

Ⅰ. Introduction
As implant placement became known as the gold standard for replacing missing teeth, it became popular. However, the success of implant therapy should not depend solely on long-term survival but also on functional, esthetic, hard- and soft- tissue stabilities, and patient-reported outcomes.1
Patients perceive the apical shift of the peri-implant facial soft tissue margin, including mid-facial recession, mucosal recession or dehiscence, soft-tissue dehiscence/deficiency, or a soft-tissue defect as unesthetic. These complications may result in a mucosal recession, gray fixture showing through the mucosa or discrepancy in the length of the implant-supported crown.2
Peri-implant soft tissue dehiscence/deficiency (PSTD) in the maxillary anterior region is common. Approximately 57% of facial PSTD ≥ 1 mm occur within the first 6 months of prosthesis delivery. The etiology of PSTD includes anatomic and pathologic factors. Anatomic factors include a buccally positioned implant platform, osseous dehiscence or fenestration, a thin gingival biotype, inadequate keratinized attached mucosa, and a high frenum. Pathological factors include recurring inflammation, over-contoured prostheses, and brushing trauma.3
The primary aim of treating PSTD should include complete coverage of dehiscence along with re-establishment of the soft tissue margin. Surgical or prosthetic approaches can be used for PSTD coverage. The approach is determined by the position of the implant and amount of soft tissue deficiency.3
Here, we report two cases of PSTD efficiently managed using different surgical procedures in the esthetic area.
Ⅱ. Case Report
1. Case #1
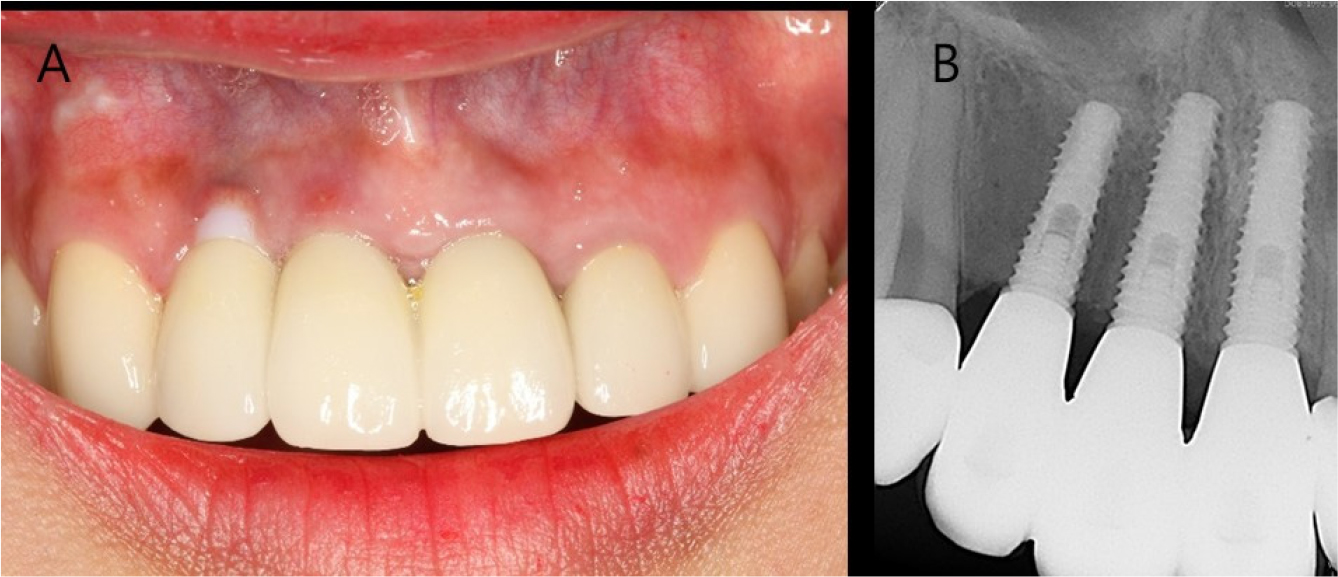
A 26-year-old woman complained of gingival recession around a maxillary anterior implant restoration. The patient had a splinted restoration with 3 implants in the maxillary anterior region placed immediately after tooth extraction (#12, #11, and #21) because of root fracture 2 years before. Bone or soft tissue grafting was not performed according to the patient interview. Clinical examination revealed gingival recession around the implant restoration in the right maxillary lateral incisor region, exposed zirconia abutment, and a gray fixture below the gingiva. A deep periodontal pocket and thin periodontal biotype were observed on the buccal side (Fig. 1).
