

Ⅰ. Introduction
Alveolar ridge preservation (ARP) is performed to reduce alveolar atrophy after tooth extraction. In 2012, Tan et al. reported that post-extraction bone remodeling reduces the horizontal (3.79 ± 0.23 mm) and vertical (1.24 ± 0.11 mm) dimensions.1 It causes consideration of guided bone regeneration (GBR) or represents an unfavorable position of the implant aesthetically and functionally. Accordingly, ARP using various materials and flap management reduces alveolar bone contraction after tooth extraction.2,3
Among the various surgical techniques of ARP, open healing ARP applies deproteinized bovine bone mineral (DBBM) to the extraction socket, covering the coronal part of the extraction socket using a native bilayer collagen matrix (NBCM) without primary closure,4 and performs hidden X suture.5This procedure does not require high-level soft tissue manipulation to cover the extraction socket. Thus, the surgical difficulty is not high, and the morbidity is lower than that associated with primary closure. However, there are concerns regarding infection or material loss through the opening of the extraction socket. However, a retrospective study using open-healing ARP in 297 compromised sockets showed 99.3% safety in relation to infection.6In addition, the lack of keratinized gingiva due to coronal displacement of the mucogingival junction to achieve primary closure can also be avoided.4,7,8
Among the implant placement timings during the healing procedure after tooth extraction, Schulte et al. described the immediate implant placement.9 Its survival rate is not statistically significantly different from that of delayed implant placement.10 Nevertheless, the immediate implant placement has the shortest treatment period among the four types of healing procedures.11 However, immediate implant placement makes it difficult to predict changes in soft and hard tissues, and it is often difficult to achieve primary implant stability.12
We hypothesized that if primary stability, a common requirement for both ARP and immediate implant placement, could be achieved, the simultaneous implementation of both procedures would be able to take advantage of each procedure. To the best of our knowledge, there are no studies in which open-healing ARP was performed simultaneously with immediate implant placement in the molar region. Thus, the purpose of this case report was to evaluate the effectiveness of immediate implant placement with open-healing alveolar ridge preservation (iARP) in the molar region.
Ⅱ. Case report
