

Ⅰ. Introduction
Following tooth extraction, the periodontal tissue surrounding the extraction socket undergoes structural changes, including dimensional and radiographic changes. Alveolar bone resorption and remodeling occur within the alveolar process, and the buccal bone plate with a high ratio of bundle bone shows significant bone loss compared to the lingual bone.1,2 In most cases, the degree of horizontal reduction of the alveolar bone is greater than that of vertical reduction.3 When a prosthetic restoration, such as an implant, is placed if the soft tissues are damaged after tooth extraction, there are significant functional and esthetic limitations. Various procedures have been attempted to minimize alveolar bone resorption and preserve the volume of periodontal tissue.
The most widely known ridge preservation technique for extraction sockets is the insertion of bone graft materials using membranes. However, previous studies did not reveal any bone graft materials or barrier membranes that have distinct advantages over other graft materials.4,5 Generally, xenograft or allograft materials are preferred because of their low absorption and replacement rates, relatively long maintenance period, and convenience of not causing secondary wounds.6,7 Previously, Cardaropoli et al. reported in a series of studies that alveolar bone loss could occur without the use of ridge preservation techniques to compensate for alveolar bone resorption after tooth extraction regardless of the thickness of the buccal plate.7,8,9 Numerous studies have shown that ridge preservation treatment is effective in maintaining a stable alveolar volume to optimize functional and esthetic results after tooth extraction.4,10 In particular, the reduction of bone volume atrophy by preserving the ridge is remarkable in premolars with low esthetic importance and anatomical advantages.10,11
Three-dimensional (3D) digital impression using an intraoral scanner is attracting attention as a novel method that can address various disadvantages, such as the inconvenience and possibility of errors in taking impressions and making models using existing impression materials. Because the shape and volume of the soft tissue can change even with a slight pressure, in case of conventional model making using an impression material, various errors inevitably occur when measuring the thickness or volume of soft tissue. Therefore, in this study, the 3D images obtained through the intraoral scans of patients were superimposed to examine the contour changes according to the extraction healing process, and were compared with the results of previous similar studies in which plaster models were scanned and overlapped.11,12,13 Although only soft tissue contours can be scanned, it has been found through several studies that the thickness of soft tissue can be accurately measured by matching the results of intraoral digital impressions with the cone beam computed tomography (CBCT) images of the alveolar bone.14,15 However, use of CBCT may induce unnecessary radiation in patients undergoing tooth extraction prior to orthodontic treatment. Thus, CBCT was not performed, and only the change in the ridge contour was followed and analyzed. The changes in the outline of soft tissue over time could be important reference materials for esthetic improvement of treatment results.
The purpose of this study was to noninvasively measure the overall contour changes of the extraction socket with data obtained using an intraoral scanner, and to investigate the effect of ridge preservation on the linear changes.
Ⅱ. Materials and Methods
Of the patients who visited the Department of Orthodontics, Seoul National University Gwanak Dental Hospital between September 2019 and August 2020, those who needed extraction of both mandibular premolars before orthodontic treatment were recruited. Only those 18 years of age or older who had to extract the left and right mandibular premolars one by one and had healthy adjacent teeth on both teeth were recruited. The following exclusion criteria were applied:
1) Pregnancy, diabetes, mental illness
2) Smokers who smoked more than 10 cigarettes a day
3) Those who were taking immunosuppressants and other drugs that induce gingival growth
4) Those who may have an allergic reaction to the xenogenic bone graft material or the collagen membrane used in the experiment
5) If the tooth adjacent to the premolar to be extracted has already been lost or needs to be extracted together
6) In cases the teeth adjacent to the premolar to be extracted showed mobility or the depth of the periodontal pocket exceeded 4 mm
This study was designed as a randomized controlled clinical study according to the Helsinki Declaration, with approval from the Institutional Review Board (IRB No. CRI19010) of Seoul National University Dental Hospital.
Following the screening visit, the patients were scheduled for tooth extraction. Immediately before extraction of the mandibular premolars, an intraoral scan (i500; Medit, Seoul, Korea) was performed for the area, including at least two teeth mesial and distal to the tooth to be extracted. According to a randomly selected computer-generated list, one of the left and right mandibular premolars was assigned to the experimental group and the other to the control group.
