

Ⅰ. Introduction
Ⅱ. Case Reports
1. Surgical procedure
2. Case 1. Preoperative mucous retention cyst
3. Case 2. Preoperative chronic maxillary sinusitis
4. Case 3. Postoperative maxillary sinusitis following sinus augmentation via transcrestal approach
5. Case 4. Postoperative maxillary sinusitis following SALW
Ⅲ. Discussion
1. Preoperative assessment and management of maxillary sinus disease
2. Intraoperative complications in sinus augmentation
3. Management of postoperative maxillary sinusitis
4. Prognosis of dental implant placed following surgical complications
Ⅳ. Conclusion
Ⅰ. Introduction
Placement of dental implants on the posterior maxilla can be challenging in case of severe atrophy of the alveolar ridge, pneumatization or pathologic conditions of the maxillary sinus. Since the sinus augmentation procedure was presented by Tatum H Jr. in 1976 and published by Boyne PJ et al. in 1980,1,2 previous studies regarding dental implants placed following sinus augmentation have shown predictable survival outcomes over 90% compared to implants placed on the native bone.3,4,5,6 Although graft failure rates of sinus augmentation are low (1–6.7%), the possibility of surgical complications should be considered to obtain a favorable clinical course.7,8,9 In addition, if the augmentation is not properly managed, surgical complications could result in paranasal sinus involvement or abscess in adjacent structures, including the brain and orbit, a serious adverse event in the postoperative period.10,11
Intraoperative complications of sinus augmentation, as reported in the literature, are Schneiderian membrane perforation and bleeding. Postoperative complications include wound dehiscence, acute/chronic maxillary sinusitis, mucocele formation, graft infection, and dissemination of the graft material into the maxillary sinus causing, disrupting the normal physiologic sinus function.8 Furthermore, risk factors of perioperative complications have been well documented in previous studies.3,12,13,14 Nonetheless, a consensus on the classification of pre-existing maxillary sinus diseases (MSDs) or guidelines for multidisciplinary therapy in a hospital setting before sinus augmentation is still lacking. In the present report of cases, the authors describe, along with a literature review, the management of perioperative pathologic conditions of the maxillary sinus and the clinical outcome of the sinus augmentation procedure.
Ⅱ. Case Reports
1. Surgical procedure
The sinus augmentation via lateral window (SALW) procedure was performed via conventional transoral antrostomy technique as described in previous studies.15,16,17 During SALW, a bony window was prepared using a piezoelectric device, and a bone graft was performed using a synthetic beta-TCP bone substitute (Sorbone; Meta Biomed Co., Cheongju-si, Korea). At 4–6 months after SALW, dental implants (Bright Implant; Dentium Implant Co., Seoul, Korea) were placed. Perioperative medications were prescribed according to signs of infection and inflammatory condition of maxillary sinus as follows: (1) antibiotics (amoxicillin 350 mg/clavulanate 25 mg; Samsung Pharmaceutical Co., Gyeonggi-do, Korea and/or metronidazole 500 mg (HK inno.N Corp, Cheongju-si, Korea); (2) anti-inflammatories (loxoprofen sodium 60 mg; Myungmoon Pharmaceutical Co., Seoul, Korea); (3) nasal decongestants (pseudoephedrine hydrochloride 60 mg; Samil Co., Seoul, Korea).
2. Case 1. Preoperative mucous retention cyst
A 48-year-old female (patient 1) was referred to the Department of Oral and Maxillofacial Surgery to evaluate maxillary sinus disease and dental implant placement on the left posterior maxilla. Radiographic examination revealed dome-shaped, cystic opacity and approximately 1–2 mm available bone height (Fig. 1A and 1B) in the left maxillary sinus. Two months after the extraction of the left maxillary first molar, treatment of mucous retention cyst, including incision of Schneiderian membrane, aspiration and removal of mucosal contents, was done (Fig. 1C to 1E), followed by SALW with bone substitute. Six months after SALW, dental implants were placed on the left maxillary molar area (Fig. 1F and 1G).