All patients were informed of the operative procedure and possible risks, and the research protocol was approved by the Ethical Committee of the Dankook University Dental Hospital, Korea (H-1412/012/002).
1. Case 1
A 68-year-old female patient with well-controlled diabetes mellitus presented to the Department of Periodontology at Dankook University Dental Hospital complaining of mobility of the lower left molar.
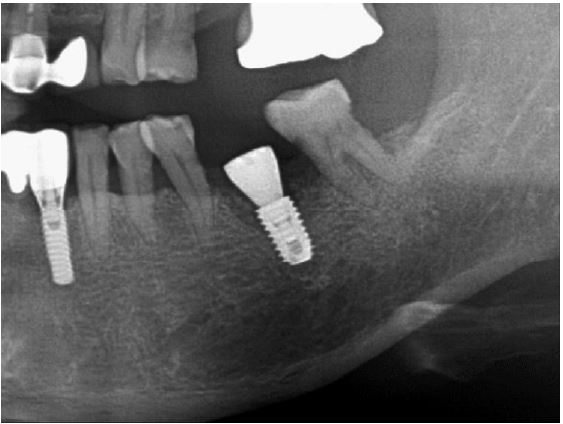
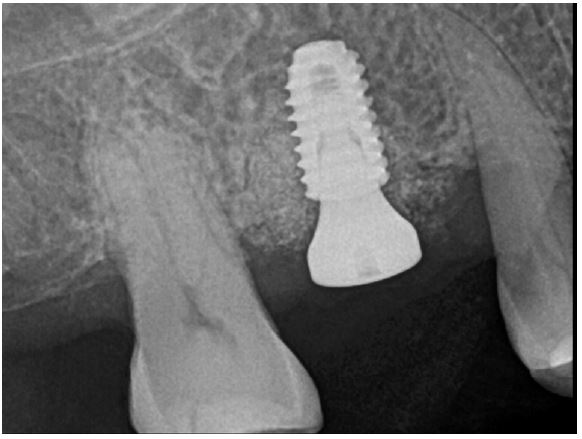
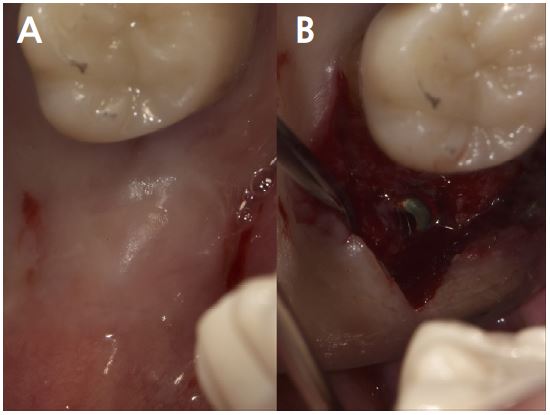
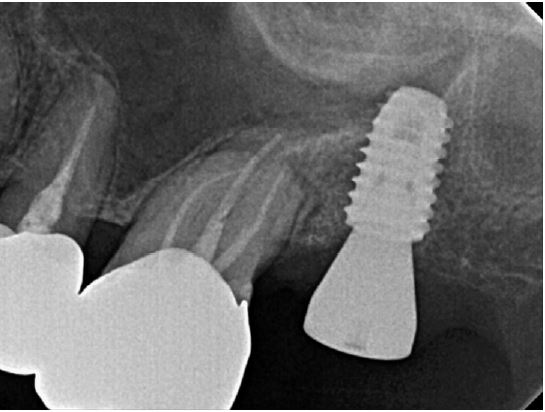
Clinical examination revealed grade 3 mobility with the gingival recession of the distal root of the left mandibular first molar (#36). Radiographic examination confirmed apically involved alveolar bone loss around the mandibular left first molar, however, at a sufficient distance from the mandibular canal (Fig. 1). It was determined that initial stability could be achieved in the apical area, and extraction and iARP were planned. The patient was instructed to rinse with 0.12% chlorhexidine digluconate solution (hexamedine; Bukwang, Seoul, Korea) for 2 min for oral disinfection. The mandibular left first molar was extracted using luxators and extraction forceps under local anesthesia with 2% lidocaine containing 1:80,000 epinephrine (Huons Lidocaine; Huons, Seoul, Korea) (Fig. 2A, 2B). After debridement of granulation tissues and irrigation with sterile normal saline solution, immediate implant placement (TS III 5.0 × 8.5 mm; OSSTEM, Seoul, Korea) was performed (Fig. 2C). The implant was placed 1 mm apical to the lingual socket wall, and the buccal side showed the exposure of two threads of the fixture (Fig. 2D). The implant stability quotient (ISQ) value at 1st surgery was 63. A gap between the implant surface and extraction socket wall and exposed buccal implant thread was filled with deproteinized bovine bone mineral (DBBM) (Bio-Oss®; Geistlich Pharma AG, Wolhusen, Switzerland) and covered with a native bilayer collagen membrane (NBCM) (Bio-Gide®; Geistlich Pharma AG) in a double-layer fashion (Fig. 2E). Subsequently, the hidden X suture and horizontal mattress suture (6-0 Ethilon; Ethicon, Cincinnati, OH, USA) were placed over the NBCM without the intention of primary wound closure (Fig 2F, 2G). Fourteen days after surgery, the patient returned for suture removal and postoperative examination. Healing of the depressed soft tissue above the extraction socket was observed, and a delayed healing pattern of the soft tissue with exposure of the cover screw was observed even after 4 weeks (Fig. 2H, 2I).

