

Ⅰ. Introduction
Ⅱ. Materials and Methods
1. Ethical statements
2. Participants
3. Surgical procedures
4. Outcome measurements
5. Statistical analysis
Ⅲ. Results
Ⅳ. Discussion
Ⅴ. Conclusion
Ⅰ. Introduction
Tooth extraction in the posterior maxilla can lead to alveolar bone loss due to both maxillary sinus pneumatization and dimensional shrinkage of the ridge, particularly on the buccal side.1,2 These resorptive changes complicate prosthetically driven implant placement and often necessitate invasive augmentation procedures, such as lateral sinus floor elevation, which can increase patient morbidity and surgical complexity.3
Alveolar ridge preservation (ARP) has been proposed as a treatment option for maintaining ridge volume following tooth extraction.4 ARP can reduce the need for invasive surgical approaches and lower the risk of complications during implant placement.5,6 In the posterior maxilla, in particular, ARP may limit sinus pneumatization and crestal bone resorption, thereby reducing the necessity for sinus floor augmentation.7,8,9
There is substantial heterogeneity in the surgical techniques and materials used for ARP.10 Various bone substitutes are widely used in clinical practice, although there remains debate over which material is most effective.11 Block bone substitutes have demonstrated superior space-making and maintenance capabilities compared to particulate bone grafts.12 Deproteinized porcine bone mineral with 10% collagen (DPBM-C) in block form has been introduced recently;13 however, few studies have evaluated the therapeutic relevance of porcine-derived soft block bone for ARP.
Therefore, the objective of this study was to investigate whether ARP using a porcine-derived soft block bone substitute could minimize vertical crestal bone changes and reduce the need for invasive sinus augmentation procedures in the posterior maxilla.
Ⅱ. Materials and Methods
1. Ethical statements
This retrospective and follow-up study was approved by Korea National Institute for Bioethics Policy (P01-202404-01-013) and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines on damaged maxillary molars.14
2. Participants
A total of 37 patients who had received ARP using deproteinized porcine bone mineral with 10% collagen (Legograft®; Purgo, Seongnam, Korea) on damaged maxillary molar extraction sockets and implant placement at the Department of Periodontology, Daejeon Dental Hospital, Wonkwang University between February 2019 and August 2022 were screened retrospectively.
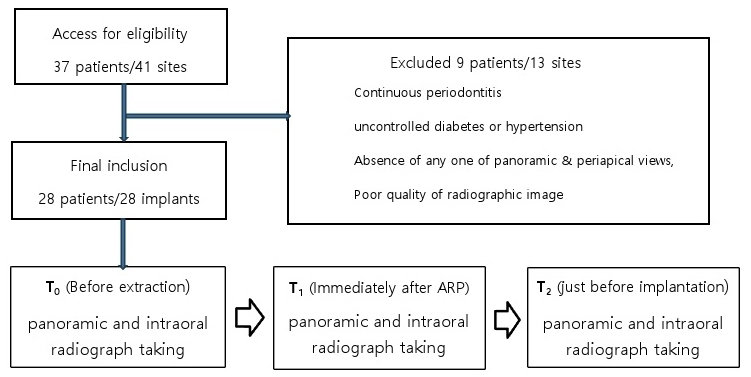
The inclusion criteria were as follows: (1) minimum age of 18 years, (2) periodontally healthy, (3) healthy or well-controlled systemic diseases, and (4) presence of panoramic and periapical views obtained before extraction, immediately after extraction with ARP, and just before implant placement. The exclusion criteria were as follows: (1) continuous periodontitis, (2) uncontrolled diabetes or hypertension, (3) absence of any one of the panoramic and periapical views, (4) radiographic images of insufficient quality for assessing associated factors, and (5) ARP sites where implants could not be placed.
Finally, a total of 28 extraction sockets of each patient were enrolled in this study. The flowchart of this study is presented in Fig. 1.
3. Surgical procedures
Extractions were performed using elevators and forceps with great care. After extraction, sockets were carefully debrided to remove all granulation tissue. The extraction sockets were then filled with deproteinized porcine bone mineral with 10% collagen (Legograft®; Purgo), without flap elevation, and covered with a collagen membrane of Remaix™ (Matricel GmbH, Herzogenrath, Germany) or Ossix Plus® (Datum Dental Biotech, Telrad, Israel). Primary wound closure was not attempted. The ARP site was stabilized using a 4–0 non-absorbable polytetrafluoroethylene monofilament (Biotex; Purgo) with interrupted and hidden X sutures (Fig. 2). Patients were instructed to rinse twice daily with a chlorhexidine gluconate solution and were prescribed analgesics and antibiotics for 5 days. All patients were followed up 7 to 10 days after the procedure for the removal of suture materials.