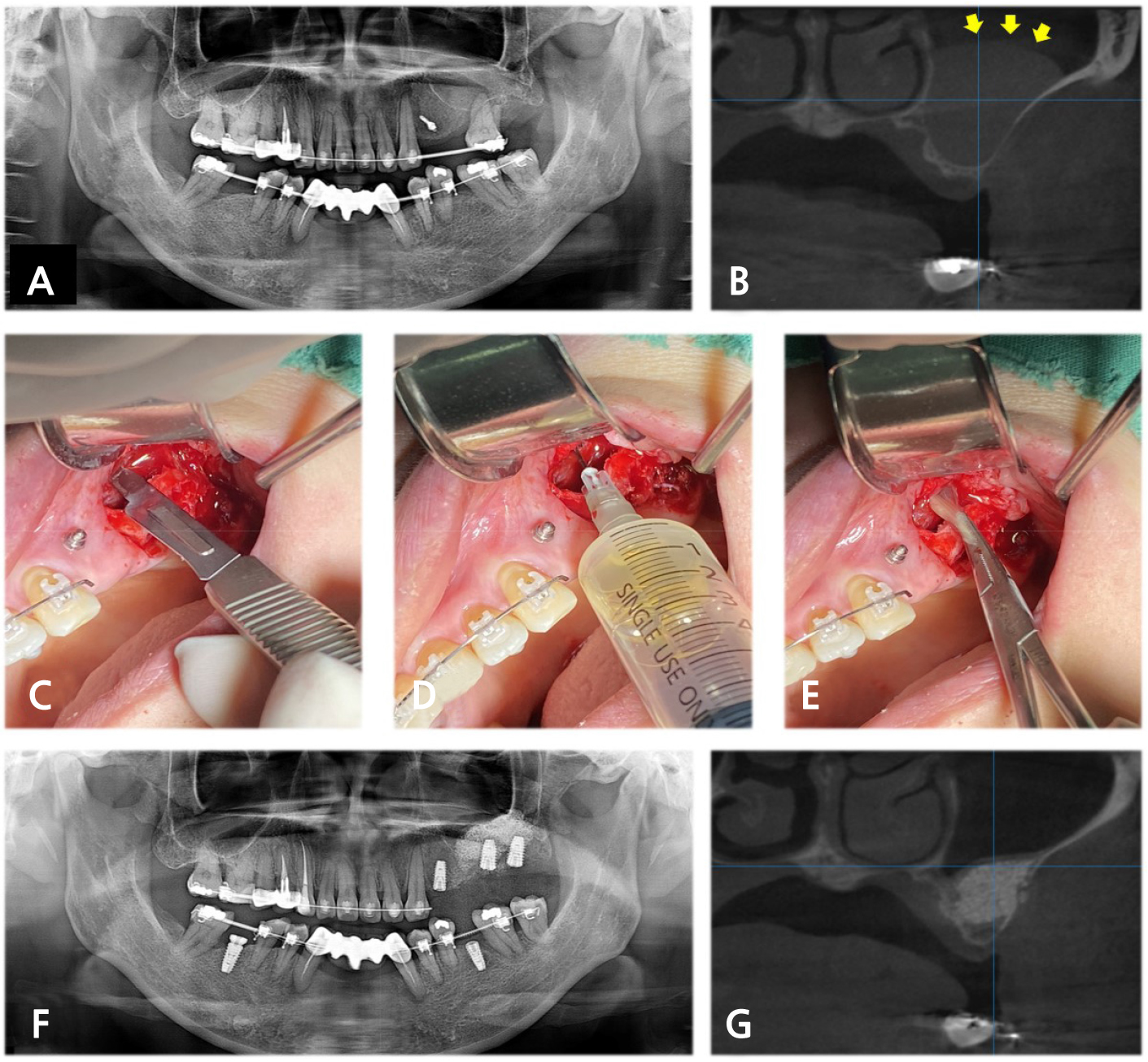
Fig. 1.
