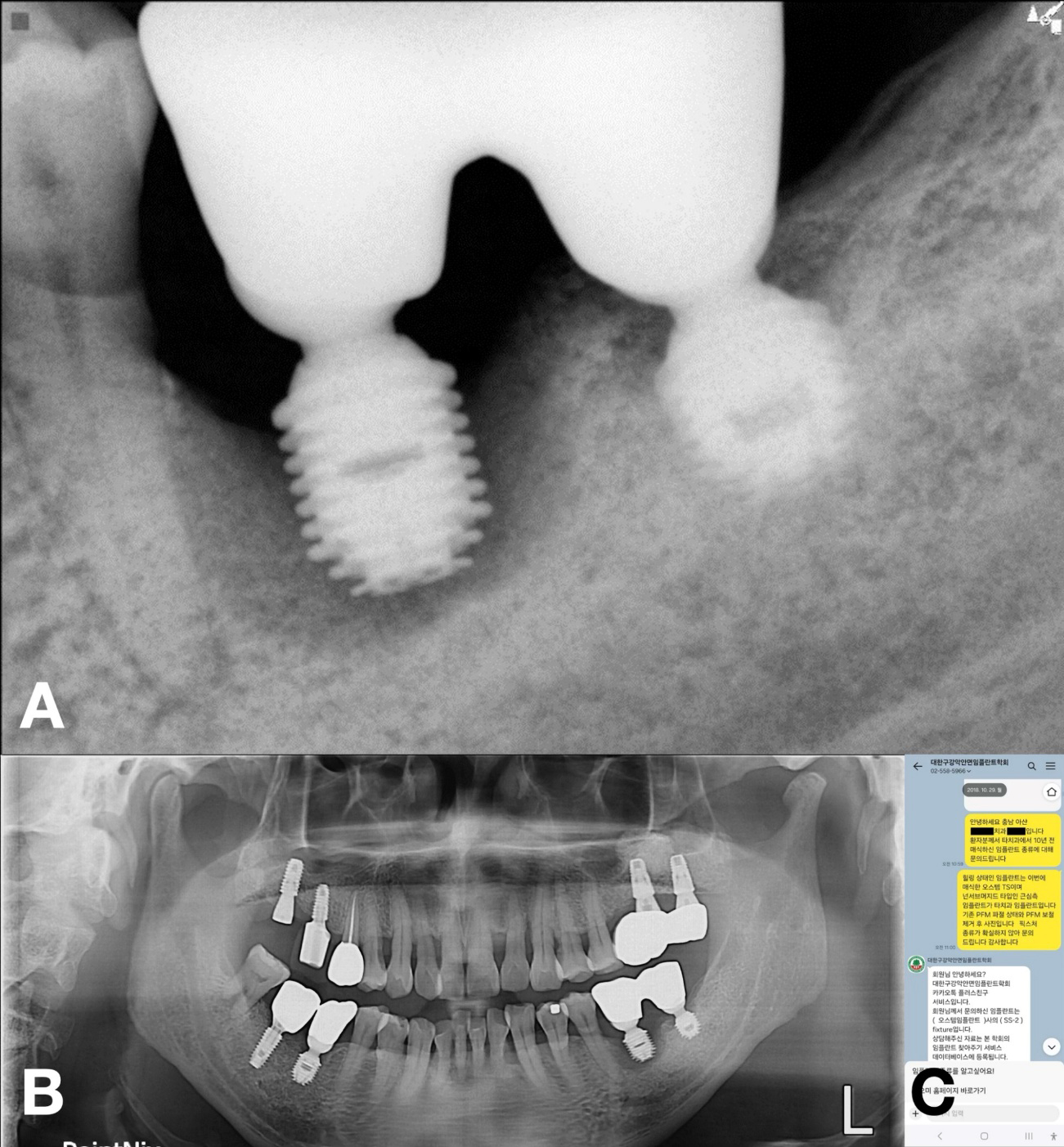
No documentation regarding the implants was available; therefore, the KAOMI implant finder service was consulted. The system identified the type of fixtures as Bicon implants (Bicon LLC; Boston, MA, USA). Based on this information, the manufacturer was contacted, and an appropriate abutment for #37 the fixture, intended for salvage, was procured (Fig. 2).