After at least 5 months of healing, every site was reentered to insert dental implants (Osstem TS III SA; Osstem Implant Co., Busan, Korea, and Dentium Superline II; Dentium Co., Seoul, Korea). Additional sinus elevation procedures were performed if necessary.
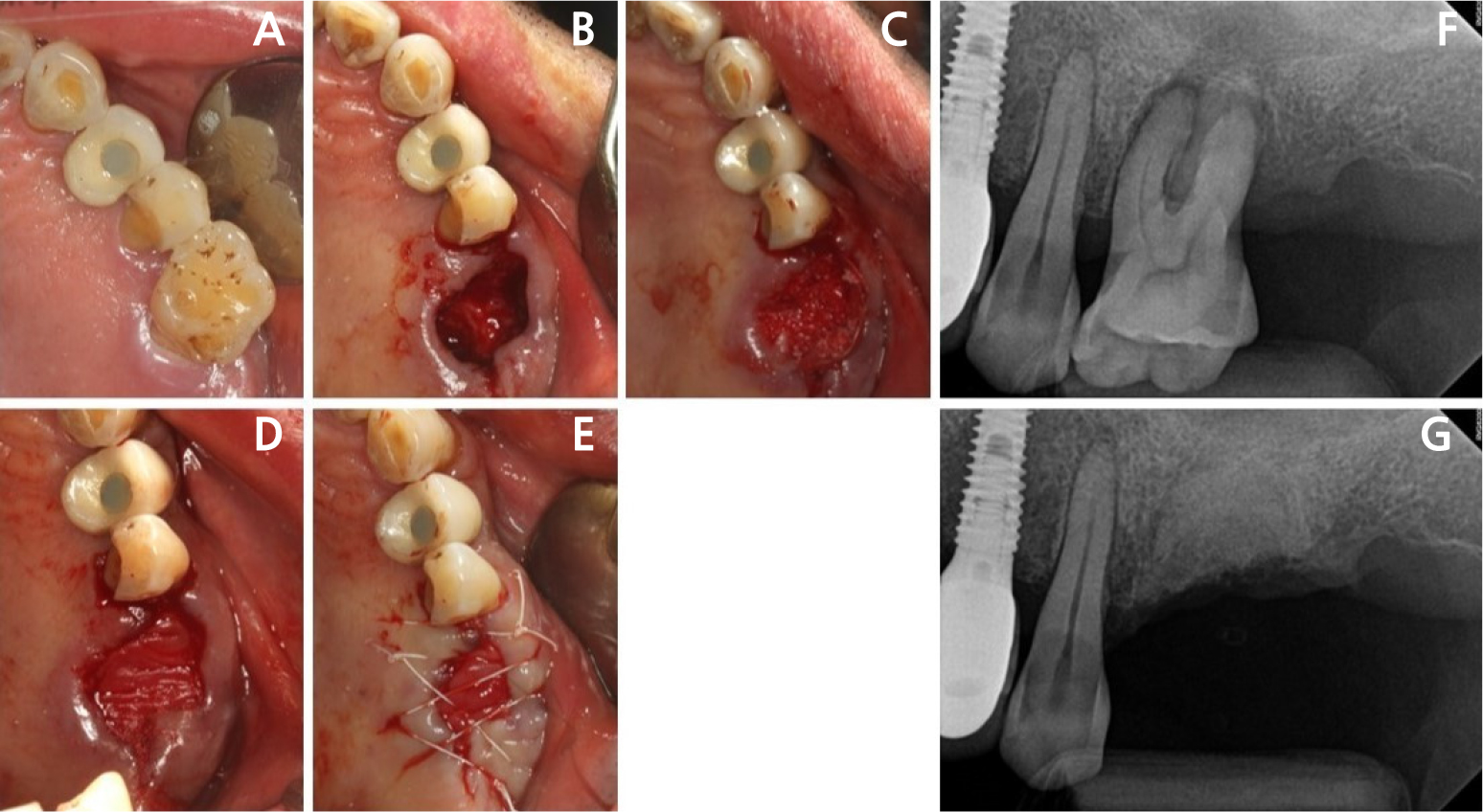
Fig. 2
Representative intraoral photographs and periapical radiographs. The severely damaged maxillary first molar (A) underwent ARP (B, C). The grafted site is covered with Remaix (Matricel GmbH, Herzogenrath, Germany) (D) and then sutured (E). (F) and (G) Periapical radiographs obtained before extraction with ARP and immediately after ARP, respectively.
