

Ⅰ. Introduction
Swallowing or aspiration of a foreign body during dental treatment procedures can cause critical complications. The average swallowing accident occurrence rate per dentist has been reported to be 0.021/year.1 In previous studies, endodontic instruments, implant devices, teeth, and prostheses were the most frequently swallowed foreign bodies in dental clinics.2 Sometimes, tracheoesophageal fistula, esophageal perforation, gastrointestinal perforation, and esophageal stricture arise because of delayed radiologic diagnosis after swallowing accidents.3 To minimize complications, proper management should be performed.
When a foreign body is swallowed, its location of the foreign body depends on its passage through either the respiratory or gastrointestinal tract. When a foreign body passes through the respiratory tract, it is most often observed in the right main bronchus. The right main bronchus has a larger diameter than the left.2 In a previous study, 50% of patients who aspirated foreign bodies showed no symptoms, and > 90% of patients who ingested foreign bodies showed no symptoms.4 However, foreign bodies may cause diverse critical pulmonary disorders in cases of aspiration through the airway.5 Ingested foreign bodies are mostly excreted spontaneously, while intestinal perforations rarely occur, resulting in sepsis in a few cases.6 From this point of view, the consequences of swallowing accidents might differ depending on their position, shape, and constituents. A radiographic examination can confirm the location of the foreign body, which appears as radiopaque material. Depending on radiographic evaluation results, conservative management or removal can be chosen. Moreover, it is important to transfer patients to specialists to evaluate the need for endoscopic removal when maneuvers to remove foreign bodies fail. In the case of foreign body ingestion, multiple follow-up radiological examinations could be important to trace the location of the foreign body. Conservative treatment can be applied if the foreign body does not cause gastric perforation, although some objects need to be removed endoscopically in some cases.
This clinical case report presents a case of foreign body ingestion during an implant placement procedure and continuous follow-up. The foreign body was excreted from the gastrointestinal tract 2 weeks later, without intervention.
Ⅱ. Case Report
This case report was approved by the Institutional Review Board of Seoul National University (ERI22020) and written according to the guidelines of the CARE checklist. The patient provided informed consent for the publication of the case report.
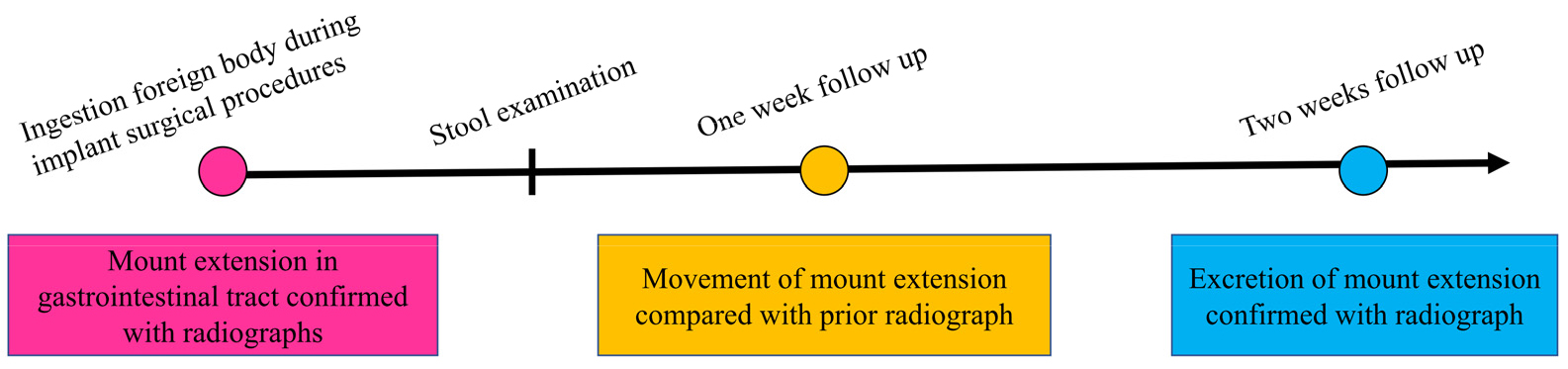
1. Timeline
The timeline of this case report is presented in Fig. 1.
2. Case
A 64-year-old man was referred for rehabilitation with dental implants in the partially edentulous lower jaw. The patient had no relevant medical history. On oral examination, the patient demonstrated severe alveolar bone resorption and tooth loss, particularly in the lower posterior area (Fig. 2). Among the rehabilitation options, the patient decided to extract a hopeless tooth and implant placement.