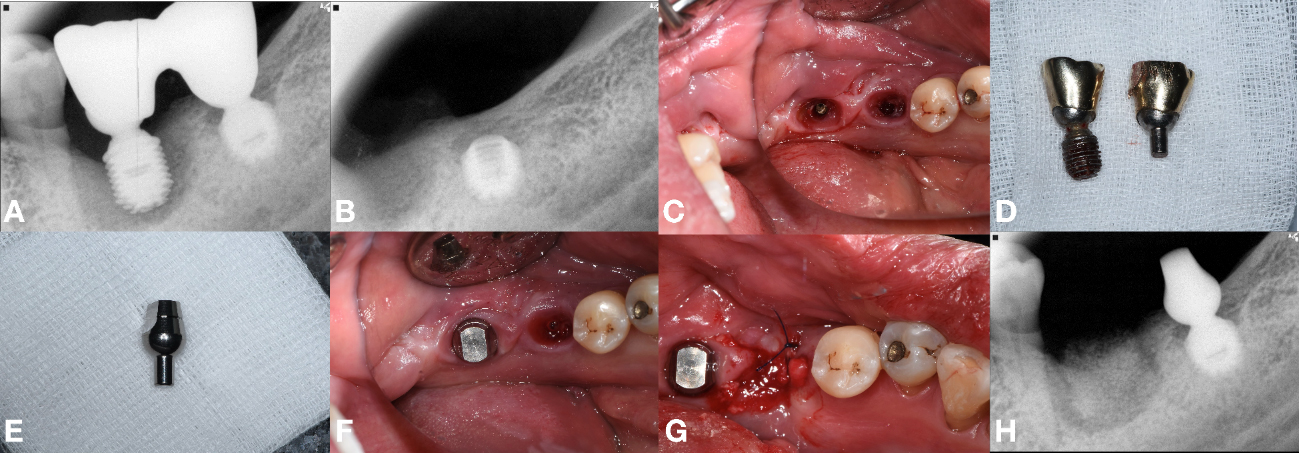
Fig. 2
Radiographic and clinical sequence. (A) Periapical radiograph of #36 and #37 implants, (B) Periapical radiograph after extraction of #36, (C) Bridge sectioning and explantation of #36, while salvaging #37, (D) Removed #36 fixture and #37 abutment crown, (E) Abutment prepared using information from the implant finder service, (F) Procured stock abutment seated on surviving #37, (G) GBR performed at site #36, (H) Periapical radiograph of #36 GBR site.
The procedure progressed uneventfully. The failing implant at site #36 was removed, followed by guided bone regeneration (GBR). The extraction socket was grafted with freeze-dried bone allograft (FDBA) (Sure-OssTM-POWDER; HansBioMed, Seoul, Korea), covered with a self-expanding biodegradable collagen matrix (Regenomer; NIBEC, Chungbuk, Korea), and sutured with 4-0 nylon (Blue nylon; Ailee Co, Busan, Korea).
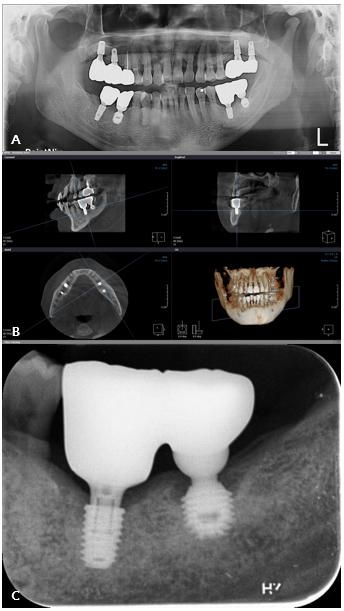
After a healing period of approximately 5 months, a new implant (TSIII, 4.5 mm diameter, 7 mm length; Osstem Implant, Busan, Republic of Korea) was placed at site #36 with an initial torque of 25 Ncm. A healing abutment (95 mm diameter, 7 mm height) was placed simultaneously (Fig. 3).
