

Ⅰ. Introduction
Sinus floor elevation is a well-established surgical intervention for vertical ridge augmentation in the posterior maxilla, primarily aimed at facilitating the placement of implants of appropriate lengths in sites with insufficient bone height. Among the available techniques, the transcrestal approach—introduced initially by Tatum in 1977 and subsequently refined by Summers in 1994 through the use of osteotomes—has gained widespread acceptance due to its minimally invasive nature and reduced patient morbidity compared with the lateral window technique.1 The clinical applicability of the transcrestal sinus floor elevation technique is primarily constrained by anatomical conditions, particularly the presence of a relatively flat sinus floor and minimum residual bone height (RBH) of approximately 5 mm.2,3 When these prerequisites are not met, such as in cases with sloped sinus morphology4 or advanced ridge resorption, the risk of membrane perforation increases, and controlled elevation becomes technically demanding. In principle, this technique is performed without direct visualization and relies heavily on the operator’s tactile perception and experience. Limited visibility through narrow surgical access restricts the detection of membrane perforation, and the uncontrolled application of malleting forces may traumatize the sinus membrane, potentially causing complications such as membrane tears,3 benign paroxysmal positional vertigo, or, in rare cases, implant displacement into the sinus cavity.5
To address these limitations, several modifications to the transcrestal approach have been introduced, including osseodensification drilling,6 rotating instrument–assisted techniques,7 hydraulic elevation,8 graftless protocols,9 and platelet-rich fibrin (PRF)-mediated methods.3 However, their effectiveness continues to rely on the presence of adequate RBH for successful membrane elevation and implant placement.
This report introduces a novel approach to crestal sinus augmentation in sockets with delayed healing, where conventional transcrestal methods are typically contraindicated.
Ⅱ. Case Report
This case series demonstrates the feasibility of transcrestal sinus elevation in sites with severely limited residual bone, presenting three clinical cases involving erratically healed10 maxillary posterior extraction sockets, each exhibiting severely compromised RBH (< 1 mm) while maintaining an intact Schneiderian membrane. In these patients, crestal sinus access was achieved without excessive malleting. Membrane elevation was initiated by tactile probing with an osteotome and hydraulic pressure applied using a standard syringe connected to a silicone hose, and was completed through the passive insertion of bone graft material into the sinus cavity. Simultaneous guided bone regeneration (GBR) was performed within the extraction socket. Postoperative cone-beam computed tomography (CBCT) consistently revealed a distinctive hourglass-shaped bone regeneration pattern, reflecting dual-compartment augmentation in both the sinus and socket.
1. Case 1
A 65-year-old male was referred to our clinic after experiencing two consecutive implant failures at the site of tooth 16 (Fédération Dentaire Internationale notation), which had been previously treated at a local clinic. The patient presented 3 months after removal of the second failed implant, having been informed at a local clinic that further implant placement was not possible due to insufficient bone volume. CBCT revealed near-complete loss of the sinus floor bone with a thick lateral wall (> 3 mm), rendering the lateral window approach less favorable and prompting the selection of transcrestal sinus elevation. Following full-thickness flap elevation, residual granulation tissue was thoroughly debrided. Tactile probing with an osteotome confirmed contact with the Schneiderian membrane and its integrity. Hydraulic sinus membrane elevation was performed using saline irrigation, followed by passive insertion of 0.5 g of deproteinized bovine bone mineral (Bio-Oss; Geistlich Pharma AG, Wolhusen, Switzerland) into the sinus cavity. Simultaneous GBR was performed in the extraction socket using a 250 mg block-type xenograft (Bio-Oss Collagen; Geistlich Pharma AG) and a ribose-crosslinked collagen membrane (Ossix Plus; Datum Dental Biotech, Israel). Primary closure was achieved using periosteal-releasing incisions and resorbable sutures. At 5 months, CBCT demonstrated substantial vertical bone gain of up to 13.1 mm. A dental implant (TS III, Ø5.0 × 8.5 mm; Osstem Implant, Seoul, Korea) was placed with adequate initial stability, and a healing abutment was connected at the time of surgery using a one-stage protocol. Prosthetic loading was initiated at 4 months postoperatively after confirming sufficient osseointegration with an implant stability quotient (ISQ) value of 80. The implant remained functional and complication-free during the 46-month follow-up period. The sequential clinical and radiographic findings of Case 1 are shown in Fig. 1.
