

Ⅰ. Introduction
Ⅱ. Case Series
Ⅲ. Lateral MSA
Ⅳ. Flap Surgeries Exposing Previous Bony Window
Ⅴ. Discussion
Ⅵ. Conclusion
Ⅰ. Introduction
Sinus pneumatization reduces bone height for proper implant placement.1 To overcome this, maxillary sinus augmentation (MSA) was introduced. It has proven to be a predictable treatment.2, 3 It is divided into lateral and trans-crestal approaches depending on the available bone height.
Lateral MSA is recommended when the available bone height is < 4–5 mm.4 Factors were investigated for the survival of implants placed in the augmented sinus using lateral MSA. Among them, using a barrier membrane over the bony access window significantly affected survival.3, 5 The suspected reasons may be as follows: 1) soft tissue ingrowth/ penetration into the bone-augmented area, 2) bone graft material displacement out of the augmented area via the access window, and 3) resultant disturbance of new bone formation.
However, in animal studies, the bony access window was not often covered with a barrier membrane.6, 7 Histologically, various extents of bone formation have been observed between the margins of the window without hampering the study of the effect of test treatment. In a rabbit model, the effect of the barrier membrane was preclinically tested further to verify the necessity of the membrane.8 Within 4 weeks, healing of the window area was incomplete, irrespective of the use of the membrane over the window. However, the effect of the membrane was insignificant in terms of new bone formation in the augmented area. Therefore, we hypothesize that a barrier membrane over the bony window may be redundant in specific situations.
Clinically, long-term data regarding the healing of the bony access window remains limited, particularly when a barrier membrane is not used. The aim of the present case series was to present clinical and radiographic healing of the bony access window without barrier membrane coverage at least 5 years post-lateral MSA.
Ⅱ. Case Series
In 16 patients who had undergone lateral MSA, flap surgery was planned in the area where the bony window (from the previous lateral MSA) was neighbored. No barrier membrane was applied to cover the windows for previous MSA. The period between the MSA and the flap surgery ranged from 5 to 27 years (mean: 14.1 ± 7.0 years). Table 1 shows the demographic information of these patients.
Table 1.
Patients’ demographic information and results of surgical re-entry to the previous bony window site
Ⅲ. Lateral MSA