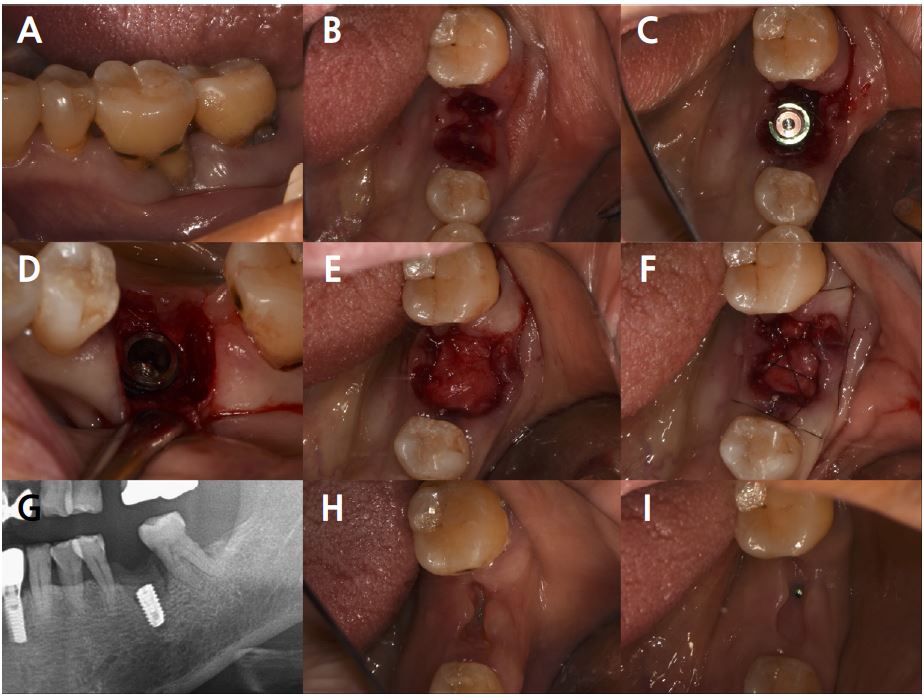
Fig. 2.
Case 1: Clinical photographs of the immediate implant placement with alveolar ridge preservation. (A) Gingival recession of the distal root of the left mandibular first molar, (B) Buccal gingival depression observed after tooth extraction, (C) Immediate implant placement in the left mandibular first molar, (D) Two threads of the fixture are exposed on the buccal side, (E) Deproteinized bovine bone mineral was placed in the extraction socket and covered with a native bilayer collagen membrane, (F) Hidden X and horizontal mattress sutures are placed, (G) Panoramic radiograph obtained after implant placement, (H) Depressed gingival healing was observed at stitch out (2 weeks), (I) Cover screw exposure with depressed gingival healing was observed during a recall check (4 weeks).
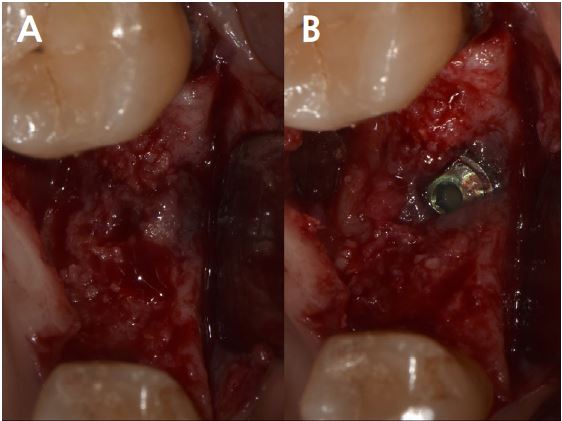
At uncovering, the second surgery, and 6 months after iARP, the site demonstrated no dehiscence of the implant fixture surface, however, a small amount of granulation tissue and graft material particles that were not compatible with the adjacent bone were observed above the cover screw (Fig. 3A). Debridement of granulation tissue and residual graft material particles with surgical curette for exposed cover screws (Fig. 3B). The ISQ value at the second surgery was 78. Subsequently, a 6.0 mm diameter, 6 mm length healing abutment was placed (Fig. 4).