In the experimental group, the inner surface of the extraction socket was thoroughly currettaged, and a fixed amount (100 mg) of deproteinized bovine bone mineral (Bio-Oss ® Collagen; Geistlich Pharma AG, Wolhusen, Switzerland) and an absorbable collagen membrane (Bio-Gide ® ; Geistlich Pharma AG) were applied without incision. After removing the granulation tissue, the control group was sutured in the same manner as the experimental group and the sutures were removed 2 weeks later. On the 30th
and 90th day after tooth extraction, the sockets were rescanned, and the STL files were saved and transmitted to a software program (Geomagic Verify 16; 3D Systems, Rock Hill, USA). Orthodontic treatment for tooth movement was not performed for 90 days after tooth extraction.
To measure the serial changes in the gingival width, all 3D scan images were merged for the automated best-fit alignment option using neighboring teeth as reference structures. Then, a buccolingual section was selected that divided the extraction socket region into two equal parts using another software (Rapidform 2006; INUS Technology, Seoul, Korea). At the baseline, a reference line was drawn through the buccal and lingual gingival margins. Horizontal ridge width (HW) was measured 2- and 4 mm (H2 and H4) below the reference line in all three STLs according to previous studies,13 and the change in HW over time was also measured. Vertical change was measured at the center of the ridge perpendicular to the reference line. After superimposing the three scan results, horizontal change on the buccal and lingual sides was measured as the height, and the vertical change at the center of the extraction site was also measured. Surgeries and intraoral scanning were performed by one clinician (YJK). Data superimposition based on the adjacent teeth, the cross-sectional setting, and the linear measurements were performed by another expert (JHK). All quantitative measurements were averaged after two iterations.
The data were analyzed using Excel (Microsoft Corp., Redmond, USA). The mean values, standard deviations, and differences of means were calculated. Repeated measures analysis of variance (rmANOVA) was applied to evaluate the effects of ridge preservation and time on each outcome. Differences between 30 and 90 days, buccal and lingual differences, and changes in H2 and H4 within the same group were compared using the Wilcoxon signed rank test. Statistical significance was set at p < .05 (SPSS statistics 23, IBM, Armonk, USA).
Ⅲ. Results