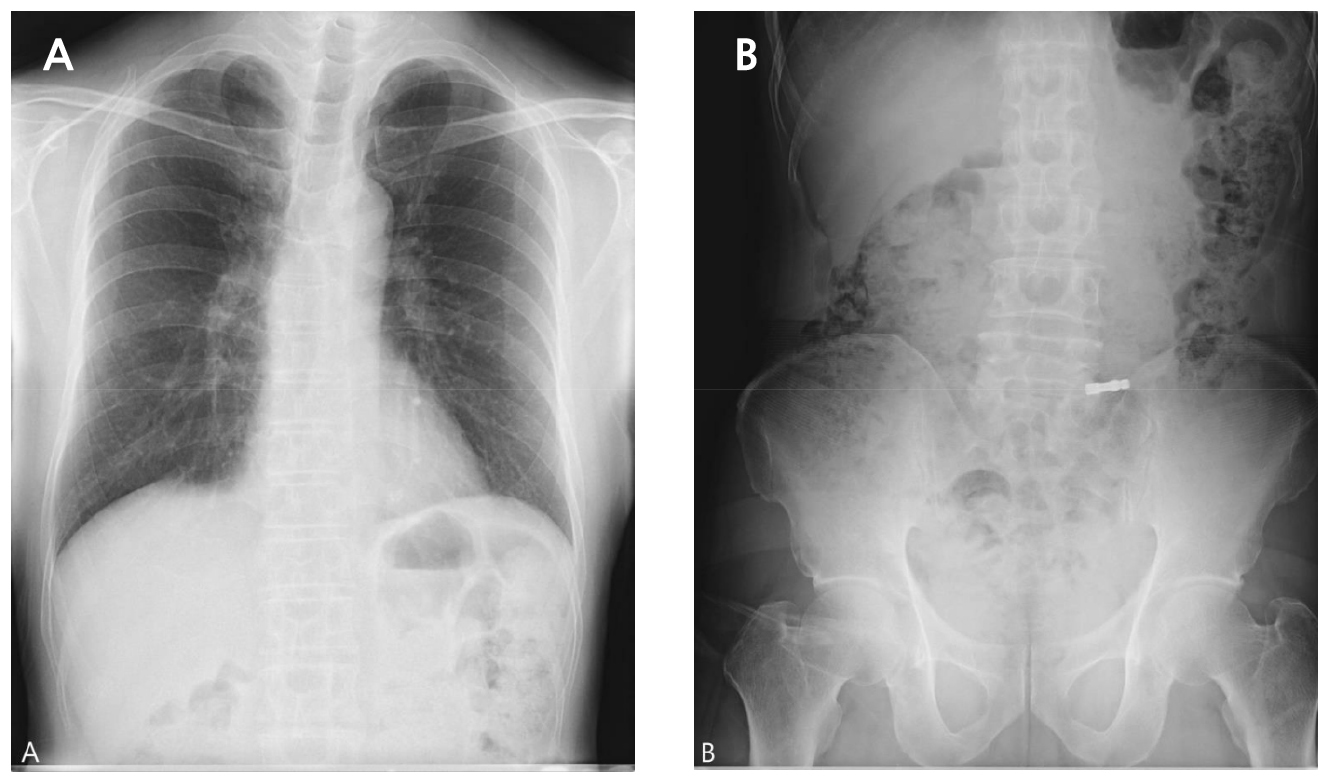
On the day of the surgery, the patient underwent implant placement in the left lower posterior area under local anesthesia. Following the implant placement, location and depth control were conducted with mount extension (ϕ4.8 × 20.5 mm) and a torque wrench. Prevention of swallowing of foreign bodies, including gauze screening, was not performed. During adjustment of the implant location and depth, the patient accidentally swallowed a mount extension into the oropharynx. Despite an immediate attempt to spit out the mount extension, the patient still swallowed it. The patient’s vital signs were stable, and there were no symptoms of discomfort. However, foreign bodies in the airways can cause severe complications. If a mount extension was in his airway, it was removed immediately. The surgical procedure was immediately stopped. Chest posteroanterior (PA) and anteroposterior (AP) radiographs (erect view) were acquired. On two radiographs taken on the day of the swallowing accident, a foreign body was observed in the gastrointestinal tract (Fig. 3). Based on the two radiographs, the foreign body was confirmed to be in the gastrointestinal tract. Because the patient showed no symptoms and the foreign body was expected to be excreted naturally with a low possibility of gastrointestinal perforation, periodic follow-up was performed to confirm that the foreign body was excreted.