A full-thickness flap was reflected to expose the lateral bony wall of the maxillary sinus. A bony access window was made with a round carbide or diamond-coated bur. The width and height of the window were approximately 20 and 8 mm, respectively. Subsequently, the sinus membrane was elevated from the sinus bone walls. A bony lid remained on the sinus membrane (Fig. 1A). Subsequently, bone substitute materials (allogenic, xenogeneic, or synthetic) were used for grafting. In all cases, implants were placed simultaneously with MSA. No barrier membrane was applied over the bone window (Fig. 1B). When elevating the sinus membrane, a small perforation (2–3 mm) was detected in four patients, but the perforation was not intentionally repaired. All implants were submerged. After 6–9 months of healing, the surgical sites were uncovered, and healing abutments were connected. Final prostheses were inserted after mucosal healing (approximately 2 months).
Ⅳ. Flap Surgeries Exposing Previous Bony Window
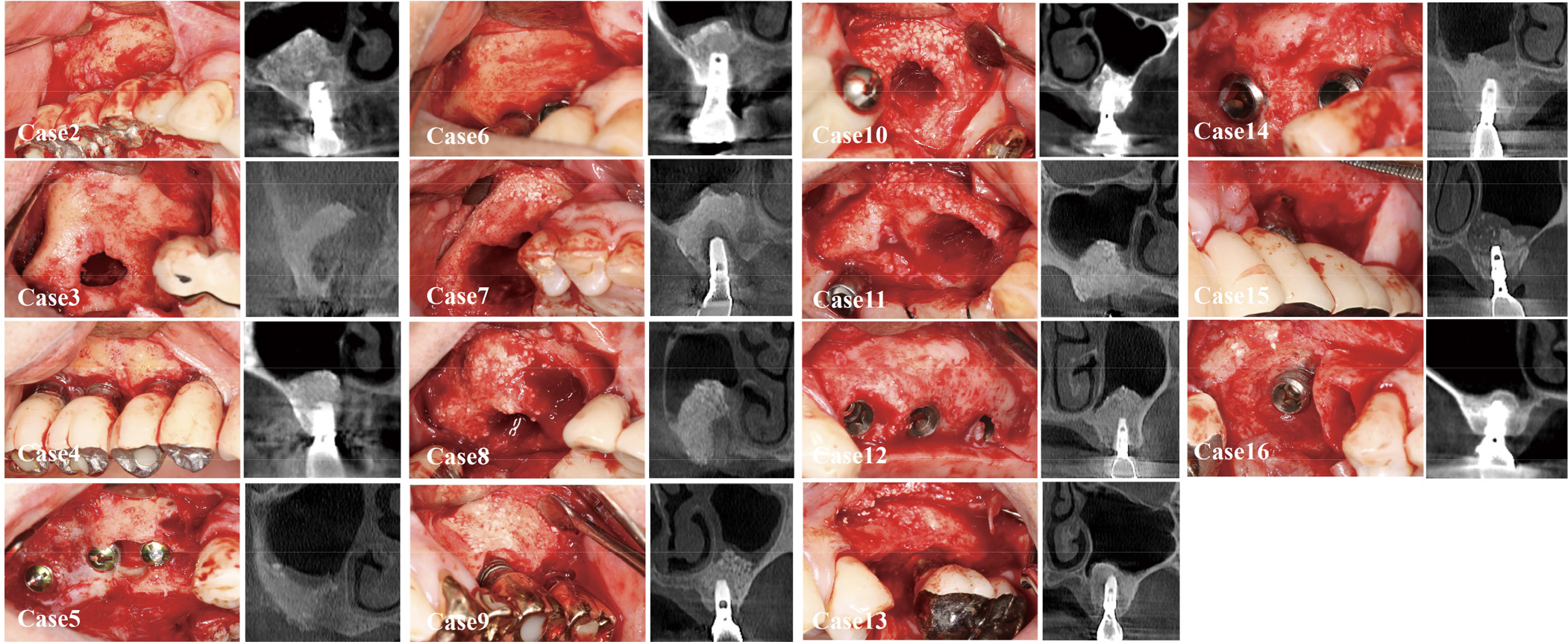
For various reasons (peri-implantitis: 11; loss of osseointegration: one; fixture fracture: one; screw fracture: one; additional implant placement in the adjacent area: one; delayed visit for uncovering: one), flap surgeries were performed at the previous implant sites. Intraoperatively, the bony window areas could be observed clinically and radiographically (Figs. 1C, 1D, and 2). Clinically, no site showed unfavorable tissue characteristics in the previous bony window area, such as fibrotic tissue formation extending into the maxillary sinus. Corticalization within the borders of the window was sufficient in all cases, as judged by probing with a periodontal probe and on cone-beam computed tomography (CBCT). Hard feel was detected by probing, and corticalization was observed on CBCT. At eight of the 16 sites, the outlines of the window could not be discerned from the neighboring area. However, at the other eight sites, partial demarcation (indicating the previous window at the lateral MSA) was observed. The remnants of bone graft particles were observed at seven sites. The particles were attached to the inside of the flap; at other sites, the particles could be discerned but were well-integrated with the regenerated bone tissue. At five sites, the bone contour looked bulged compared to the pre-MSA situation. Osteoplasty was performed in three of these cases.
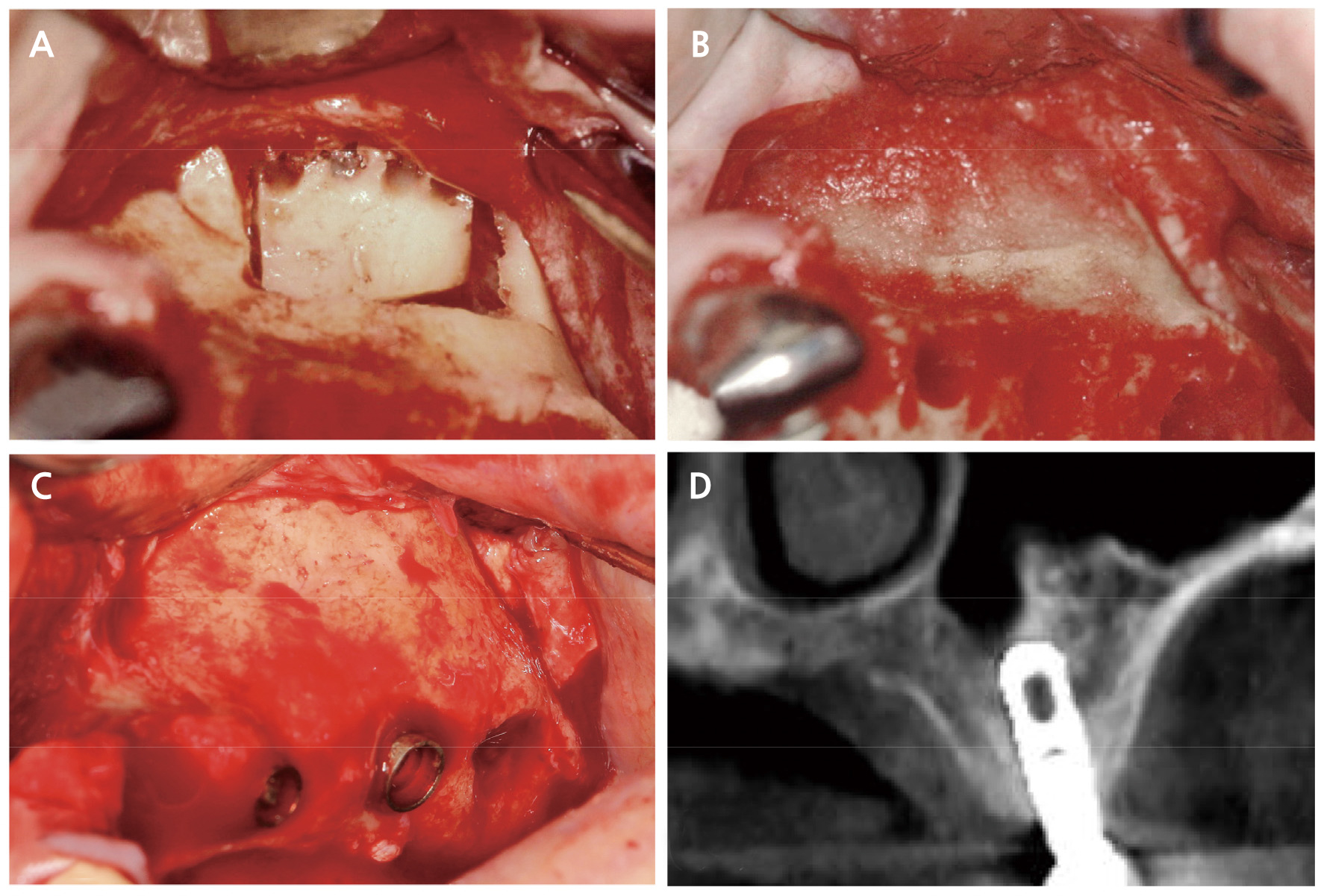
Fig. 1.
Representative case of the patient #1. (A) A bony access window was made on the lateral wall of the maxillary sinus, (B) Bone substitute material was grafted in the sinus, and no barrier membrane was applied over the window, (C) Clinical situation after 27 years, (D) Cone-beam computed tomographic view after 27 years.
Ⅴ. Discussion
The present case series detailed healing of the bony access window without barrier membrane coverage in lateral MSA. All sites exhibited favorable corticalization in the previous bony window areas, but at some sites, remnants of bone substitute particles and bulging of the bone contour were observed.
A barrier membrane is routinely applied over a bony access window in lateral MSA. The primary reason for using the barrier membrane in lateral MSA is similar to guided bone regeneration (GBR). The membrane establishes an occluded space from unwanted tissue or cell interaction. Thus, bone-forming cells can selectively act in the augmented space.9