In nine patients, 18 teeth were extracted from both premolars, ridge preservation was performed only on one side, and a horizontal change in width was observed. Table 1 shows the horizontal and vertical linear changes measured by superimposing the soft tissue contours obtained using intraoral scanning just before tooth extraction and 30- and 90 days after tooth extraction. Buccal and lingual changes according to the reference height and vertical height change were expressed as average values over time. All quantitative measurements were recorded after two iterations, and the average amount of tissue changes surrounding the premolars was calculated.
Table 1.
The mean (±SD) soft tissue contour changes between pretreatment and 30- and 90 days after extraction
ESM; Extraction socket managed group (experimental group)
| BUCCAL CHANGE (mm) | LINGUAL CHANGE (mm) | VERTICAL CHANGE (mm) | |||||
| 30D | 90D | 30D | 90D | 30D | 90D | ||
| ESM | H2 | - 1.111 ± 0.473A | - 1.524 ± 0.929 | - 1.745 ± 1.805A | - 1.450 ± 1.226A | ||
| H4 | - 0.432 ± 0.495B | - 0.845 ± 0.425 † | - 0.101 ± 0.338B | - 0.307 ± 0.258B † | |||
| - 1.452 ± 0.742a | - 0.801 ± 0.626b | ||||||
| CONTROL | H2 | - 0.906 ± 0.582Ab | - 1.491 ± 0.523Aa ‡ | - 0.705 ± 0.549Ab | - 0.987 ± 0.203Aa ‡ | ||
| H4 | - 0.177 ± 0.343Bb | - 0.733 ± 0.684Ba | - 0.024 ± 0.107Bb | - 0.207 ± 0.165Ba | |||
| - 1.263 ± 0.387a | - 0.463 ± 0.268b | ||||||
As shown in Fig. 1, the three soft tissue contours were observed in one cross section, and the distance between the outlines was measured. Horizontal lines were drawn 2- and 4 mm below the reference line
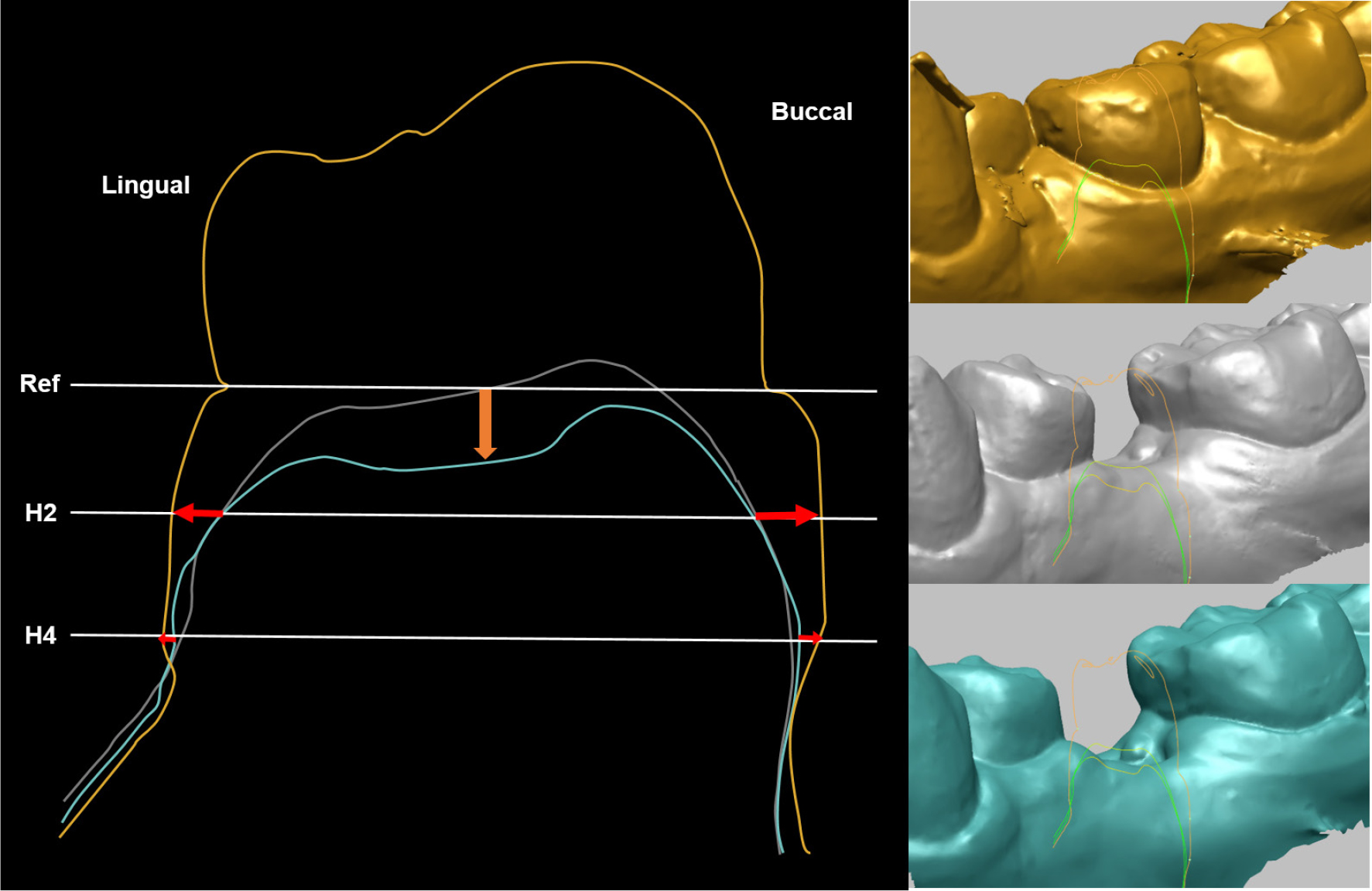
Fig. 1.
Cross-sectional view of the region of interest.
The contour of the yellow model (before tooth extraction), white model (30 days after tooth extraction), and blue model (90 days after tooth extraction) were superimposed according to the adjacent teeth. The reference line was drawn through the buccal and lingual gingival margins. Horizontal width change (red) was measured between the STLs at 2- and 4 mm (H2 and H4) below the reference line. Vertical change in the ridge was measured perpendicular to the reference line (orange) at the center of the ridge.
(H2 and H4) connecting the gingival margin before extraction, and the amount of change on the buccal and lingual sides was measured. When comparing the decrease in gingival width at 30- and 90 days after tooth extraction, there was a significant difference in all cases regardless of the buccal, lingual, and vertical height in the control group, but not in the experimental group. (p < .05)
In addition, on both the buccal and lingual sides, the horizontal width reduction was greater at H2 than that at H4. (p < .05, Except for 90-day buccal measurements in the experimental group) (Fig. 2). On comparing the difference in mean horizontal width reduction between the buccal and lingual sides, only at 90 days after tooth extraction, the buccal reduction was significantly greater than the lingual reduction in the experimental group at H4 and the control group at H2. (p = .011, .008).