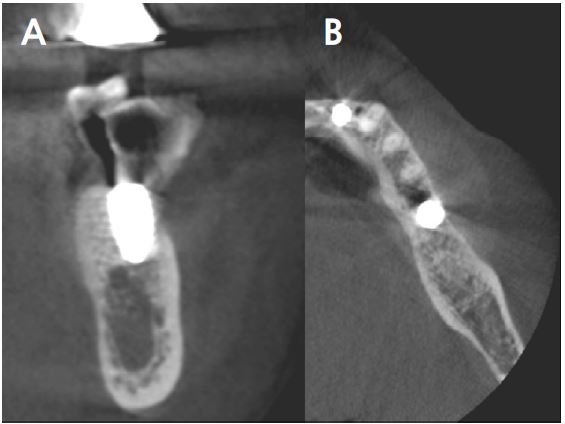
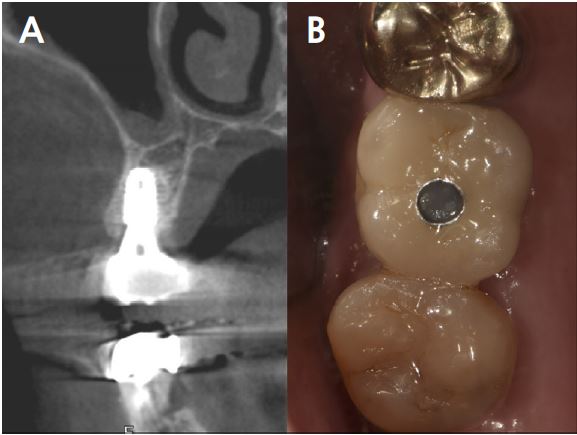
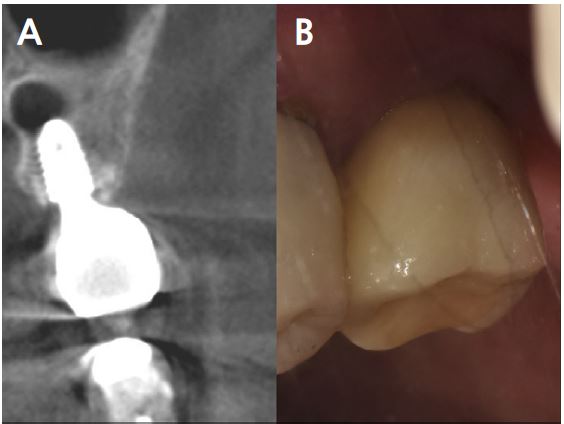
At 20 months follow-up, the cone beam computed tomography (CBCT) paraxial view showed that the buccal side of the fixture was adjacent to the outer border of the buccal bone plate (Fig. 5). However, the implant buccal probing depth (PD) did not exceed 4 mm, and the condition was maintained without any complications for 20 months after prosthesis placement (Fig. 6A, 6B).
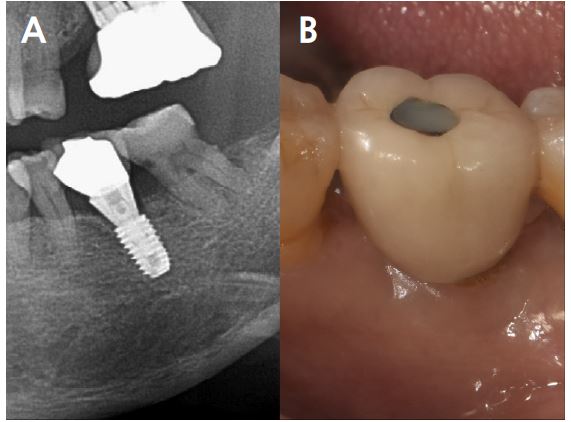
2. Case 2
A 71-year-old healthy female patient presented to the Department of Periodontology at Dankook University Dental Hospital with dull pain in the upper right molar.
Clinical examination revealed bleeding on probing with a 7 mm PD of the buccal furcation of the maxillary right first molar (#16). Radiographic examination confirmed apically involved alveolar bone loss in the buccal roots of the mandibular first molars. (Fig. 7). It was assumed that initial stability could be achieved in the apical and septal bones, and extraction and iARP were planned. The patient was instructed to rinse with 0.12% chlorhexidine digluconate solution for 2 minutes for oral disinfection. The tooth was extracted using luxators and extraction forceps under local anesthesia with 2% lidocaine containing 1:80,000 epinephrine (Fig. 8A, 8B). After debridement of granulation tissues and irrigation with a sterile normal saline solution, immediate implant placement at the septal bone (TS III 5.0 × 8.5 mm; OSSTEM) was performed (Fig. 8C). The ISQ value at 1st surgery was 60. The gap between the implant surface and the extraction socket wall was filled with DBBM and covered with NBCM in a double-layer fashion (Fig. 8D). Thereafter, the hidden X suture and horizontal mattress suture were placed over NBCM without primary wound closure (Fig. 8E, 8F). Fourteen days after surgery, the patient returned for suture removal and postoperative examination. A delayed healing pattern with yellowish granulation tissue above the extraction socket was observed, and a depressed healing pattern of soft tissue with exposure to the cover screw was observed even after four weeks (Fig. 8G, 8H).