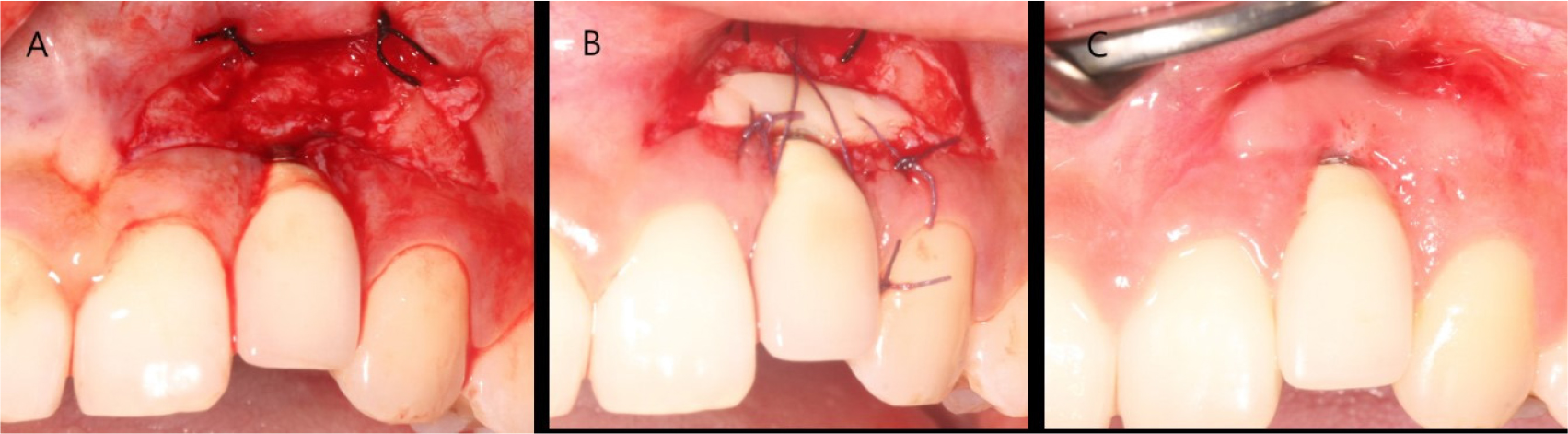
The patient was diagnosed with facial peri-implant soft tissue deficiency of the right maxillary lateral incisor. Soft tissue grafting was planned for gingival coverage of the exposed abutment. An intra-sulcular incision was made, and the flap was reflected. A bone dehiscence defect due to buccal bone resorption was observed. The exposed fixture was decontaminated using chlorhexidine ball scrubbing, titanium curettage and scaling, and saline irrigation. Subepithelial connective tissue was obtained from the palate using the trap door technique. Subepithelial connective tissue grafting was performed with a coronally advanced flap (Fig. 2).