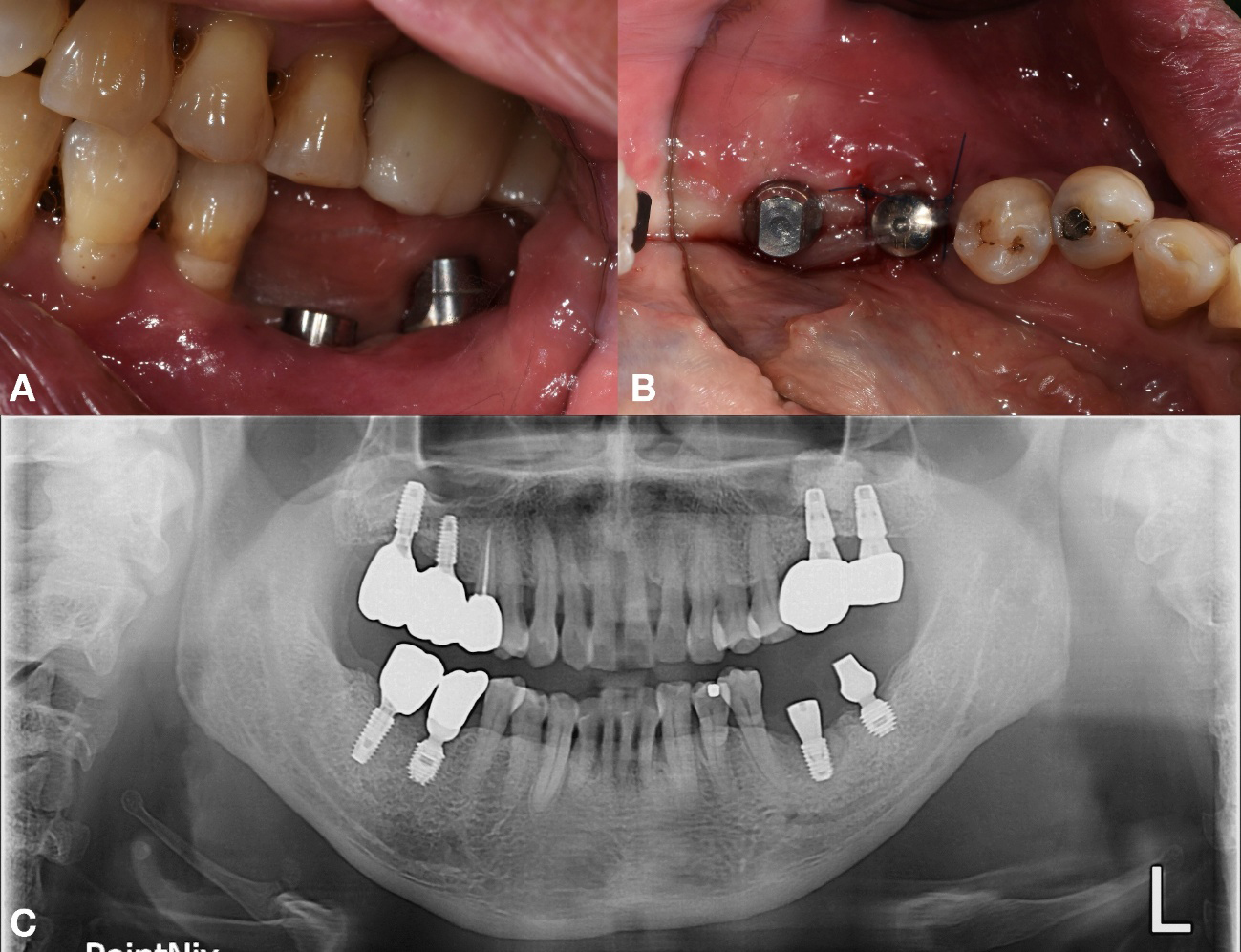
Approximately 3 months after implant placement of #36 implant, prosthetic rehabilitation was initiated. A custom abutment was fabricated for #36, and a new abutment was delivered for the salvaged, preexisting fixture of implant #37 (Figs. 4 and 5).
After 2.5 years, the prosthesis remained functional without significant complications, and radiographs confirmed stable peri-implant bone levels surrounding both fixtures (Fig. 6).