Mount extension was observed in a different position in the gastrointestinal tract one week later (Fig. 4). No abnormal signs or symptoms were observed. In general, ingested food is excreted in feces within 24 hours through the gastrointestinal tract. In short, one week may be sufficient for excretion through the gastrointestinal tract. However, the patient answered that he went to the toilet twice a week. Because foreign bodies can cause complications if they remain in the gastrointestinal tract for a long time, the attending surgeon explained the patient’s need to transfer to the Department of Internal Medicine for removal evaluation. However, the patient did not visit an internal medicine doctor for personal reasons. Two weeks after swallowing, the patient came to the clinic, and the mount extension was demonstrated to have been excreted completely on an abdominal AP radiograph (erect view; Fig. 5). No abnormal clinical signs or symptoms were observed.


Ⅲ. Discussion
Ingestion or aspiration of foreign bodies during dental procedures can occur in dental clinics. The supine position makes it easier to aspirate foreign bodies.7 However, the aspiration of foreign bodies is unlikely to occur in healthy adults. Various foreign bodies were swallowed or aspirated. Endodontic files, screwdrivers, crowns, burs (drills), and rubber dam clamps are the most swallowed foreign bodies.4 According to a four-year retrospective study, ingestion occurred more frequently than aspiration.8 Ingestion of foreign bodies during dental procedures mostly occurs during prosthodontic treatment. Elderly patients are prone to ingesting foreign bodies.9
When foreign bodies are aspirated into the bronchus, wheezing, coughing, and breathing hardness are representative features. Occasionally, there are no clinical features, resulting in undetected objects in the long term. This can cause severe complications such as bronchoesophageal fistulas, pneumonia, or abscesses that require a surgical procedure.10 Once a patient swallows a foreign body, diagnosis is important. Radiography is recommended for the diagnosis. Computerized tomography, gastrointestinal endoscopy, and bronchoscopy can also be used as diagnostic tools.11 Although most dental instruments are radiopaque, some are not radiopaque. If radiolucent materials are aspirated, indirect findings such as lobar collapse or other chronic pulmonary changes could be indicated on radiologic examination.12 Therefore, immediate transfer to a specialist is recommended when aspiration is observed or suspected because most aspiration cases require endoscopy or surgery to remove the foreign body.
Ingestion can be considered safer than aspiration because foreign bodies can pass through the gastrointestinal tract without specific signs or symptoms. However, the type, size, shape, and location of foreign bodies in the gastrointestinal tract should be evaluated. In some cases, delayed diagnosis and transfer cause severe complications and necessitate surgical intervention. For example, when foreign bodies are stuck in the esophagus, their type, size, and duration of impaction have been demonstrated to be significant risk factors. Magnetic foreign bodies can cause perforation or necrosis of the gastrointestinal tract, resulting in severe complications.13 When magnetic foreign body ingestion occurs, prompt transfer to a specialist for endoscopic removal is recommended. When a battery component