

Ⅰ. Introduction
Several attempts have been made to improve the accuracy of dental implant placement using computer-guided surgical templates and computed tomography (CT).1 Previously, surgical guides in implant dentistry were fabricated using analog stone casts, which did not reflect information such as mucosal thickness, basal bone morphology, and anatomical structures. They were often unstable intraoperatively due to interference from oral soft tissues.2 With the recent widespread use of CT and intraoral scanners, computer-assisted surgical planning has enabled superior biomechanical and esthetic outcomes, even in cases with anatomical limitations, insufficient bone volume, or low bone density.2
Although implant placement without surgical guides is feasible in most clinical situations, computer-assisted planning and guided placement significantly reduce the risk of damage to adjacent anatomical structures.3 Two main approaches have been proposed for incorporating three-dimensional (3D) imaging into implant surgery: stereolithographic (STL) surgical guides and dynamic optical navigation systems.4 While navigation-assisted implant surgery has yielded inconsistent results regarding accuracy, the use of 3D-printed STL surgical guides has become more widespread in clinical practice.5
Implant guides are categorized based on their support type as tooth-supported, mucosa-supported, and bone-supported designs.6 In fully edentulous cases, mucosa- or bone-supported guides are generally employed, while tooth-supported guides are preferred in patients with partial edentulism.7 The accuracy and stability of tooth-supported guides are widely acknowledged to decrease as the number of remaining teeth reduces.8 However, few studies have investigated the extent of this reduction in patients with partial edentulism and only a few teeth, particularly with respect to how the number of supporting teeth affects the stability and accuracy of surgical guides.
Therefore, this study aims to evaluate the accuracy of computer-aided design and manufacturing (CAD/CAM)-fabricated STL surgical guides based on the number of supporting teeth in patients with partial edentulism undergoing implant placement.
Ⅱ. Materials and Methods
Maxillary and mandibular models (BASIC; Korea Model Technology, Guri, Korea) were fabricated using five representative dentition patterns. These models underwent CT scanning and were superimposed with intraoral scan data to generate 3D composite models. Ten models were assigned to each group.
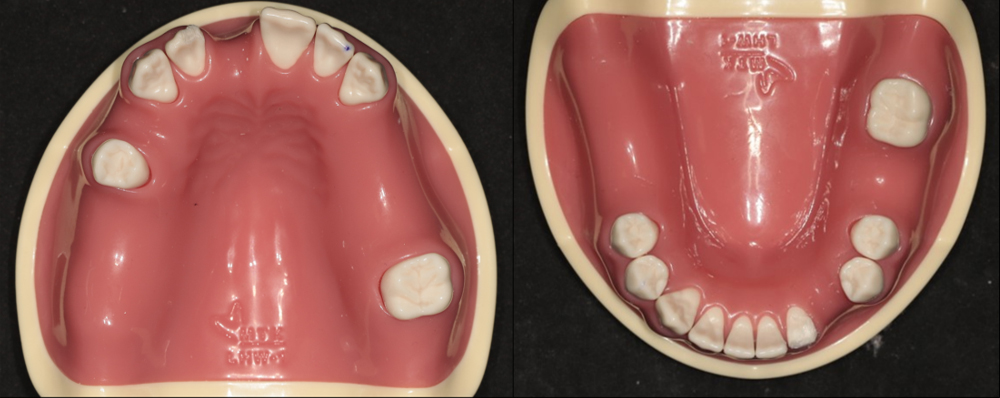
The experimental group consisted of maxillary and mandibular arches, with only three remaining teeth per arch, distributed in a triangular pattern (anterior, left posterior, and right posterior) without adjacent contacts (Fig. 1). The control group comprised arches with seven or more remaining teeth per arch, allowing for adjacency, while maintaining a triangular distribution of anterior, left posterior, and right posterior teeth (Fig. 2). For virtual implant placement surgery, STL guide fabrication, navigation procedures, and rapid prototyping models were subjected to CT scanning. CT imaging was performed using a Siemens Sensation 64 system (Siemens AG, Erlangen, Germany) with the following parameters: pixel size 0.4375 mm, resolution 512 × 512, field of view 22.40 cm, reconstruction algorithm H60f, and slice thickness of 0.6 mm.