The clinical workflow can be summarized as follows: 1) Submission of radiograph of the target implant (#37) to the KAOMI implant finder service via a messaging application, 2) Retrieval of identification details (manufacturer and product line), 3) Procurement of corresponding prosthetic components, 4) Delivery of the final prosthesis, and 5) Long-term follow-up evaluations.
2. Case 2
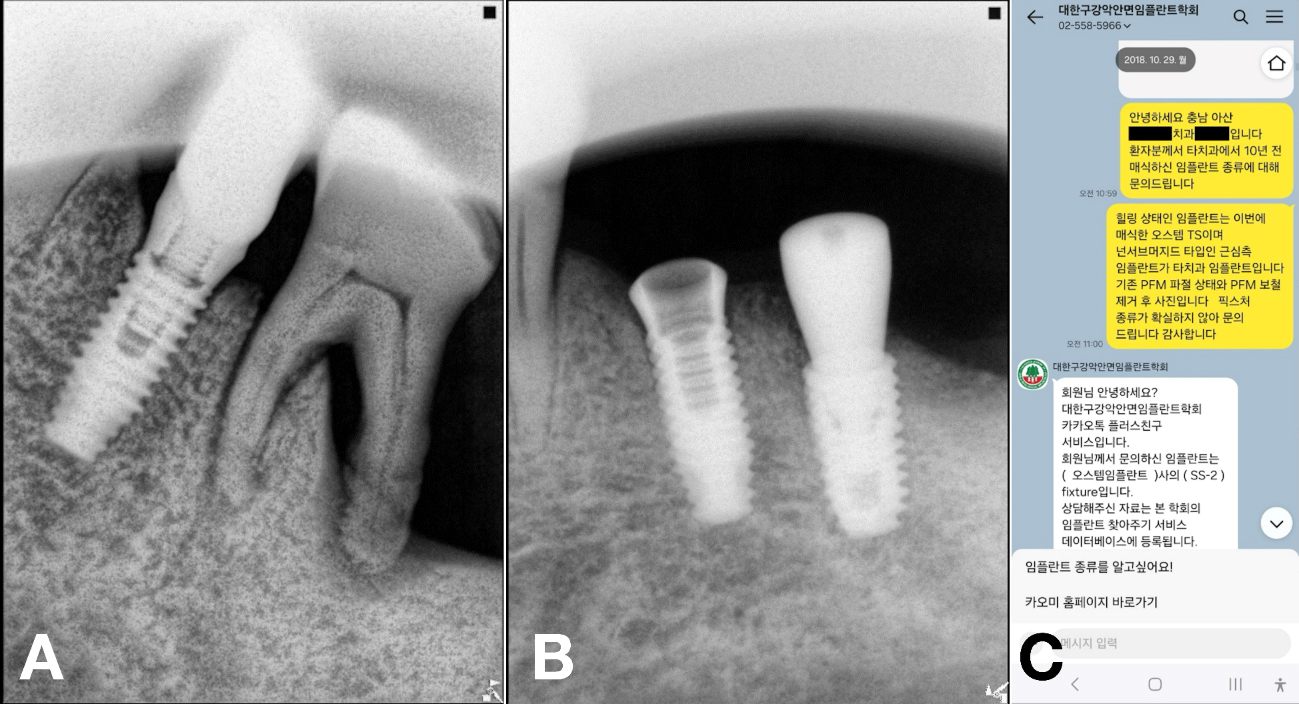
A 69-year-old male presented with discomfort in the left mandibular molar region. Tooth #36 was deemed hopeless and subsequently extracted, whereas the adjacent #35 implant exhibited a fractured crown on an existing undocumented fixture.6, 7 Two months after a GBR with a FDBA at site #36, a new implant (TSIII, 4.5 mm diameter and 8.5 mm length; Osstem Implant) was placed with an initial torque of 35 Ncm. A healing abutment (5 mm diameter, and 7 mm height) was simultaneously placed. As the implant at site #35 remained undocumented, the KAOMI team again was consulted. The fixture was identified as SS-2 (SS-2; Osstem Implant) (Fig. 7).