(A) Preoperative panoramic radiograph (PAN) and (B) Cone beam computed tomography (CBCT) of patient 1 revealed a dome-shaped opacity in the left maxillary sinus (yellow arrow), (C) Clinical photograph demonstrated incision of the membrane, (D) Aspiration and (E) Removal of mucosal fluid, (F) Postoperative PAN and (G) CBCT demonstrated no remarkable opacity in the left maxillary sinus at four months after sinus augmentation via lateral window (SALW).
3. Case 2. Preoperative chronic maxillary sinusitis
A 68-year-old male (patient 2) was referred to the Department of Oral and Maxillofacial Surgery to evaluate maxillary sinus disease and dental implant placement on the left posterior maxilla. Radiographic examination revealed complete opacity and approximately 2~4mm of available bone height in the left maxillary sinus (Fig. 2A to 2C). Because the suspicious chronic maxillary sinusitis was asymptomatic, despite a detailed explanation, the patient stubbornly refused referral to the Department of Oral and Maxillofacial Surgery or Otolaryngology in a hospital setting for further evaluation and treatment of ostium patency and asked for the treatment of MSDs and implant placement in our clinic. After suggesting the possibility of referral and surgical intervention of the ostiomeatal unit enlargement in the future, medication, including antibiotics, anti-inflammatories and nasal decongestants, was prescribed three times a day for one week before surgery. Then, debridement of inflamed tissue was done via the lateral bone window, followed by simultaneous SALW with bone substitute. At four months after SALW, dental implants were placed on the left maxillary molar area after reduced mucosal thickening less than one-half of the maxillary sinus was identified in panoramic radiograph (PAN) and cone