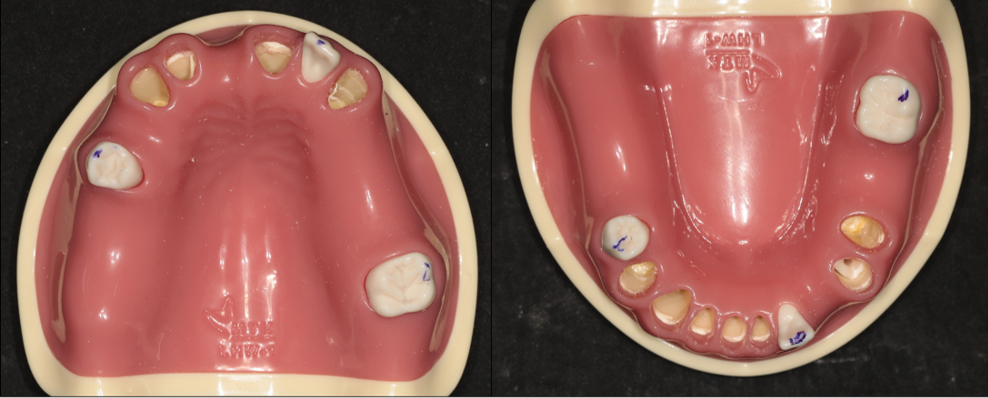
Fig. 1
In the experimental model, three teeth (blue markings) support the surgical guide. Five maxillary and five mandibular models are created, each incorporating slight variations in tooth morphology. These variations are generated by randomly removing portions of the dental crowns, resulting in distinct model configurations.
Each model was scanned using a desktop optical scanner (Identica T500; Medit, Seoul, Korea) to obtain high-resolution tooth surface data, replicating the clinical workflow for surgical guide fabrication. The scan data were superimposed onto CT datasets based on occlusal surfaces, replacing the CT-derived tooth structures with higher-resolution optical scan data. In the surgical experiments, implant fixtures with a diameter of 4.5 mm and a length of 10 mm (SS type; Osstem, Seoul, Korea) were used consistently across all trials, with placement performed at the edentulous sites of the jaw models.
In the experimental and control groups, implant placement was performed at edentulous sites, with three implant sites designated per model: one anterior site and one posterior site on the left and right sides of the maxilla and mandible, respectively. In the maxillary model, the implant fixtures were inserted into the right central incisor (#11), first molar (#16), and left second premolar (#25). In the mandibular model, implant fixtures were placed in the left canine (#33), first molar (#36), and right first molar (#46).
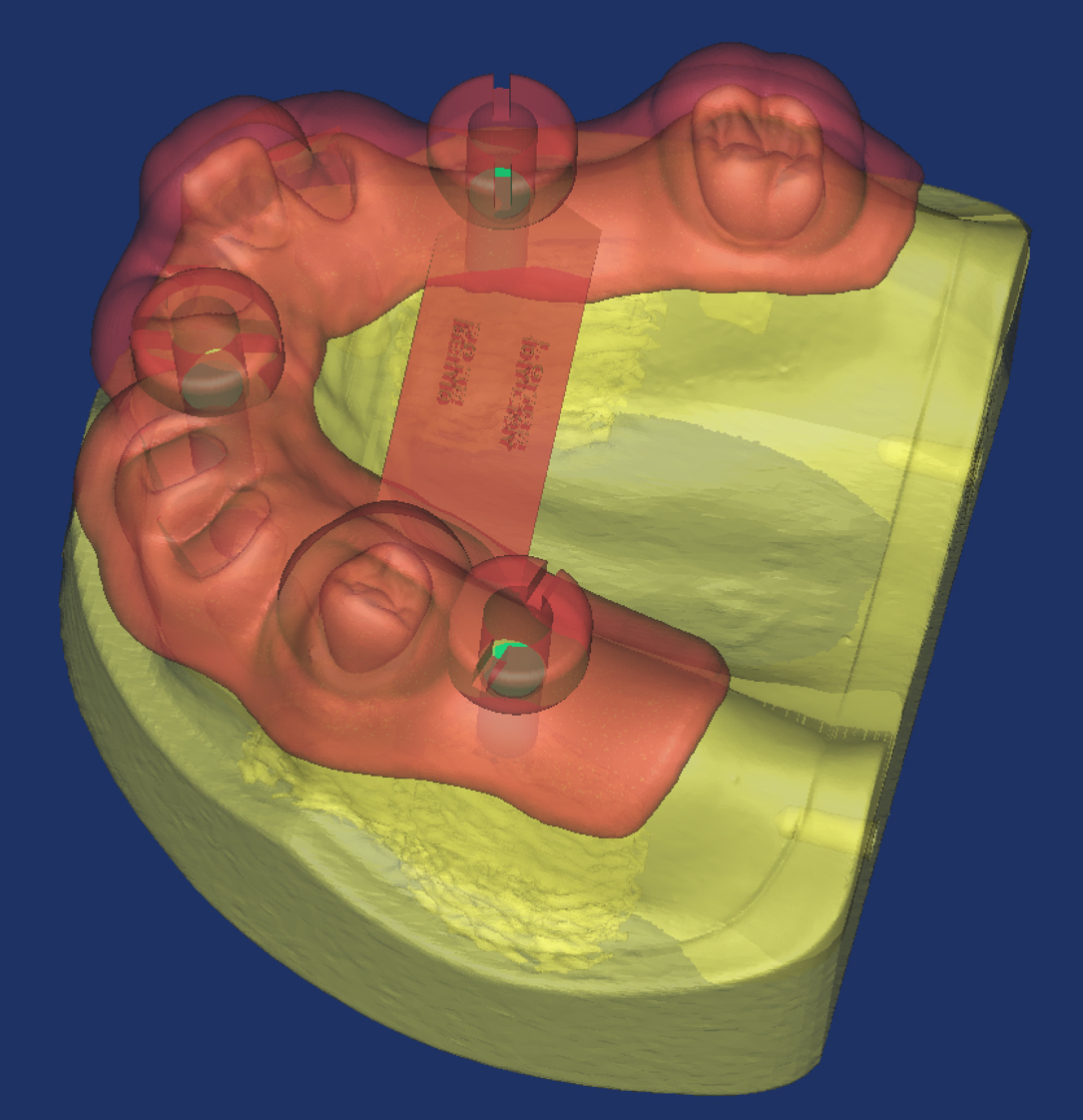
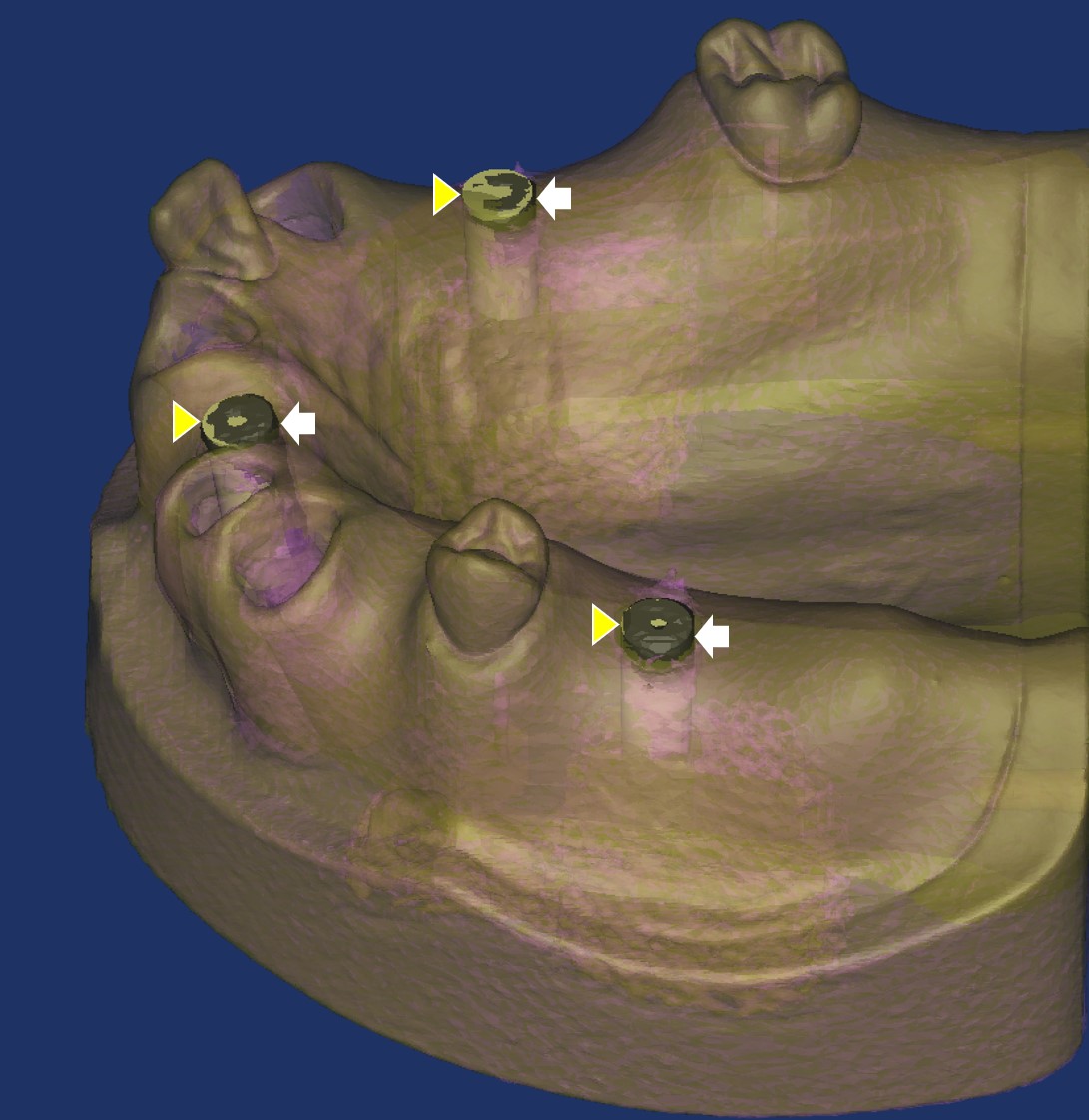