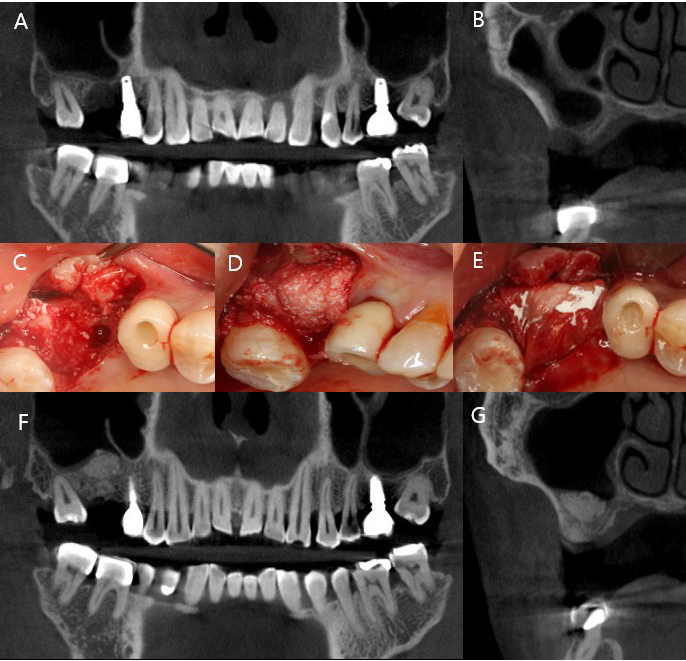
Fig. 1
Representative case of crestal sinus elevation in an erratically healed extraction socket. (A, B) Preoperative cone-beam computed tomography (CBCT) showing severe crestal bone resorption and partial continuity of the extraction socket with the maxillary sinus cavity, (C–E) Intraoperative images after flap elevation and granulation tissue removal. Transcrestal sinus floor elevation with guided bone regeneration (GBR) was performed using deproteinized bovine bone mineral and an absorbable collagen membrane, (F, G) Five-month postoperative CBCT demonstrating hourglass-shaped bone formation with 13.1 mm vertical bone height gain.
2. Case 2
A 65-year-old male presented with an oroantral fistula at the site of a previously grafted tooth 27 extraction socket. The patient reported that bone grafting had been attempted at a local clinic but was complicated by postoperative infection and wound dehiscence. Clinical and radiographic examination confirmed communication with the maxillary sinus and exposure of infected graft material (Fig. 2A to 2D). Initial management involved thorough debridement, removal of the infected material, and reinforcement of the Schneiderian membrane with an absorbable collagen membrane. Primary closure was achieved using periosteal-releasing incisions to allow for soft tissue healing.
Eighteen months later, a re-entry surgery was performed. Flap elevation revealed that the sinus floor was partially closed with stable soft tissue coverage, although bone regeneration within the socket remained minimal. The Schneiderian membrane appeared intact and resilient, permitting transcrestal sinus floor elevation and simultaneous GBR to be performed under favorable conditions (Fig. 2E and 2F). A transcrestal sinus floor elevation was subsequently performed using 0.5 g of deproteinized bovine bone mineral (Bio-Oss; Geistlich Pharma AG) alongside simultaneous bone grafting using a 100 mg block-type xenograft (Bio-Oss Collagen; Geistlich Pharma AG) and an absorbable collagen membrane (Bio-Gide; Geistlich Pharma AG).
At 6 months postoperatively, a dental implant (TS III, Ø5.0 × 8.5 mm; Osstem Implant) was placed with adequate initial stability, and a healing abutment was connected to allow transmucosal healing. CBCT at that time revealed vertical bone regeneration, reaching a height of 9.9 mm, supporting successful implant placement and long-term stability (Fig. 2G to 2K). The prosthesis was delivered 5 months later after confirming an ISQ above 75. The implant has remained functionally stable and complication-free during 63 months of follow-up under regular maintenance.
Despite the unfavorable condition of sinus exposure due to prior infection, Case 2 exhibited partially preserved bony housing, providing a stable environment conducive to healing and favorable GBR outcomes.
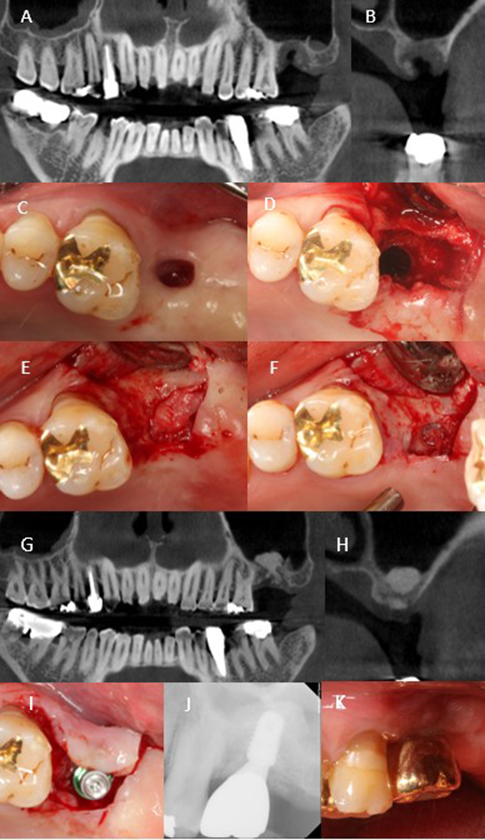
Fig. 2
Clinical and radiographic treatment sequence of Case 2. (A, B) Initial cone-beam computed tomography (CBCT) showing an oroantral fistula and insufficient bone at the previously grafted tooth 27 site, (C, D) Intraoral view before treatment showing sinus exposure, (E, F) Re-entry at 18 months demonstrating partial soft tissue coverage of the sinus floor with an intact Schneiderian membrane, (G, H) Six-month postoperative CBCT showing vertical bone gain in both the sinus and socket compartments, (I) Placement of the implant fixture with sufficient initial stability, (J, K) Periapical radiograph and intraoral image at 63-month follow-up showing stable function and healthy peri-implant soft tissue.