beam computed tomography (CBCT) (Fig. 2D to 2F). Eighteen months after delivery of the definitive prosthesis, CBCT revealed a recurrence of opacification in the left maxillary sinus. Though no symptom or sign of a chronic inflammatory condition was detected, it remains under surveillance (Fig. 2G to 2I).
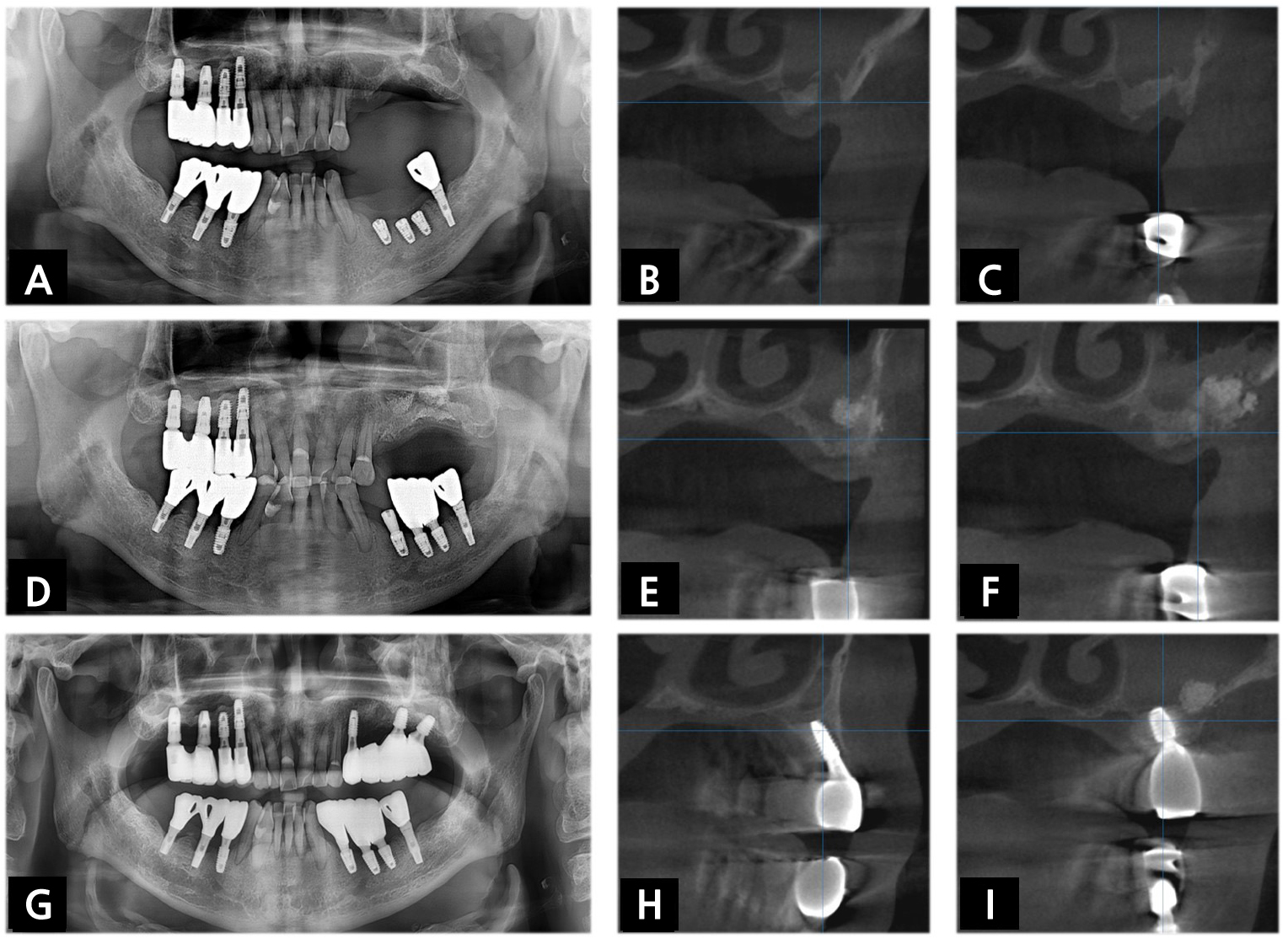
Fig. 2.
(A) Preoperative PAN and (B, C) CBCT of patient 2 revealed complete opacification in the left maxillary sinus. Before the sinus augmentation, (D) Follow-up PAN and (E, F) CBCT revealed reduced mucosal thickening in the left maxillary sinus. (G) Postoperative PAN and (H, I) CBCT demonstrated recurred opacification in the left maxillary sinus 18 months after delivery of the definitive prosthesis.
4. Case 3. Postoperative maxillary sinusitis following sinus augmentation via transcrestal approach
A 41-year-old female (patient 3) was referred to the Department of Oral and Maxillofacial Surgery to evaluate acute maxillary sinusitis after bone-added osteotome sinus floor elevation with simultaneous dental implant placement on the left maxillary 2nd molar. The patient complained about purulent nasal discharge and pain in the left midfacial area. Radiographic examination revealed no remarkable migration of graft material but opacification exceeding 50% of antral volume on the left maxillary sinus (Fig. 3A and 3B). The dental implant fixture was immediately removed, and nasal decongestants were prescribed. Three months after the fixture removal, the intact mucosal lining of the maxillary sinus was observed (Fig. 3C and 3D), and SALW was performed with bone substitute (Fig. 3E and 3F). The dental implant was replaced on the left maxillary 2nd molar four months after SALW, and the definitive prosthesis was delivered and surveilled for nine months.