The simulated surgery and guide fabrication process involved importing preoperative CT digital imaging and communications in medicine data into implant planning software, where 3D dental models were superimposed with intraoral scan data. Virtual implant placement was performed using software simulation functions. CAD data for the implants were generated using Mimics software (version 14.0; Materialise, Leuven, Belgium) and exported for surgical guide fabrication. The datasets were submitted in the Osstem guide system (Osstem, Seoul, Korea) format, and STL guides were fabricated accordingly (Fig. 3). Final implant placement was performed using 3D-printed surgical guides (OneGuide; Osstem, Seoul, Korea), which replicated clinical implant surgery (Fig. 4).

For surgical guide application, the guide was positioned at the designated implant sites, and osteotomies were performed using guide sleeves, followed by fixture placement. Drilling was conducted through predetermined guide sleeves with sequential enlargement of drill diameters to prepare the osteotomy, ensuring that implant placement conformed to the planned angulation and depth defined by the guide. To ensure an adequate sample size, three implants were placed in each edentulous arch, resulting in a minimum of 30 implants per group. Following implant placement using both methods, each model was rescanned using the same CT acquisition protocol applied during the preoperative stage (Figs. 5 and 6).


To compare deviations between the simulated and actual surgeries, postoperative CT datasets were superimposed onto the preoperative data within the analysis software. Positional differences between the virtually planned implants and placed fixtures were measured (Fig. 7). Reference points included the centroid of the coronal surface, centroid of the apical surface, coronal and apical planes, and central axis connecting the coronal and apical centroids of each fixture. Measurements included linear deviations (the shortest distance from the central axis) and angular deviations between the planned and actual implants. Vertical discrepancies were calculated as the distance between the coronal plane and coronal centroid, and between the apical plane and apical centroid. Horizontal discrepancies were assessed by measuring the differences between the coronal centroids and between the apical centroids of the planned and placed implants. Each parameter was evaluated and compared between the experimental and control groups.
Preoperative and postoperative values (postoperative – preoperative) were compared using independent t-tests. Statistical analyses were performed using IBM SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < .05.
Ⅲ. Results
No statistically significant differences were observed between the groups with respect to the number of supporting teeth (Tables 1, 2, 3, 4, 5, 6, 7, and 8). When evaluating the minimum distance between the two central axes, the mean error was 0.16 ± 0.17 mm for guides supported by seven or more teeth and 0.20 ± 0.12 mm for guides supported by three teeth, showing no significant difference between the two groups.