4. Outcome measurements
4.1. Radiographic analysis
Standard periapical and panoramic radiograph images were obtained for each patient before extraction (T0), immediately after extraction and ARP (T1), and shortly before implant placement (T2), using a PCH-2500® (Vatech, Hwaseong, Korea). Radiographic measurements were conducted using INFINITT® (Infinitt Healthcare, Seoul, Korea) software and medical imaging software (OsiriX version 11.0; Pixmeo SARL, Geneva, Switzerland). To correct for distortion in the periapical radiographs, measurements of landmark structures, such as the treated or adjacent teeth, prostheses, and anatomical features, were used to adjust the values, based on the periapical image with the least inclination of the tooth axis.
CBCT imaging (CS 8100 3D®; Carestream, Rochester, United States) was performed using I-mode with an 80 × 90 mm field of view (FOV), voxel size of 0.15 mm, and 90 kV shortly before implant placement (T2). OnDemand3D® software (Cybermed, Seoul, Korea) was used for DICOM file reconstruction.
Most measurements were made on periapical radiographs. The reference line for the measurements was the extended line of the crest levels of the adjacent neighboring teeth or the crest levels between the adjacent tooth and the adjacent extraction socket (in cases of multiple extractions). All measurements were performed by a single investigator. Intra-class correlation coefficients were used to evaluate intra-examiner repeatability on 10 pairs of randomly selected recordings. All intra-examiner repeatability coefficients exceeded 0.95. The measurement system had a precision of 0.01 mm.
The following parameters were measured as described in the study by Jung et al.15 (Fig. 3):
(1) Sinus floor level (SFL): vertical distance between the reference line and the sinus floor at the center of the extraction socket.
(2) Bone crest level (BCL): vertical distance between the reference line and the crestal bone at the center of the extraction socket.
(3) Residual alveolar bone height (RBH): vertical distance between the sinus floor and bone crest.
(4) ΔSFL, ΔBCL, and ΔRBH: changes in SFL, BCL, and RBH between T0 and T2.
The ΔSFL represents the amount of sinus pneumatization, and ΔBCL indicates crestal bone shrinkage, and ΔRBH reflects bone gain.
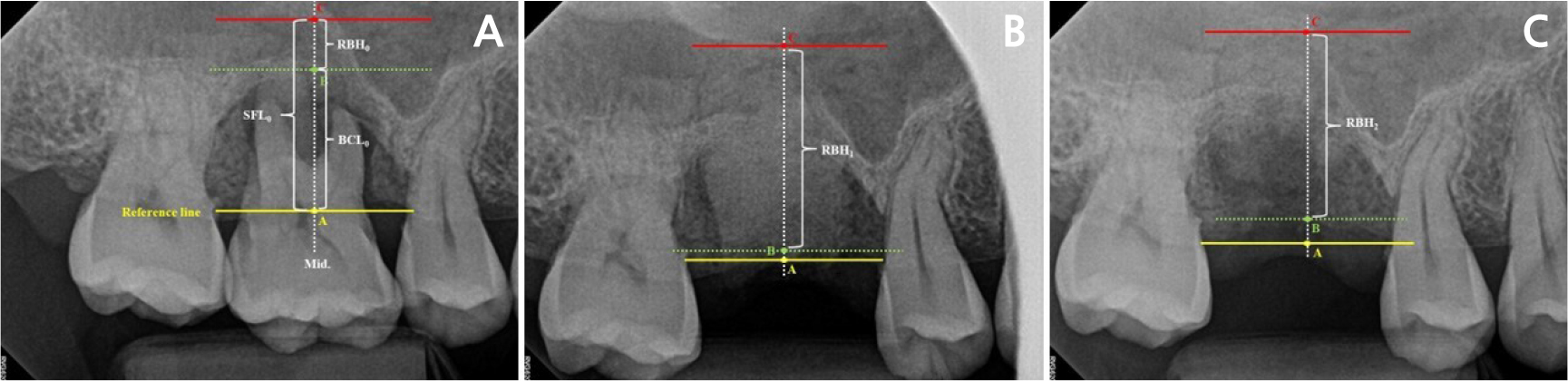
Fig. 3
Radiographic measurements. For vertical measurements, the reference line (yellow) was defined as the extended line of the crest levels on each side, and the midline (middle, white dotted) was defined as the line passing through the center-most area of the extraction socket. A (yellow), B (green), and C (red) represent the contact points formed by the reference line and midline. SFL and BCL were measured from A to C and A to B, respectively. RBH was measured from B to C. Yellow A, green B, and red C represent the RBHs at T0, T1, and T2, respectively (RBH0, RBH1, and RBH2). T0: before extraction; T1: immediately after extraction and ARP; T2: shortly before implant placement.