3. Case 3
A 42-year-old male with generalized severe periodontitis underwent the extraction of a floating tooth 26 (Fig. 3A). At 4 months, CBCT revealed incomplete socket healing, with RBH < 1 mm (Fig. 3B and 3C). Transcrestal sinus floor elevation with simultaneous GBR was planned. Following full-thickness flap elevation and meticulous debridement of the compromised socket, the integrity of the Schneiderian membrane was confirmed using an osteotome. Subsequent membrane elevation was achieved using gentle hydraulic pressure with saline irrigation, followed by the insertion of 0.5 g of deproteinized bovine bone mineral (Bio-Oss; Geistlich Pharma AG) into the sinus cavity. GBR was performed in the extraction socket using the remaining Bio-Oss particles and a 250 mg block-type xenograft (Bio-Oss Collagen; Geistlich Pharma AG) and a resorbable collagen membrane (Bio-Gide; Geistlich Pharma AG), achieving tension-free primary closure.
Five months postoperatively, CBCT revealed dual-compartment bone regeneration, with a dome-shaped graft in the sinus and well-contained bone regeneration at the extraction site, yielding a total bone height of 9.5 mm (Fig. 3D and 3E). A dental implant (TS III, Ø4.5 × 8.5 mm; Osstem Implant) was placed with moderate initial stability, and a healing abutment was connected. ISQ measurements of 71/73 prompted an extended healing period, and prosthetic loading was initiated 6 months after placement. At the 38-month follow-up, the implant remained functional, with healthy peri-implant soft tissues and no complications (Fig. 3F).

Fig. 3
Radiographic sequence of Case 3. (A) Pre-extraction radiograph showing severe mobility of tooth 26, (B, C) Four-month post-extraction cone-beam computed tomography (CBCT) images reveal delayed socket healing, (D, E) Five-month postoperative CBCT demonstrating dome-shaped sinus graft and regenerated alveolar bone within the extraction socket, (F) Radiograph at 38-month follow-up showing a stable implant with healthy peri-implant tissues.
Ⅲ. Discussion
Lateral sinus floor elevation is commonly used for RBH < 4 mm but requires extensive flap elevation and vertical incisions, resulting in increased surgical morbidity and patient discomfort. In contrast, the transcrestal approach preserves the buccal wall and shortens recovery time. However, conventional transcrestal procedures involve blind fracture of the sinus floor using osteotomes, which increases the risk of membrane perforation, particularly in cases of irregular sinus anatomy or overdrilling.
This case series presents a minimally traumatic variation of the transcrestal technique performed on compromised extraction sockets with partial sinus continuity. Sinus membrane elevation was achieved using gentle hydraulic pressure and particulate graft insertion, without the use of a mallet or lateral access. Simultaneous GBR was performed within the extraction socket, resulting in dual-compartment vertical bone augmentation.
From a biological perspective, this healing pattern parallels classic socket healing, in which blood clot formation acts as a scaffold for angiogenesis and the recruitment of osteoprogenitor cells from marrow-rich borders.11 Additionally, the Schneiderian membrane contains mesenchymal stem cells capable of osteogenic differentiation,12 which may contribute to bone regeneration when clot stability is maintained. Thus, stable graft containment within the socket-sinus complex may be critical for the observed regenerative outcomes.
Ⅳ. Conclusion
This case series demonstrates a minimally invasive strategy for achieving substantial vertical bone regeneration in the posterior maxilla without lateral window access or extensive malleting. By preserving the Schneiderian membrane and utilizing the anatomical continuity between the sinus floor and extraction socket, simultaneous bone regeneration in both compartments was accomplished with minimal patient discomfort. These findings support the clinical utility of transcrestal sinus elevation under favorable healing conditions, even in cases with severely limited RBH.