Table 1.
Three-dimensional distant error between the top surface area of the implant and simulation fixture (mm)
Table 2.
Three-dimensional distant error between the apex surface area of the implant and simulation fixture (mm)
Table 3.
Minimum distance between the 2 centerline of the implant and simulation fixture (mm)
Table 4.
Angular error between the 2 centerline of the implant and simulation fixture (°)
Table 5.
Vertical distant error between the top surface area of the implant and simulation fixture (mm)
Table 6.
Horizontal distant error between the top surface area of the implant and simulation fixture (mm)
Table 7.
Vertical distant error between the apex surface area of the implant and simulation fixture (mm)
Table 8.
Horizontal distant error between the apex surface area of the implant and simulation fixture (mm)
Assessment of angular deviation of the implant axis showed a mean error of 3.02 ± 2.05° in the group with guides supported by seven or more teeth and 3.41 ± 2.64° in the group with guides supported by three teeth, showing no statistically significant difference.
For horizontal distance error of the coronal centroids, the mean error was 0.34 ± 0.21 mm in the group supported by seven or more teeth and 0.31 ± 0.15 mm in the group supported by three teeth, showing no statistically significant difference.
For vertical deviation of the coronal centroids, the mean error was 0.47 ± 0.31 mm in the group supported by seven or more teeth and 0.43 ± 0.30 mm in the group supported by three teeth, with no statistically significant difference between the two groups.
Ⅳ. Discussion
This study investigated the accuracy of implant placement using surgical guides supported by three versus seven or more remaining teeth. The results showed no statistically significant differences in placement accuracy between the two groups in terms of axial angular deviation and center-point distance between the actual implant position and the preoperatively planned CAD-based implant position.
A meta-analysis by Tahmaseb et al.9 reported mean deviations observed in partially edentulous patients undergoing guided implant surgery of 0.9 mm at the coronal level, 1.2 mm at the apical level, and a 3.3°angular deviation. In this study, the experimental group demonstrated coronal, apical, and angular deviations of 0.56 ± 0.28 mm, 0.84 ± 0.55 mm, and 3.40 ± 2.63°, respectively. Although this investigation was conducted in vitro using dental models, all three parameters were within the ranges reported in the meta-analysis. These findings suggest that, contrary to the prevailing concern that fewer supporting teeth would compromise guide accuracy, clinically acceptable implant placement accuracy can still be achieved with digital surgical guides even when only a limited number of supporting teeth are present.
Given that this study was conducted in vitro using dental models, factors commonly encountered in clinical situations, such as tooth mobility, soft tissue characteristics, saliva, and patient movement, were not represented, which constitutes a limitation. In the experimental group, the maxillary and mandibular models retained three non-adjacent teeth distributed in a triangular pattern (anterior, left posterior, and right posterior). In the control group, each arch had seven or more teeth, including adjacent teeth, while maintaining a similar triangular distribution across the anterior and bilateral posterior regions. Furthermore, because the surgical guides were designed to achieve triangular stabilization across the anterior, premolar, and molar regions, the results cannot be directly generalized to cases where three-point stabilization was obtained only in the anterior region. Additional studies are needed to evaluate differences in accuracy according to various residual tooth distribution patterns. Previous reports have indicated that posteriorly supported guides demonstrate greater accuracy than anteriorly supported guides, highlighting the need for systematic comparative studies under diverse clinical scenarios, such as anterior-only or posterior-only support.8
Recent advances in 3D CT have facilitated the development of 3D skeletal analysis and simulation surgery, enabling more precise diagnosis and surgical planning. In dental implant surgery, 3D simulation is also increasingly performed, with 3D-printed surgical guides subsequently applied during the procedure. The outcomes of preoperative simulation surgery must be accurately reflected intraoperatively, particularly with respect to the osteotomy site, angulation, and depth during the initial drilling stage of implant placement. Consequently, STL stent devices are commonly used to guide these parameters.10, 11
However, the use of STL surgical guides and optical navigation systems for surgical planning based on 3D imaging presents certain limitations.5 For instance, errors may occur during the fabrication of surgical guides using CAD/CAM technology, and when surgical stents are employed, their stability is a critical factor in minimizing such errors. Some investigators have reported that tooth-supported stents provide greater stability than tooth–mucosa-supported devices, whereas others have suggested that broader support areas may yield improved outcomes in patients with full edentulism than in patients with partial edentulism. In this study, standardized training models were modified, which likely provided more favorable conditions for implant placement than those encountered in clinical practice. Accordingly, in actual clinical research, additional sources of error beyond those observed in this experimental model should be anticipated.