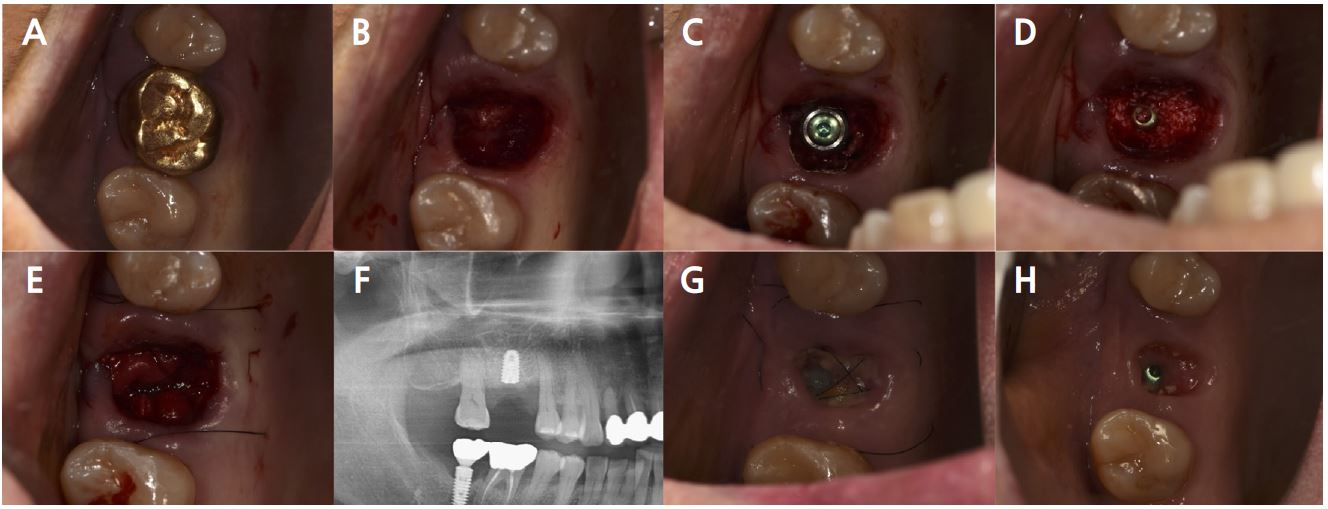
Fig. 8.
Case 2: Clinical photographs of the immediate implant placement with alveolar ridge preservation. (A) Initial clinical photograph of the maxillary right first molar, (B) Buccal gingival tears observed after tooth extraction, (C) Immediate implant placement in the septal bone, (D) Deproteinized bovine bone mineral was placed in the extraction socket, (E) Hidden X and horizontal mattress sutures are placed over the native bilayer collagen membrane, (F) Panoramic radiograph after implant placement, (G) Delayed gingival healing with yellowish granulation tissue observed at stitch out (2 weeks), (H) Cover screw exposure with depressed gingival healing was observed during a recall check (4 weeks).
Five months after the first surgery of the implant, reopening for the second surgery, the site demonstrated that the fixture was surrounded by new bone, and hard bone quality was confirmed through a surgical curette. (Fig. 9A, 9B). The ISQ value at 2nd surgery was 73. Subsequently, a 6.0 mm diameter, 5 mm length healing abutment was placed (Fig. 10).
Follow-up CBCT view obtained after 2 years revealed that the bone and implant conditions were maintained without any complications for 19 months after prosthesis placement (Fig. 11A, 11B).
3. Case 3
A 39-year-old healthy male patient presented to the Department of Periodontology at Dankook University Dental Hospital with pain and a foul odor in the upper left tooth.