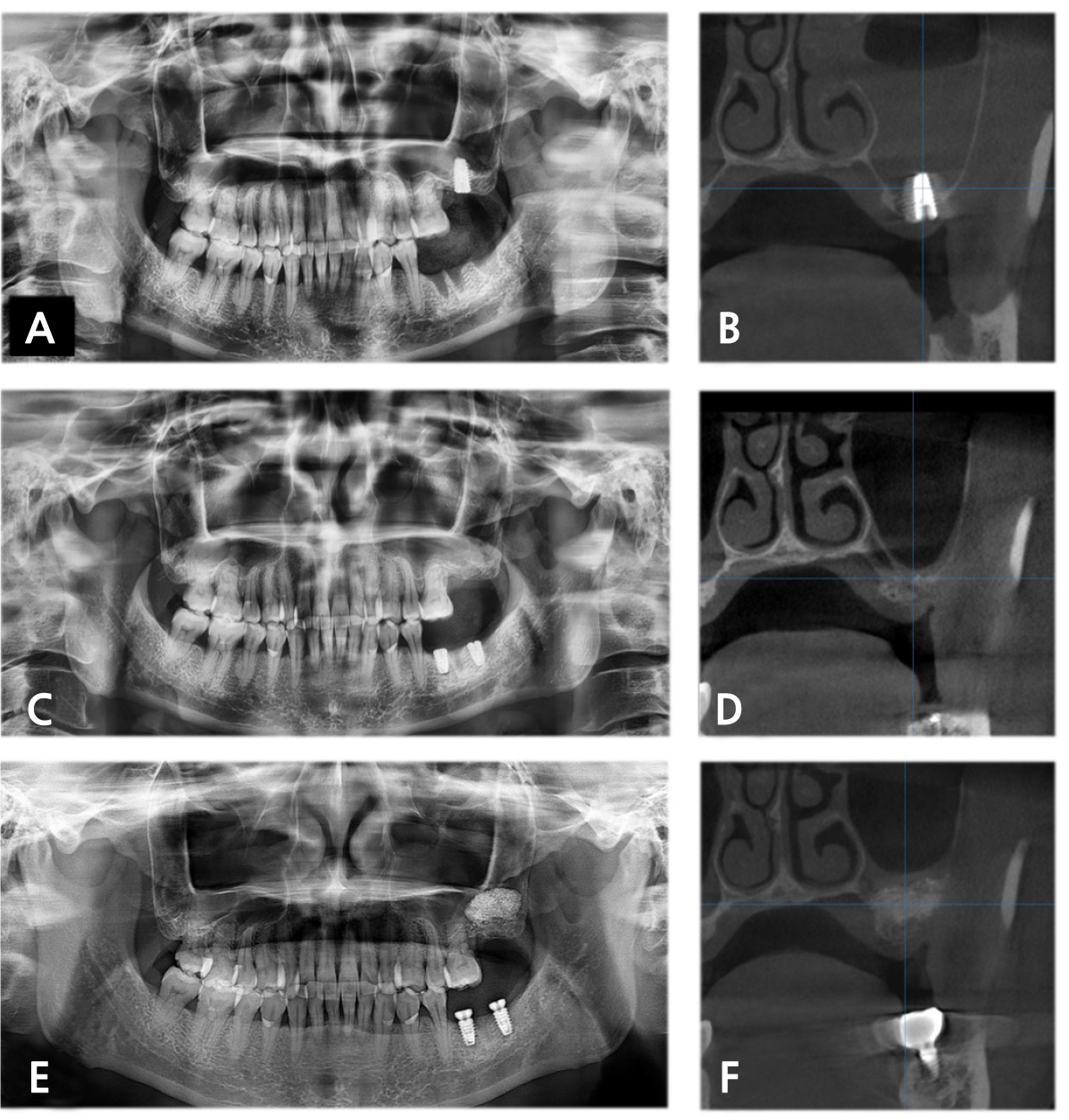
Fig. 3.
In the 1st attempt at dental implant placement in patient 3. (A) Immediately postoperative PAN revealed suspicious perforation of the sinus floor and Schneiderian membrane. One week after 1st attempt, (B) CBCT showed opacification exceeding half of the antral volume in the left maxillary sinus. Three months after removing the fixture, (C) PAN and (D) CBCT showed intact mucosal lining of the maxillary sinus. Four months after SALW, (E) PAN and (F) CBCT demonstrated no remarkable opacification.