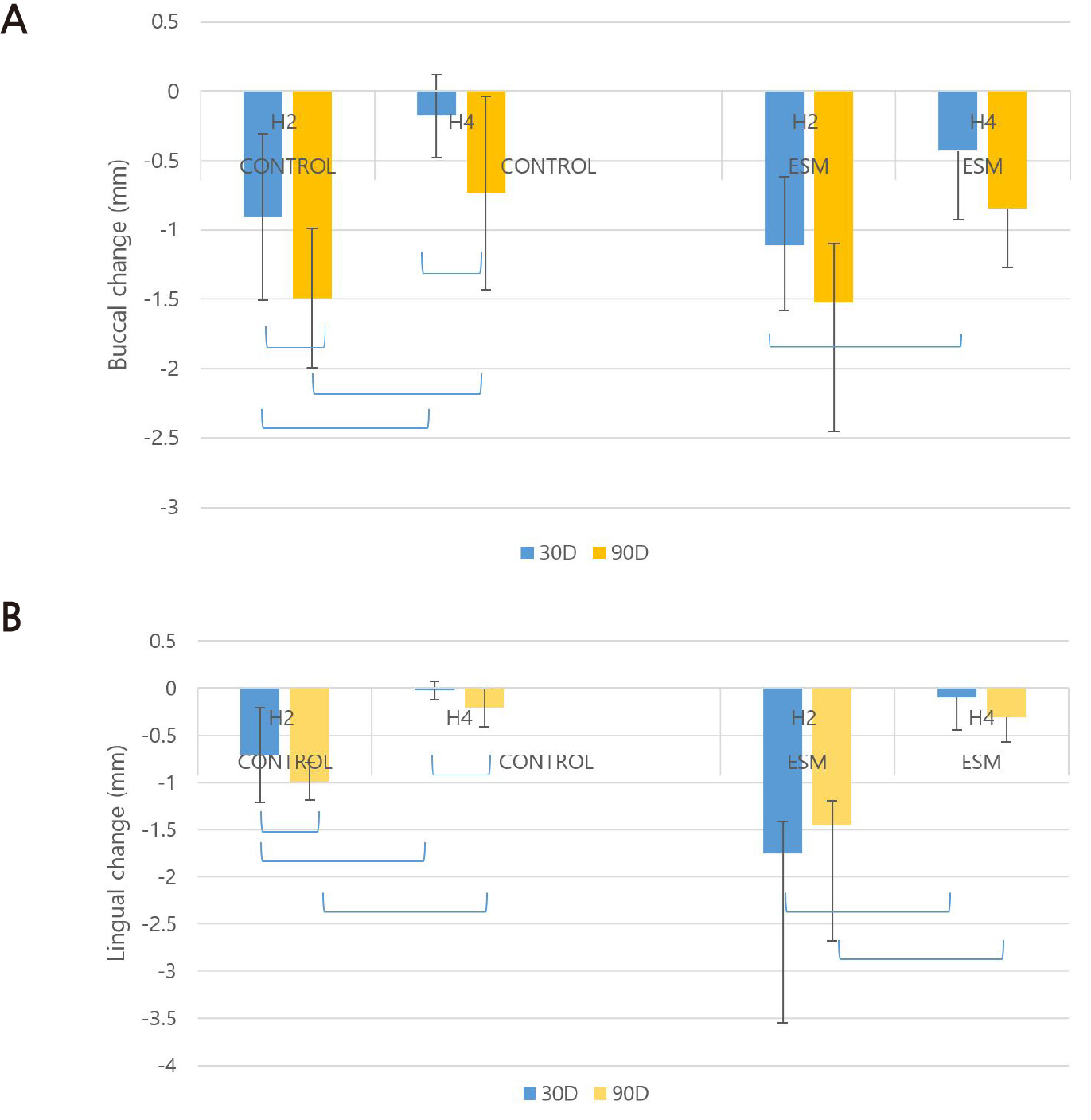
Fig. 2.