4.2. Additional sinus augmentation procedures
Additional sinus augmentation procedures performed either prior to or during implant placement were identified in computerized dental records. The decision to perform additional sinus elevation and the choice of surgical approach were based on CBCT image analysis. The following types of sinus augmentation procedures were noted:
1. Lateral sinus floor elevation (LSFE): two-stage and one-stage techniques via the lateral approach
2. Transcrestal sinus floor elevation (TSFE): osteotome sinus floor elevation with or without bone graft.
4.3. Implant survival
Implant survival was defined as the presence of the implant at the most recent follow-up visit with no signs indicating the need for removal. Implant failure was defined as absence of the implant in the oral cavity for any reason. Implant survival and failure were assessed using the most recent radiographs. The average follow-up period was 4.26 years (range: 2 to 5 years).
5. Statistical analysis
All data were analyzed using SPSS version 29.0 (SPSS Inc.; Chicago, IL, Unites States). The mean values and standard deviations of SFL, BCL, and RBH were calculated. Normality was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Based on these results, ΔSFL between T0 and T1 was the only variable for which a non-parametric test was applied. Statistical analysis was performed using the Wilcoxon signed-rank test and paired t-tests to evaluate significant changes in SFL, BCL, and RBH. A p-value of < .05 was considered statistically significant.
Ⅲ. Results
A total of 28 implants from 28 patients (12 males and 16 females), aged 44 to 70 years (mean age: 55.56 ± 8.69), were included in this study. The mean interval between ARP (T1) and implant placement (T2) was 7.06 ± 1.78 months, ranging from 5 to 11 months. The study included six maxillary second molars and 22 first molars (Table 1).
Table 1.
Demographic characteristics of patients and surgical sites (n=28)
Remaix (Matricel GmbH, Herzogenrath, Germany) and Ossix Plus®(Datum Dental Biotech, Telrad, Israel).
None of the 28 cases that underwent ARP and implant placement showed serious or adverse complications. The survival rates at both the implant and patient levels were 100%, with no implant failures observed during the latest follow-up (average: 4.26 years).
The results of radiographic measurements are shown in Table 2. ΔSFL and ΔBCL between T2 and T1 were 0.16 ± 0.08 mm and 2.20 ± 1.15 mm, respectively. RBH increased by 7.44 ± 1.95 mm between T0 and T1, and ΔRBH between T0 and T2 was 5.01 ± 1.65 mm. SFL significantly decreased between T0 and T1, and between T1 and T2 (p = .008 and p < .001, respectively). BCL decreased between T0 and T1, and increased between T1 and T2; both changes were statistically significant (p < .001 for both). There was a significant increase in RBH between T0 and T1 (p < .001) and a significant decrease between T1 and T2 (p < .001). ΔRBH significantly increased between T0 and T2 (p < .001).
Table 2.
Measurements of sinus floor level, bone crest level, and residual bone height
SFL: Sinus floor level; BCL: Bone crest level; RBH: Residual bone height.
T0: before extraction; T1: immediately after extraction and ARP; T2: shortly before implant placement.
Of the 28 cases, 18 implants (64.29%) needed additional TSFE, and three implants (10.71%) required LSFE procedures. No additional sinus augmentation procedure was needed in seven cases (25.0%).
Ⅳ. Discussion
This retrospective study examined the clinical effectiveness of ARP using DPBM-C in the posterior maxilla. There was a significant increase in residual bone height compared to baseline after ARP. Although some bone loss occurred between the ARP and implant placement, ARP was effective in maintaining bone height. However, in most cases, ARP could not fully eliminate the need for additional sinus floor augmentation procedures.