5. Case 4. Postoperative maxillary sinusitis following SALW
A 61-year-old male (patient 4) visited the Department of Oral and Maxillofacial Surgery for dental implant placement on the left posterior maxilla. SALW with bone substitute and placement of dental implants were simultaneously performed. Immediate postoperative radiographic examination revealed the intact status of the mucosal lining and bone augmentation of the left maxillary sinus (Fig. 4A). Ten days after the procedure, however, the patient complained about purulent nasal discharge, foul odor and headache on the ipsilateral side. After taking PAN showing the migration of bone graft material, lavage and removal of bone graft material from the sinus cavity were performed (Fig. 4B). Subsequent PAN showed scattered bone graft material in the sinus cavity, and further lavage was performed (Fig. 4C). During the follow-up period from the lavage procedure on the sinus cavity, symptoms of acute maxillary sinusitis subsided. At four months after implant placement and SALW, favorable osseointegration was confirmed, and the definitive prosthesis demonstrated favorable clinical and radiological findings at 18 months after delivery (Fig. 4D).
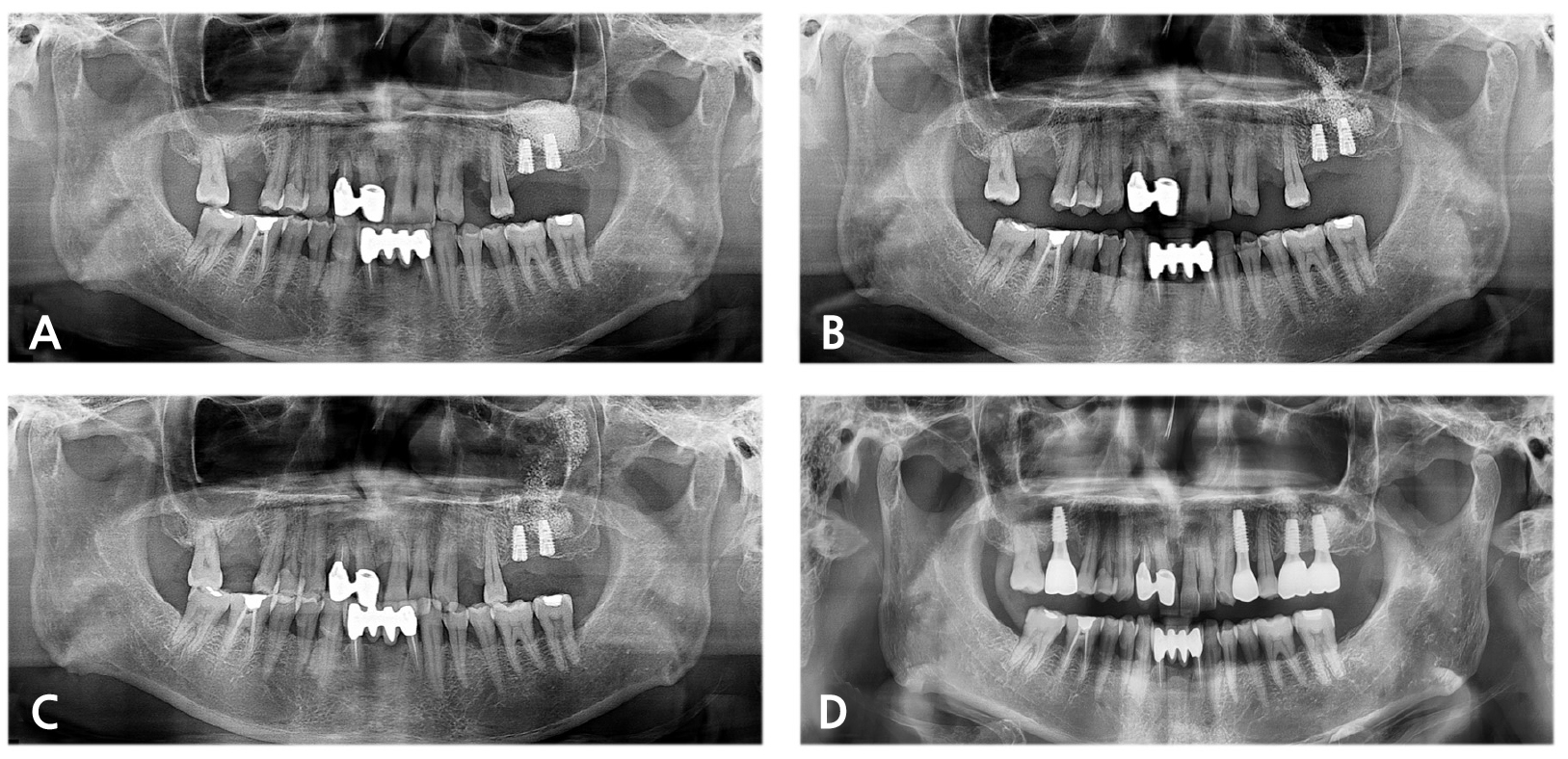
Fig. 4.