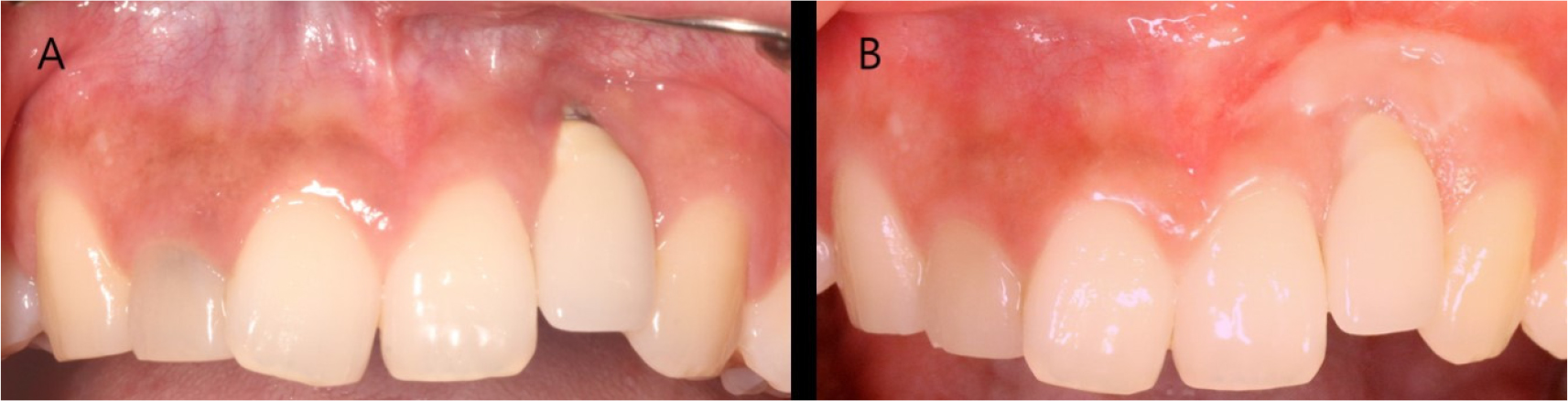
The stitches were removed after 2 weeks. Normal healing took place without any adverse events. Complete abutment coverage did not occur, but the gingiva was thickened through soft tissue augmentation (Fig. 3). At the 3-year follow-up, gingival creeping had occurred. Furthermore, the fixture was not visible because the buccal gingiva had thickened, and peri-implant tissues had remained healthy (Fig. 4).

2. Case #2
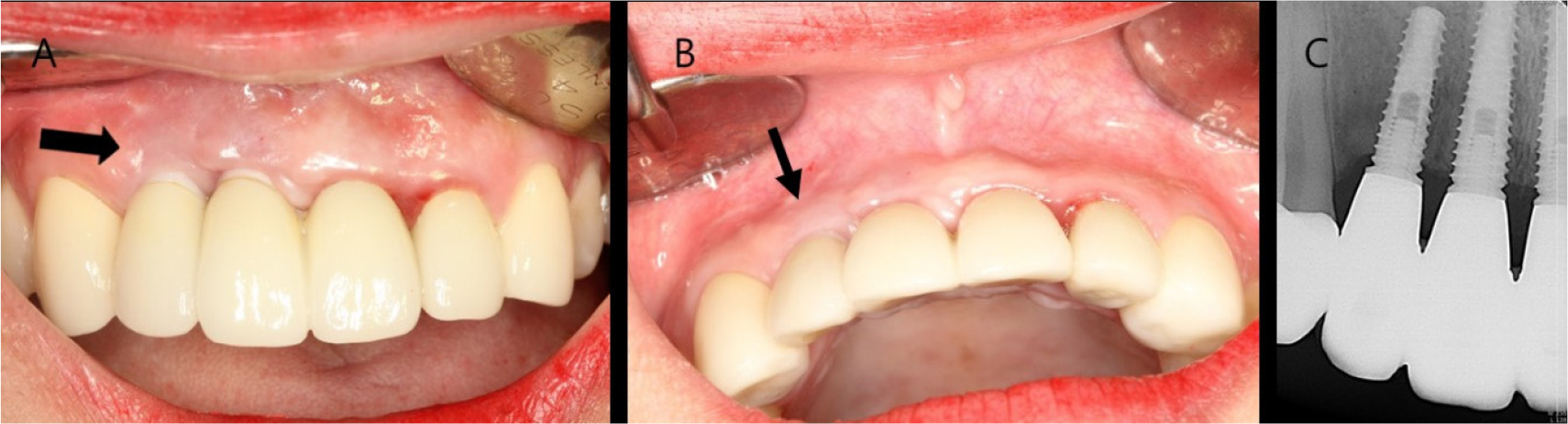
A 23-year-old woman complained of gingival recession and metal exposure around an implant restoration in the left maxillary lateral incisor region. According to the patient’s interview, the root fracture had been caused by trauma 6 years before. The tooth was extracted, and an implant was placed. Clinical examination revealed that the implant had been placed on the buccal and apical side, and the incisal edge of the crown had been formed on the apical side compared to the adjacent teeth. Gingival recession was observed, and the metal platform of implant shoulder was exposed. A normal periodontal pocket and insufficiently attached gingiva were observed on the buccal side (Fig. 5).