The use of surgical guides for implant placement has certain disadvantages, including the need for prefabrication and the potential bulk of the device, which may restrict mouth opening and complicate implant placement in posterior regions. Recently, in addition to the use of prefabricated guides based on preoperative simulation surgery, real-time computer-assisted navigation surgery has been introduced for implant placement.4 Navigation surgery enables the intraoperative utilization of preoperative imaging data, allowing surgeons to visualize critical anatomical structures that are otherwise difficult to identify with the naked eye. This capability facilitates minimally invasive procedures and ensures accurate adherence to preoperative treatment plans. Consequently, the application of navigation systems has expanded across various surgical fields and is increasingly adopted in oral and maxillofacial surgeries, including dental implant surgeries.
Whether a navigation system or a 3D-printed surgical guide is used, both methods rely on CT imaging. In this study, multislice CT (MSCT) was used for image acquisition. Recently, cone-beam CT (CBCT), which involves lower radiation exposure, has become increasingly prevalent and is gradually replacing conventional imaging modalities for the head and neck region. Although CBCT has limitations related to its restricted field of view, it is particularly suitable for mandibular imaging, given the mandible’s anatomical dimensions and morphology, and related research continues to advance.12 However, CBCT images may contain artifacts that partially obscure anatomical structures. Compared with MSCT, CBCT is generally considered clinically acceptable for 3D image reconstruction, although its accuracy may be inferior. Although MSCT was employed in this study, the growing clinical applicability of CBCT in oral and maxillofacial surgery suggests that future research based on CBCT is warranted.13
In dedicated navigation systems for implant surgery, parameters such as the length and angulation of surgical instruments, including handpieces and burs, are preregistered, which is thought to reduce errors arising from registration inaccuracies. Navigation systems are particularly advantageous in patients with edentulism, in whom reliable intraoral anatomical landmarks are often missing. However, several limitations have been reported, including potential errors during CT data conversion and reduced precision of navigation devices.14 Furthermore, because many dentists are unfamiliar with navigation systems, the multiple registration steps involved may introduce additional errors. The bulkiness of the equipment also poses challenges for its use under local anesthesia in dental office settings. Despite ongoing technological advancements, the high cost of navigation systems remains a significant barrier, thereby limiting their widespread use compared with conventionally prefabricated surgical stents for implant placement.5 If future technological developments result in affordable navigation systems suitable for routine outpatient dental practice, further studies involving multiple implant placements in actual patient jaws will be warranted.
Research on surgical guide systems currently in widespread clinical use is essential, as ongoing studies regarding implant placement sites and guide applications are expected to establish protocols that enable more efficient and accurate surgical outcomes. These findings suggest that when the residual teeth are periodontally healthy and morphologically intact, tooth-supported digital guides may be safely applied, even with a limited number of supporting teeth. This can reduce the unnecessary use of auxiliary fixation devices, thereby saving time and cost. Conversely, when residual teeth exhibit mobility due to periodontal disease, guide stability may be compromised, thereby increasing the risk of reduced accuracy. In such situations, additional stabilization methods, such as fixation pins or alternative reinforcement techniques, should be considered.15 Furthermore, when fewer than three teeth remain, making tripod stabilization difficult, or in unilateral free-end situations, additional measures to enhance guide stability are likely necessary.16 In clinical practice, reduced accuracy is highly probable when residual teeth are mobile or clustered on one side. Therefore, strategies to reinforce guide stability must be incorporated into treatment plans.
Ⅴ. Conclusion
This in vitro study demonstrated that using tooth-supported CAD/CAM surgical guides for implant placement in partially edentulous cases with only three remaining teeth resulted in no clinically significant deviations. Although the study was conducted under experimental rather than clinical conditions, the findings indicate that surgical guides supported by as few as three non-adjacent teeth can achieve stability comparable to that of guides supported by a greater number of teeth.