However, healing of an augmented sinus may differ from that of the GBR site: 1) The sinus cavity is surrounded by more bone walls than the sites for GBR,10, 112) in MSA, bone substitute material is contained within the cavity, but in GBR, the stability of the bone material becomes susceptible to action (for example, suturing)12 and pressure from the outer environment. Thus, the requirement of a barrier membrane to cover the bony access window may be questionable in lateral MSA, as supported by several studies. Preclinical investigations demonstrated no significant influence of a barrier membrane on the amount of newly formed bone within the augmented sinus.8, 13 Previous clinical studies (published decades ago) have advocated using the membrane.14, 15, 16 However, recent studies have revealed no distinct difference in new bone formation or dimensional stability of augmentation between the membrane-applied and non-applied sinuses.17, 18
In the present study, no histologic analysis was performed. Although corticalization of the bony window area was confirmed visually and with probing, the tissue composition of new tissue in the window area was unknown. In a preclinical study, the absence of a membrane affected bone formation near the window area as the window size increased.8Remnants of graft particles in the present case series might reflect incompletely ossified parts. However, no clinical study showed detailed histologic information in the window area.
Five cases showed bulging bone contours, indicating graft material displacement out of the sinus cavity. Such a finding was in line with a clinical study demonstrating statistically significant displacement of bone graft material via the window when the window was not covered by the membrane.19 However, in that study, the bone graft displacement did not influence implant placement later.
Despite the results of the present case series, we do not completely reject using a barrier membrane over the bony window. Particularly in the case of a large or multiple bony access windows and thin crestal bone, the membrane should be used for covering the window to maximize healing potential and prevent bone graft material displacement.
The present case series has some limitations. First, the size of the bony access window was not standardized. Second, CBCT was not performed immediately after MSA, although postoperative CBCT is not a routine procedure in clinical settings. Third, only partial information about healing of bony access windows without barrier membrane coverage can be obtained because of the lack of histologic analyses. Fourth, implant survival and dimension stability of augmentation could not be compared because only selected cases were included in the present case series.