The patient was diagnosed with a facial peri-implant soft tissue deficiency of the left maxillary lateral incisor. Soft tissue grafting was planned for gingival coverage of the exposed fixture. A horizontal incision was made around the mucogingival junction, and a partial thickness flap was reflected. The metal of the shoulder part of the buccal inclined fixture was exposed. Epithelized gingival tissue was obtained from the palate. A free gingival graft was sutured on the recipient site. The stitches were removed after 2 weeks. Normal healing took place without any adverse events. Complete metal coverage occurred, but the gingival scars remained (Fig. 6). At the 3-year follow-up, the grafted soft tissue had stably maintained, and peri-implant tissues had remained healthy (Fig. 7).
Ⅲ. Discussion
To prevent PSTD, sufficient consideration should be made before implant placement. We should be fully aware of the factors that increase risk of PSTD. Minimal keratinized mucosa around implants plays a critical role among the factors that cause mucosal recession around implants.4 Additionally, immediately placed implants are associated with a high incidence (9% – 41%) of facial PSTD.5 The risk of inducing PSTD is three times higher when the implant shoulder is positioned buccally than when it is positioned lingually. Cosyn et al. showed an odds ratio of 17.2 for mid-facial PSTD and a buccally positioned implant.6 Neither of our case showing PSTD in the esthetic area had sufficient keratinized gingiva. In case #1, the implant placement was immediate with a thin periodontal biotype, and in case #2, the implant shoulder was buccally positioned.
Many techniques, such as the coronally advanced flap, tunnel, free gingival graft, guided bone regeneration procedure, resubmergence technique, or surgical-prosthetic approach, have been proposed for treating PSTDs.3 They are similar to the surgical procedure for root coverage in gingival recession of the natural teeth. However, the peri-implant periodontium differs from the periodontal tissue around the teeth. Reduced vascularity, lower number of fibroblasts, parallel organization of the connective tissue fibers, and long junctional epithelium, which are characteristic of the peri-implant soft tissue, are more scar tissue that the soft tissue around teeth.7 These anatomical differences may lead to an inferior PSTD coverage compared to the outcomes usually obtained when treating the teeth with the same technique. Therefore, PSTD coverage should comprehensively consider the degree of PSTD, position of buccolingual implant placement, interproximal papilla height, and marginal level of the implant-supported crown.
In case #1, buccal bone dehiscence around the implant occurred after implant placement immediately after tooth extraction and after alveolar bone remodeling. Since it was a thin biotype, mucosa discoloration occurred because of fixture under the mucosa. Through subepithelial connective tissue grafting with a coronally advanced flap, the periodontal biotype was corrected from thin to thick. This surgical procedure has been proposed as the most effective way to treat PSTD in the short and long terms. Maturation of the autologous connective tissue increased the buccal soft tissue thickness and caused a “creeping” phenomenon, showing the improved mean coverage of the dehiscence later rather than sooner postoperatively.8
As in case #2, soft tissue augmentation with submerged healing is recommended when the implant shoulder is biased to the buccal side and the gingival margin of the crown is located apically in relation to the contralateral teeth.3 Delivery of a new implant-supported crown after the surgical procedure can allow exposed metal coverage and an esthetic implant restoration. However, the patient preferred the cost-efficient treatment option, and soft tissue augmentation with free gingival graft alone was sufficient to correct the exposed metal, periodontal biotype and healthy peri-implant tissue.
Soft tissue augmentation and prosthetic treatment alone cannot restore all PSTDs. Implant removal should be considered when, together with the lack of interproximal papilla, the implant head is too buccally displaced, such as implant malpositioning.9,10
Treatment of PSTD may vary depending on the patient’s esthetic requirements. Although fabricating a new prosthesis may be the ideal treatment method, considering the patient’s demand and treatment cost, soft tissue grafting can yield satisfactory results by maintaining healthy and stable soft tissues surrounding the implant.
Ⅳ. Conclusion
The presented cases showed that esthetics were restored and peri-implant soft tissue health was promoted through two soft tissue augmentation techniques, including subepithelial connective tissue grafting with a coronally advanced flap and free gingival grafting, for two patients with PSTD in the esthetic area.