The mean change in horizontal ridge width on the buccal (A) and lingual (B) sides
H2: horizontal width 2 mm inferior to the reference line , H4: horizontal width 4 mm inferior to the reference line, ESM; extraction socket managed group ( experimental group); the blue connecting line indicates a statistically significant difference. (p < .05)
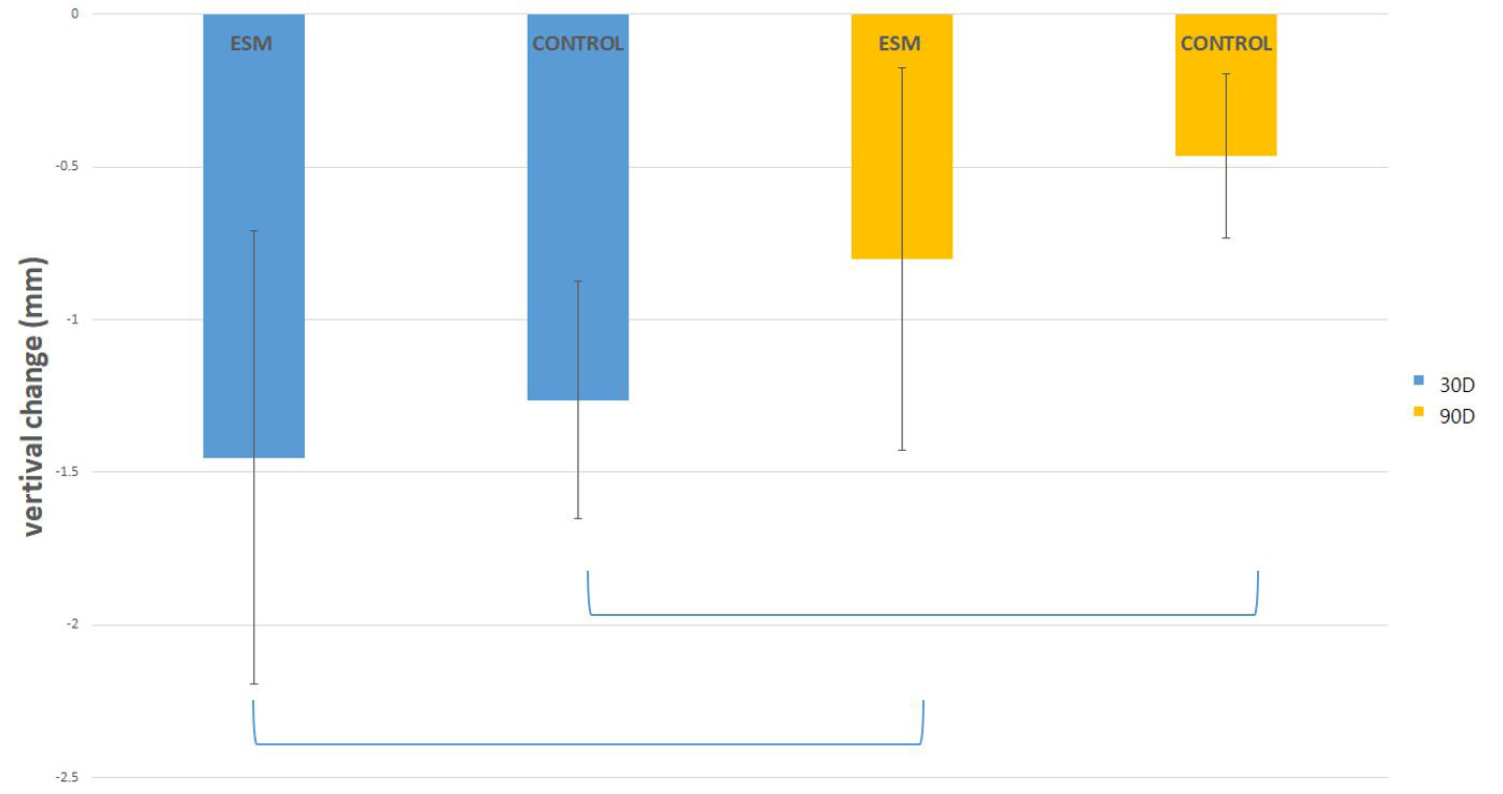
Fig. 3 shows the vertical changes in the center of the ridge, and both the experimental group and the control group showed a significant decrease in the gingival height at 30 days after tooth extraction, which increased again after 90 days. (p < .05).
As mentioned above, the difference in the amount of change according to the time point and location was significant in the control group, but overall, the difference in the horizontal width of the experimental group and the control group measured repeatedly over time was not statistically significant as a result of rm-ANOVA. (p = .44)
Ⅳ. Discussion
Several recent studies have concluded that direct digital impression systems can be as accurate as 3D models obtained by conventional impression methods.16,17 In this clinical study, all data were obtained through direct intraoral scanning rather than a method of recording impressions and preparing models to differentiate it from the existing studies. Because the intraoral scanner can directly view the region of interest in three dimensions in advance, the area can be quickly rescanned in case of a discrepancy, which makes the procedure more convenient than the conventional impression method that requires repeating the entire process. To analyze this digital impression data, it is also important to perform operator calibration for scan acquisition or calibration for superimposition and measurement. Therefore, in this study, all digital impressions and software work were performed by a single person.