Radiographic examination confirmed root caries and apical lesions in the maxillary left second molar (Fig. 12). It was predicted that the initial stability could be achieved, and extraction and iARP were planned. The patient was instructed to rinse with 0.12% chlorhexidine digluconate solution for 2 minutes for oral disinfection. The left second molar was extracted using luxators and extraction forceps under local anesthesia with 2% lidocaine containing 1:80,000 epinephrine (Fig. 13A, 13B). After debridement of granulation tissues in the apical area and irrigation with a sterile normal saline solution, immediate implant placement (TS III 5.0 × 8.5 mm; OSSTEM) was performed (Fig. 13C). The ISQ value at first surgery was 60. The gap between the implant surface and the extraction socket wall was filled with DBBM and covered with NBCM in a double-layer fashion (Fig. 13D, 13E). The hidden X suture and horizontal mattress suture were placed over NBCM without primary wound closure (Fig. 13F, 13G). Fourteen days after surgery, the patient returned for suture removal and postoperative examination. Healing of the depressed soft tissue above the extraction socket is observed. After four weeks, soft tissue depression continued, but epithelial healing was complete (Fig. 13H, 13I).
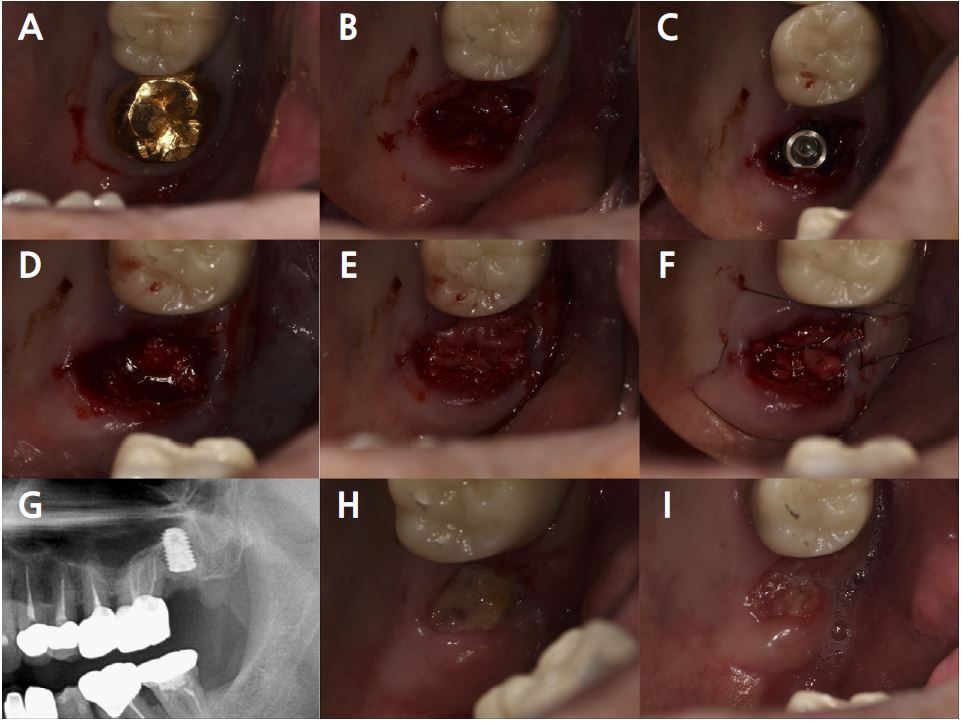
Fig. 13.
Case 3: Clinical photographs of the immediate implant placement with alveolar ridge preservation. (A) Initial clinical photograph of the left maxillary second molar, (B) The tooth was extracted without any gingival damage, (C) Immediate implant placement in the left maxillary second molar, (D) Deproteinized bovine bone mineral is placed in the extraction socket and covered with a native bilayer collagen membrane, (E) Extraction socket and covering with native bilayer collagen membranes, (F) Hidden X and horizontal mattress sutures are placed, (G) Panoramic radiograph obtained after implant placement, (H) Yellowish, depressed gingival healing observed at the stitch removal (2 weeks), (I) Depressed gingival healing was observed without inflammation at recall check (4 weeks).
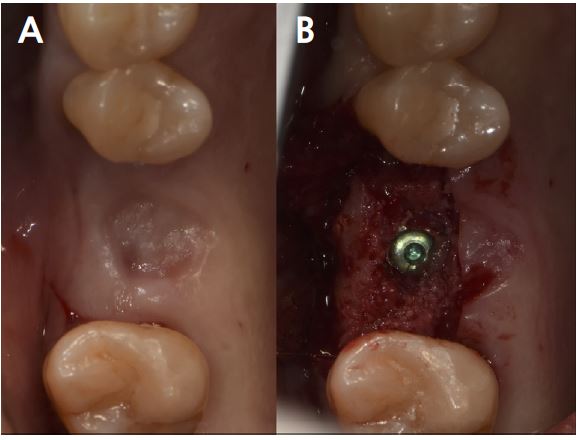
Four months after the first surgery for the implant, reopening for the second surgery, the site demonstrated that the fixture was surrounded by new bone, and the ISQ value was 68 (Fig. 14A, 14B). Subsequently, a 6.0 mm diameter, 7 mm length healing abutment was placed (Fig. 15).