(A) Immediately postoperative PAN of patient 4 revealed no remarkable findings on the left maxillary sinus. Ten days after SALW, (B) PAN showed migration of graft material and opacification in the left maxillary sinus. During the lavage of the maxillary sinus, (C) PAN still showed disseminated graft material within the maxillary sinus, (D) Eighteen months after the definitive prosthesis delivery, no remarkable pathologic condition was identified.
Ⅲ. Discussion
1. Preoperative assessment and management of maxillary sinus disease
To minimize perioperative complications in the sinus augmentation, the thickness of the Schneiderian membrane and pathologies, including chronic maxillary sinusitis, mucous retention cyst (MRC) and tumor, should be identified before surgery. To detect those risk factors at preoperative diagnosis, conventional computed tomography (CCT) or CBCT is an essential modality, as well as plain X-ray including PAN, water’s view and lateral view.15,18 CBCT has been documented to have several benefits of low radiation dose, low sensitivity to metallic artifacts and higher spatial resolution compared to CCT.19 With a large FOV, CBCT could provide sufficient information for preoperative diagnosis from floor to ostiomeatal complex in the maxillary sinus.
Based on the interpretation of CBCT findings, the thickening of the Schneiderian membrane is frequent, with a 20.2–28.2% incidence rate.19,20,21,22 Morphology and thickness of the Schneiderian membrane must be analyzed for preoperative medical or surgical management before surgery. On the premise that the ostium patency is verified, researchers have documented that flat basal type or flat type thickening less than one-half of the antral volume indicates sinus augmentation.19,23 Cystic or dome-shaped thickening is reported to have an 8.9–22.6% incidence rate, of which fluid should be examined by aspiration for diagnosis. Those conditions between 10–15 mm diameter in CBCT findings, which is less than one-half of the maxillary sinus height, could be candidates for sinus augmentation. However, should a large cystic lesion or polyp be elevated and alter the patency of natural ostium, surgical intervention, including conventional transoral antrostomy or functional endoscopic sinus surgery (FESS), would be considered.19,22,23 For flat but circumferential or irregular thickening, additional surgical interventions must be carefully considered due to the risk of obstructing the natural ostium.19 Chronic maxillary sinusitis specified as air-fluid level or opacification exceeding one-half of the antral volume at a 3.6–6.5% incidence rate might require conservative therapy with administration of antibiotics, decongestants, antihistamines and steroids for a favorable surgical environment in the maxillary sinus.18,19 For drug-resistant chronic maxillary sinusitis, the abovementioned surgical intervention should be implemented for sinus augmentation.23 In Case 2 in this report, in which the patient refused the surgical intervention, the drug-resistant chronic maxillary sinusitis consequently recurred within one year after the sinus augmentation.