is ingested, the patient must be transferred soon. Second, the size and shape of the ingested foreign body are important factors for determining whether it is an emergency. In a previous study, if a patient ingested a foreign body of size < 2 cm or length < 6 cm, it could be excreted through the gastrointestinal tract. However, foreign body excretion can be influenced by either the size or the patient’s condition, such as sex and age. If the patient shows airway compromise, sepsis, perforation, or active bleeding, transfer to a specialist for emergency treatment is recommended. When a sharp foreign body is ingested, it can perforate the gastrointestinal tract over time.
Furthermore, if the foreign body does not change its position on the radiograph, it can be lodged into deep tissue, resulting in perforation of the gastrointestinal tract.6 The perforation rate of the gastrointestinal tract with sharp foreign bodies is 35%.14 Perforation of the gastrointestinal tract is usually reported in the esophagus, duodenum, duodenojejunal flexure, and ileocecal region.15 Perforation below the esophagus causes acute/subacute peritonitis, leading to clinical symptoms, such as abdominal pain. A positive stool occult blood test result indicates intestinal perforation or obstruction.11 Otherwise, esophageal perforation results in acute mediastinitis with chest pain and severe odynophagia with signs of pneumonitis. Therefore, patients who ingest either long or sharp foreign bodies that do not pass might be transferred to specialists for removal evaluation. Radiological follow-up is necessary to trace the foreign body in cases of ingestion. In general, ingested food is excreted in feces within 24 hours. In a previous study, endodontic instruments passed through the gastrointestinal tract asymptomatically after 2−4 weeks.16 In the present case, the mount extension persisted for approximately 14 days without any pain or symptoms. These results may be due to the patient’s bowel movement habits. According to a previous study, in cases of conservative treatment, weekly follow-up radiographs are recommended to confirm and document the passage of the foreign body.17 In addition, before endoscopic retrieval, it might be helpful to apply laxative and supportive care, as described in a case report.18 However, this may not always be effective or recommended.19
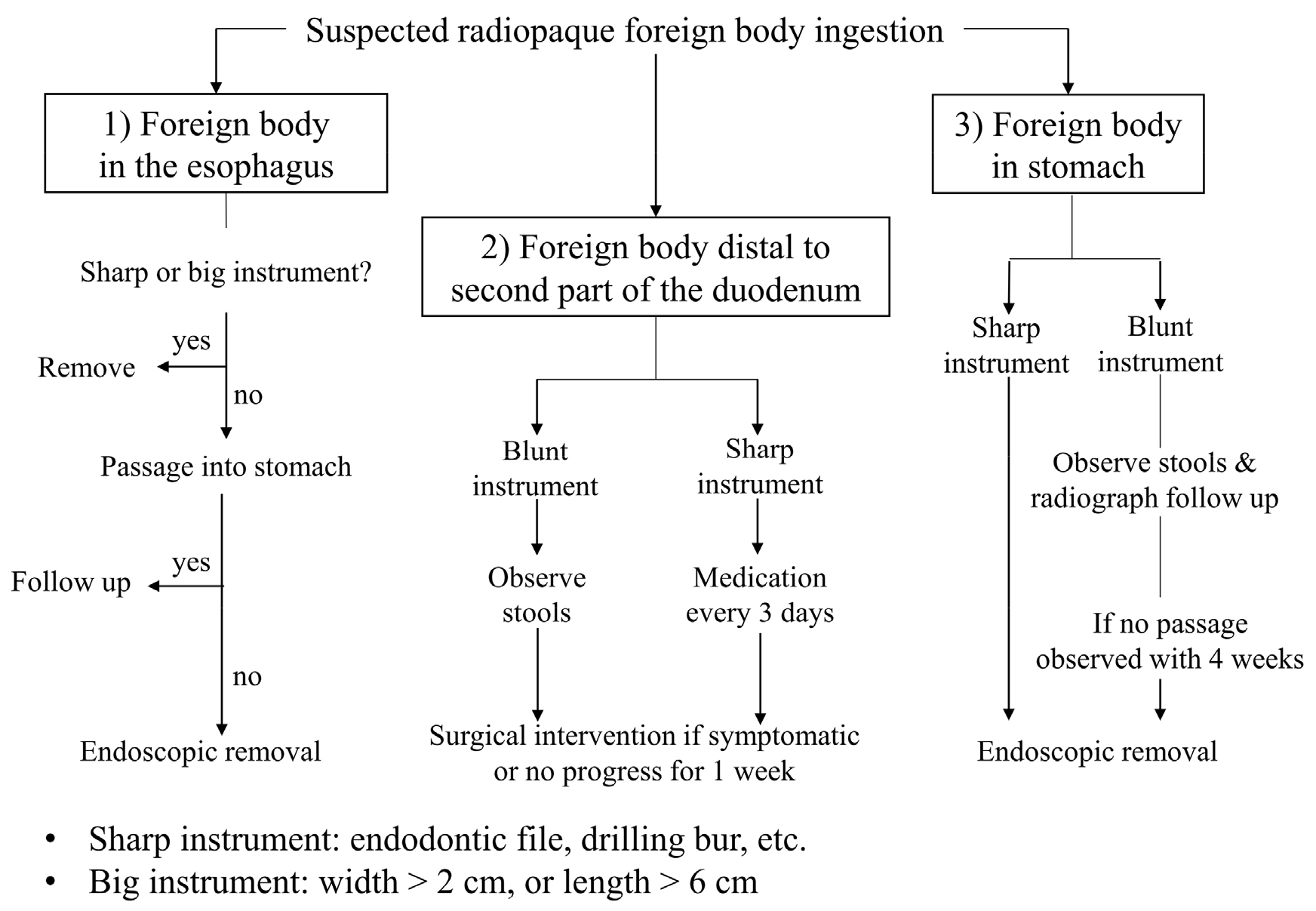
A modified protocol (Fig. 6) is represented when foreign body ingestion accidents occur in dental clinics, depending on the foreign body’s type, size, shape, and location in the gastrointestinal tract, with reference to the previous study.20
Ⅳ. Conclusion
In conclusion, it is important to prevent swallowing accidents using gauze screening and rubber dam application. However, when a swallowing accident occurs during a dental procedure, it is recommended to stop the remaining surgical procedure and expel it the object. Despite these efforts, either ingestion or aspiration can become irreversible. It is important to determine the location of the foreign body using chest PA and abdominal AP radiographs (erect view) to select the proper treatment plan. In the case of ingestion, a non-sharp foreign body of width < 2 cm or length < 6 cm can be excreted within two weeks without any intervention. However, transferring patients to internal medicine specialists is important to evaluate whether the foreign body should be removed early.