A 2-year follow-up CBCT view revealed that the condition was maintained without any complications for 21 months after prosthesis placement (Fig. 16A, 16B).
Ⅲ. Discussion
Similar to this report, there is a randomized controlled trial in which semi-submerged healing was performed by placing a healing abutment immediately after placement in the anterior region and gap filling of the extraction socket.13 However, the molar region has a wider socket than the anterior region, so erratic healing may occur more frequently. Erratic healing was defined as fibrous scar tissue occupying the extraction site rather than the bone after more than 12 weeks of healing. Such healing was observed in patients younger than 60 years of age, with hypertension, molar extraction sites, or single tooth extractions.14 Although erratic healing may interfere with delayed implants, even with immediate implant placement, it can affect primary stability and weaken secondary stability. Therefore, gap filling is essential for immediate implant placement in the molar region.
Although there are no guidelines for the most effective bone graft material for ARP, DBBM is the most commonly used, and it is known that the material has a low absorption rate and osteoconductive properties.15 In addition, in a preclinical study by Kuchler et al., DBBM was not absorbed even under inflammatory conditions and contributed to new bone formation. Therefore, the DBBM introduced in this study was used for iARP without primary closure.16
Representative negative opinions about ARP with delayed implants include lack of primary stability due to weak bone quality and consequent increase in total treatment time due to the healing period. However, achieving primary stability in immediate implants is considered an important factor that contributes to implant survival. Accordingly, primary stability was secured in all cases in this report, and it was assumed that problems that may occur when placing delayed implants at the ARP site can be overcome. In addition, since open healing ARP was performed, it is assumed that the difficulty of predicting changes in soft and hard tissues can be overcome to some extent.
However, a clinical photograph of case 1 at the second surgery revealed a very thin residual bone in the area that previously showed a severe bone loss. In a follow-up CBCT view approximately 2 years later, it was confirmed that the position of the implant shoulder was similar to that of the outer buccal cortical bone. The thin peri-implant bone can act unfavorably in terms of long-term stability. This is presumed to be the result of bone modeling and remodeling in the area of severe buccal bone loss. Therefore, in the case of a severe bony wall defect, dehiscence should be reduced by adjusting the distance between the fixture and the defect. In addition, because the position of the fixture on CBCT appears to be shifted to the buccal side, and there is a lot of resorption of the buccal bone composed of bundle bone, it is necessary to consider positioning the fixture lingually or palatally during immediate implant placement.
The buccal bone in case 2 was also almost missing, however, the septal bone remained, there was no recession in the buccal soft tissue, and the distance from the buccal defect was relatively far compared to case 1, suggesting that the fixture was stably positioned into the bone housing. It is difficult to find a study on the distance between the defect and the fixture when the immediate implant is performed in the molar. Levine et al. confirmed that applying the graft material to a gap of 2 mm or more formed a thicker buccal bone wall in the case of immediate implant placement in the maxillary anterior region.17 Therefore, if there is a buccal defect wall in the molar area that can show various modeling and remodeling aspects after tooth extraction, it is necessary to maintain a distance of at least 2 mm from the fixture.
In all cases, an additional mattress suture was performed above the hidden X suture. According to our experience, when open healing ARP was performed in the extraction socket of a wide molar tooth, it was confirmed that graft material dropout occurred more frequently than in other areas. Accordingly, if the extraction socket is wide, if the soft tissue of the extraction socket shows undesirable irritation, or if it is assumed that the graft materials with socket sealing materials seem to be loose with only the hidden X suture, additional mattress sutures can be performed. This may reduce the buccolingual width of the keratinized gingiva to some extent, however, it is thought to have a more reliable fixing force to maintain the graft material inside the extraction socket.