The clinical pathway involved initial consultation, implant identification, component acquisition, prosthetic delivery, and subsequent follow-up evaluation.
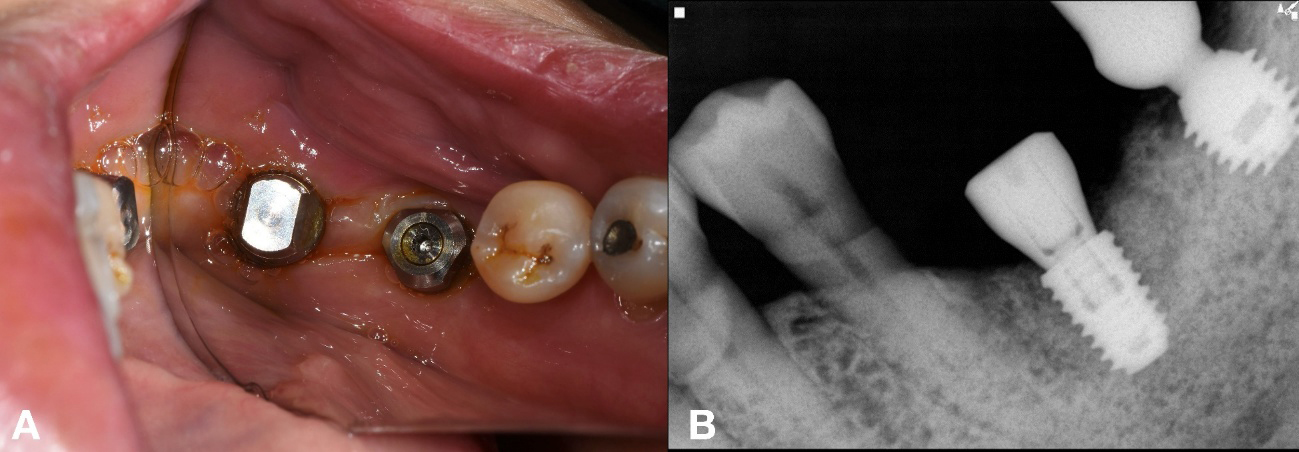
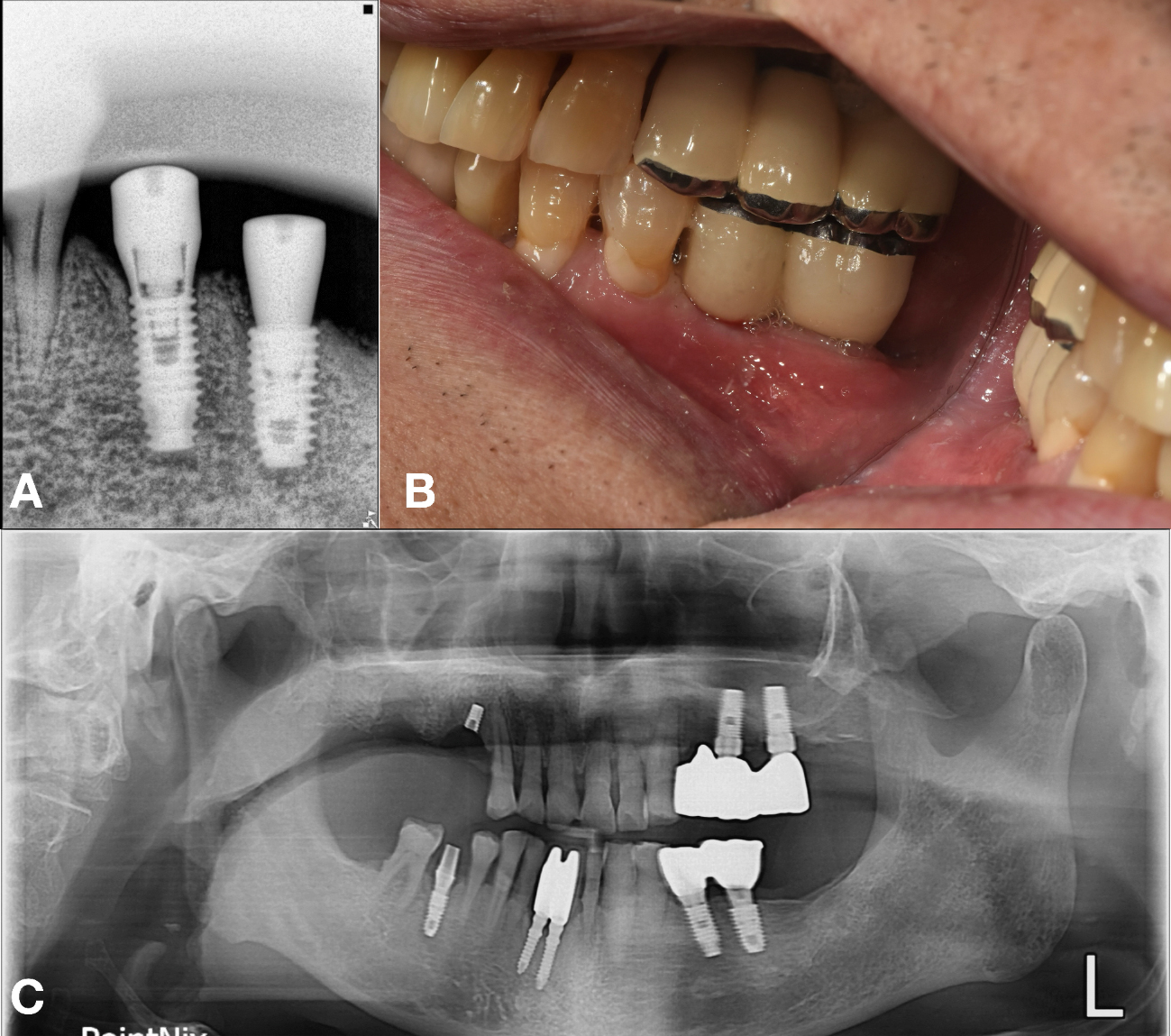
An appropriate stock abutment for fixture (#35) was procured, enabling reuse of the existing implant for patient comfort and reduced surgical morbidity. The restoration was completed based on the information provided by the implant finder service (Fig. 8A and 8B).
At the 6 year follow-up, the implants on the mandibular left side remained functional and stable. However, the patient experienced implant fracture in the maxillary right quadrant, possibly due related parafunctional activity such as bruxism (Fig. 8C).8
The clinical workflow can be summarized as follows: 1) Submission of a radiograph of the target implant (#35) to the KAOMI implant finder service via a messaging application, 2) Retrieval of identification details (manufacturer and product line), 3) Procurement of corresponding prosthetic components, 4) Delivery of the final prosthesis, and 5) Long-term follow-up evaluation.
Ⅲ. Discussion
Clinicians frequently face the challenge of prosthetic failure in implants with undocumented treatment histories. While every effort is made to salvage existing implants, the following two main factors often complicate these cases: a lack of documentation and parafunctional habits (e.g., bruxism) that contribute to unpredictable biomechanical overloading.9 These circumstances necessitate the removal of otherwise osseointegrated fixtures, thereby subjecting patients to additional surgical and financial burdens. Accurate identification of existing fixtures and their corresponding abutment can transform a surgically integrated but prosthetically compromised implant into a functionally successful one, thereby minimizing patient discomfort and the burden of re-treatment.
In situations where fixture removal is unavoidable, particularly when implants are splinted, identification of the remaining fixtures is critical for designing a compatible prosthesis.10, 11 To the best of our knowledge, the KAOMI implant finder service addresses this challenge through expert-driven analysis of submitted. A panel of experienced implant specialists reviews the images, cross-references them with an extensive database, and provides highly accurate fixture identification.
This report illustrates two cases in which an implant finder service enabled the salvage of undocumented implants, obviating unnecessary removal and facilitating long-term prosthetic function. While limited by a small sample size and lack of a comparator group, these cases highlight the clinical value of collaborative services such as KAOMI in bridging diagnostic gaps.
Furthermore, recent advances in artificial intelligence, including machine and deep learning, offer promising new avenues for precise and efficient implant identification.12, 13 Such technologies may pave the way for more accurate and comprehensive implant detection services in the future.14, 15