When intramural calcification is detected, the location and shape of the calcification should be assessed for differential diagnosis and surgical intervention between fungal sinusitis and non-fungal, inflammatory sinusitis, including mucocele or bacterial sinusitis. In CBCT, central calcification with a fine punctate shape is commonly presented in fungal sinusitis, whereas peripheral calcification with a round or eggshell shape occurs in non-fungal sinusitis.24 When heterogeneous soft-tissue density and destruction of adjacent structure is observed, prompt biopsy should be performed for pathologic confirmation in maxillary sinus tumor, which requires an ablative surgery as a contraindication of sinus augmentation.19,22,23 Abovementioned abnormal findings in the maxillary sinus usually require surgical interventions in a hospital setting. Interdisciplinary therapy with the Department of Oral and Maxillofacial Surgery or Otorhinolaryngology should be considered for proper ventilation and drainage of the maxillary sinus. As a surgical intervention for successful sinus augmentation, functional endoscopic sinus surgery (FESS) should be performed for ostium obstruction, chronic fungal or non-fungal sinusitis and nose deformity.22
2. Intraoperative complications in sinus augmentation
Among the intraoperative complications during sinus augmentation documented in previous literature, Schneiderian membrane perforation is the most frequent, with a wide incidence rate (11–56%).3,11,13,14,25 If Schneiderian membrane perforation is not adequately managed in the immediate postoperative period, it can lead to inadequate stabilization or delayed dissemination of graft material into the sinus.13 It remains controversial, but Schneiderian membrane perforation has been documented to have a significant association with the incidence of postoperative complications of sinus augmentation.3,26 Another intraoperative complication is the iatrogenic blockage of the ostiomeatal complex. Though infrequent, it should be avoided since it can injure the normal physiologic function of the maxillary sinus.14
3. Management of postoperative maxillary sinusitis
Postoperative maxillary sinus, the most common surgical complication after augmentation procedure, can be evoked by various clinical features: (1) pre-existing pathologic condition including chronic fungal/bacterial sinusitis or large mucous retention cyst; (2) postoperative inflammatory changes altering normal physiologic sinus function; (3) blockage of ostiomeatal complex by intra-sinus bleeding, graft material, thickened membrane or MRC; (4) bacterial contamination of graft material after recognized or unrecognized perforation of Schneiderian membrane.8,11,12,14,27,28,29 At 1–2 weeks after the sinus augmentation, postoperative maxillary sinusitis presents with acute symptoms of fever, swelling, pain, foul odor, congestion, postnasal drainage or purulent discharge from oroantral fistula.18 According to previous studies, along with systemic antibiotics, anti-inflammatory agents and nasal decongestants, surgical approaches may be considered for managing postoperative maxillary sinusitis. Drainage via minimal antrostomy could be the treatment of choice unless signs of infected graft material are apparent. For graft material stability and direct viewing of antral lavage, separate antrostomy through the canine fossa might benefit the drainage procedure.30,31 In case of graft infection, oroantral fistula (OAF) or refractory postoperative maxillary sinusitis not responding to the above treatments, a complete debridement is required via previous antrostomy area combined with OAF closure procedure for the remission of maxillary sinusitis and further re-entry of augmentation. Concurrent FESS could be considered if necessary for the above procedures.10,14,18
4. Prognosis of dental implant placed following surgical complications
The impact of sinus membrane perforation on the survival and success of dental implants placed in the augmented maxillary sinus is still controversial, but most of the literature characterizes membrane perforation as having no statistical significance in terms of dental implant survival on the augmented maxillary sinus.3,15,25,32 Karabuda C. et al. reported that perforation of the sinus membrane does not compromise the overall survival and success of 259 dental implants placed in the augmented maxillary sinus.15 Oh E et al. documented that perforation of the sinus membrane had no negative long-term effects on 175 augmented sinuses and 438 dental implants.32 From a meta-analysis of 388 Schneiderian membrane perforations out of 1652 sinus augmentation cases by Al-Dajani M et al., the overall survival rate of dental implants in the perforated side was 93% (range, 76.2–100%), and in the nonperforated side 98.1% (range, 95.6–100%), not a statistically significant difference.25 Schwartz-Arad D. et al. demonstrated no significant association between Schneiderian membrane perforations and dental implant survival.3
Ⅳ. Conclusion
The present case series study reported on clinical courses of the sinus augmentation procedure with respect to managing predisposing maxillary sinus pathology or postoperative maxillary sinusitis. Based on the evaluation of anatomic variation and pathologic conditions of the maxillary sinus, surgical interventions should be determined before the sinus augmentation procedure.