ARP has been shown to effectively reduce the need for additional augmentation procedures prior to or during implant placement, especially in the maxilla.16 Barone et al.17 reported that three out of 20 implants in the grafted group required further bone augmentation during implantation. Although the lateral approach for sinus augmentation is effective and associated with high implant survival and success rates, it carries a high risk of complications, such as sinus membrane perforation and excessive pain or swelling.18,19 A recent systematic review reported that the need for additional augmentation was 15% lower following ARP compared to spontaneous healing.6 We could not obtain data on the extent to which ARP reduced the need for additional augmentation compared to spontaneous healing. In this study, additional grafting was required in 75% of ARP sites. Eighteen implants (64.29%) required additional TSFE, and three implants (10.71%) required LSFE procedures. The mean bone height under the sinus floor at T0 was less than 3 mm, prompting most clinicians to choose the lateral approach for implant placement. Although there is a limitation in not having a control group, ARP appeared to positively affect bone volume preservation and reduce the need for more aggressive sinus augmentation surgery.
Autogenous bone is regarded as the “gold standard” owing to its osteogenic, osteoinductive, and osteoconductive properties. Nevertheless, its high resorption rate, donor site morbidity,20 and the limited amount of bone available for harvesting are significant limitations. As an alternative, allografts, xenografts, and alloplastic materials are widely used in clinical practice, although there is ongoing debate regarding which is superior.11 Block bone substitutes have demonstrated better space-making and maintenance capabilities than particulate bone substitutes—an essential requirement for predictable bone regeneration and favorable long-term results in GBR.12 Among xenogeneic block bone substitutes, deproteinized bovine bone mineral with 10% collagen (DBBM-C), commonly used for alveolar ridge preservation, shows good adaptability and favorable outcomes in both horizontal and vertical bone defects.21,22,23 To the best of our knowledge, no prior study has evaluated the therapeutic relevance of deproteinized porcine bone mineral with 10% collagen (DPBM-C) for ARP.
Several animal and clinical trials have demonstrated that DPBM is not inferior to DBBM in clinical and histological outcomes.24,25,26 Furthermore, DPBM carries a low risk of prion disease transmission.26,27 Bae et al. investigated the histological outcomes of DPBM and DBBM in rat calvarial defects and found no significant differences in new bone area and volume, osteogenic ability, or gene expression between the two groups.24 Comparative randomized clinical trials of DPBM and DBBM for ARP of compromised and damaged extraction sockets found no significant differences in hard and soft tissue dimensions, histologic variables, or biocompatibility.25,27,28 In this study, RBH significantly increased compared to baseline following ARP using DPBM with 10% collagen.
In our study, survival rates of implants at both the patient and fixture levels were 100% during the average follow-up period of 4.26 years. However, there were two ARP sites (excluded) where implant could not be placed because of insufficient initial stability. Both were extraction sockets of second molars adjacent to first molars that had undergone ARP. The two patients were satisfied with single implants in the posterior area; thus, no further attempts at implant placement were made. Although ARP appears effective in maintaining alveolar bone volume, further research is needed to evaluate the quality of the bone formed through the ARP procedure.
There are a few limitations to this study. First, a major limitation was the absence of a naturally healed control group. Second, owing to the retrospective nature of this study, various variables, such as the amount of graft material, type of collagen membrane, timing between tooth extraction and implant placement, and implant system, could not be controlled, resulting in increased variability. Third, ARP and implant placement were performed by surgeons with differing levels of clinical experience, which introduced operator variability that could not be controlled. Fourth, the relatively short observation period and the small number of patients must be taken into consideration, and the findings should be interpreted with caution. Finally, the absence of standardized devices such as plastic stents may have introduced measurement errors.
Because of cost considerations and concerns about radiation exposure, CBCT is not routinely obtained in everyday dental practice. In most cases, only periapical and panoramic radiographs were taken before extraction (T0) and immediately after extraction and ARP (T1), with CBCT performed only after at least a 5-month healing period (T2). Therefore, radiographic measurements were mainly based on periapical images, with some based on panoramic images. Considering the limitations of two-dimensional imaging, a larger-scale prospective study is needed, with CBCT performed at all key time points during ARP and implant placement.
Ⅴ. Conclusion
Within the limitations of this study, it was observed that ARP procedures performed in damaged posterior maxillary molar extraction sockets may help reduce the need for more invasive sinus augmentation procedures. This suggests that ARP could be a valuable alternative in certain clinical scenarios, potentially reducing the need for more complex procedures.