Since this study was a pilot study involving a small amount of data, one should be cautious in drawing a clear conclusion, but as a result of observing the change in the soft tissue contour over time in each of the nine experimental and control groups, there was no statistically significant difference overall.
This is somewhat different from the conclusions of numerous studies suggesting the need for ridge preservation with bone grafting in the extraction socket. Since this study involved extraction of teeth without periodontal disease for orthodontic treatment in healthy patients, it can be inferred that extraction socket management did not cause a significant difference in the relatively healthy teeth. In the experimental group, in which the xenograft material was placed into the extraction socket, an average decrease in horizontal width of 0.845 mm on the buccal side and 0.307 mm on the lingual side at H4 was observed in 90 days. In the control group, the mean reduction in horizontal width was 0.73 mm buccally and 0.21 mm lingually. The vertical decrease in gingival height measured 90 days after tooth extraction was 0.8 mm in the experimental group and 0.46 mm in the control group.
This is a rather smaller reduction compared to that observed in previous studies, where on average, the width of the alveolar ridge decreased by 3.8 mm horizontally and 1.24 mm vertically within 6 months after tooth extraction.10 According to a recent review, ridge preservation techniques are known to prevent alveolar bone resorption of up to 1.99 mm horizontally and 1.16–1.72 mm vertically. 5 Of course, since this study only measured linear changes of the outline of the soft tissue, it is difficult to ascertain the exact decrease in the width of the alveolar bone. Rather than simply comparing numerically, it is reasonable to compare the ratio of the amount of change to the overall width, as done in a previous study. As a result of calculating the ratio of the amount of change to the total width and length, it was found that the reduction was less than that reported in a previous study.13 It can be speculated that this is because, unlike previous studies that performed bone regeneration and prosthetic restoration, such as implants after tooth extraction, the present study was conducted in healthy young patients without periodontal disease. However, since healing continues even after 90 days and further changes may be noticeable after 6 months, the effect of ridge preservation may not be revealed at 90 days. Above all, the fact that the experimental group did not show a significant difference compared to the control group, which showed a sharp decrease in ridge width at 90 days compared to 30 days after tooth extraction, suggests the possibility that the ridge preservation effect may appear more clearly after 90 days.
Several reports have shown that ridge preservation before orthodontic tooth movement increases the tooth movement speed, reduces the possibility of gingival recession or dehiscence, and also affects the reduction in root resorption.18,19,20 A split-mouth design was planned for premolars, which are known to be the most appropriate indications for ridge preservation,10,11 and the contours of the extraction socket and surrounding soft tissues were observed over time for orthodontic patients who needed extraction of such premolars. Orthodontic force was not applied to prevent the movement of adjacent teeth as much as possible for 90 days after tooth extraction, and orthodontic movement was started after 90 days. However, since the teeth adjacent to the extraction socket moved slightly even without the application of orthodontic force, four teeth mesial and distal to the extracted socket were included as reference points when taking impressions and superimpositions, which may have limited the accuracy of the measurement.
The decrease at H2 showed a remarkable change, especially in the experimental group. This reflects the irregular dent in the center of the socket immediately after extraction; in some cases, the vertical height decreases rapidly. Therefore, in subsequent studies, it should be considered that measurements at 2 mm below the reference line cannot be considered to reflect true horizontal width change. In case of vertical change, it was observed that the height increased again after 90 days than that immediately after extraction, which can be inferred from the healing of the extraction socket and remodeling of the alveolar bone.
A major limitation of this study is the small sample size, which prevents proper power calculations from being performed. In addition, we have to admit that there is a limit to mentioning the exact thickness of soft tissue because CBCT imaging was not performed separately to measure the width of the inner alveolar bone. Further research should be conducted using different measurement methods so that not only linear measurements but also 3D volumetric variations can be measured.
Ⅴ. Conclusion
Within the limits of this study, the horizontal width of the alveolar ridge during the healing process of healthy mandibular premolar extraction showed a tendency to decrease over time, and a greater change was observed as the height of the measurement point was closer to the reference gingival margin. The effects of ridge preservation were not evident.
