

Ⅰ. Introduction
Various treatment modalities, such as complete dentures, implant-supported overdentures, and fixed implant-supported prostheses, can be considered for treating edentulous patients.1 While removable dentures are hindered by maintenance difficulties and masticatory ability inefficiencies, implant-supported prostheses are a commonly accepted treatment because of their high success rate and long-term stability.2 In young patients, implant treatment may be preferred in terms of psychological satisfaction, even in cases of severe bone resorption which are challenging for clinicians.
The sequelae of alveolar bone resorption and the structural changes following tooth extraction are inevitable biological processes.3 In the anterior part of the maxilla, horizontal bone loss involving resorption of the facial bone plate is prominent, often resulting in the sharp edge form of the alveolar crest.4 Alveolar ridge preservation and additional bone augmentation with various bone graft materials are favorable treatment options to overcome this.5,6 In the posterior part of the maxilla, sinus pneumatization is one of the most common problems for implant placement. The sinus lift procedure is used to overcome this because it is predictable with a high implant success rate.7,8 Clinically and radiographically, detailed examinations must precede the sinus surgery because of anatomical difficulties and maxillary sinus complications during or after the surgery. Preoperative chronic rhinosinusitis is one of the most frequently occurring maxillary sinus diseases that can affect postoperative complications after dental implantation.9 Therefore, if an abnormal sinus condition is suspected on the basis of radiographical findings, patients must be referred to an otolaryngologist in advance to minimize potential risks.
In this case, we report seven implants that were placed after extracting the entire remaining maxillary dentition impaired by chronic periodontitis using guided bone regeneration (GBR) for horizontal augmentation in the anterior bone defect and bilateral sinus lift. We consulted with an otolaryngologist for patients with chronic rhinosinusitis.
Ⅱ. Case Report
A 47-year-old male patient visited our hospital with a discomfort due to mobility of the remaining teeth and reduced masticatory function. The patient had been using a removable partial denture with a six-unit fixed prosthesis from the upper right canine to the upper left canine. Panoramic view revealed severe vertical resorption of both posterior alveolar bone (Fig. 1A) and remaining hopeless teeth with chronic periodontitis (Fig. 1B). The patient’s condition required overall restoration after extraction of all remaining maxillary dentition. The patient also showed peri-implant disease and vertical bone resorption in the lower jaw with inappropriately placed implants.
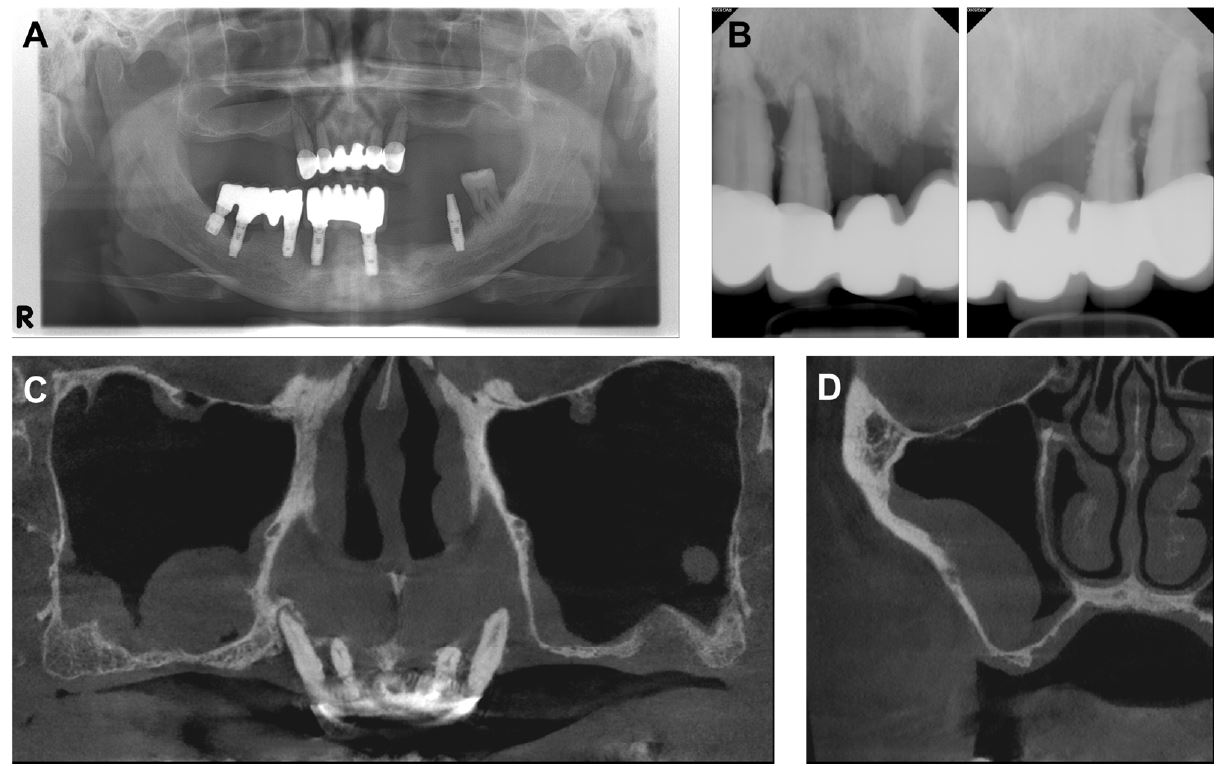
Fig. 1.
Radiographic image on first visit. (A) Panoramic view presenting alveolar bone resorption and pneumatization of both sinus floors, (B) Intraoral radiography showing the remaining tooth with chronic periodontitis, (C and D) Cone-beam computed tomography CBCT of the maxillary sinus revealing mucosal thickening, particularly in the right sinus floor.
We decided to remove all remaining implants and planned various treatment options for full mouth rehabilitation. The first option was bar-type overdenture treatment involving the placement of four implants on the maxilla and two implants on the mandible. The second option was implant-assisted removable partial denture involving the placement of five to seven implants on the maxilla with sinus augmentation and five implants on the mandibular inter-foraminal area. The third option was to construct a fixed implant-supported prosthesis with sinus augmentation and GBR for both the maxilla and mandible. Owing to the patient’s insufficient bone quantity and quality, poor oral hygiene, and long-term history of smoking, we recommended the first two treatment options to the patient because of their minimal invasiveness and requirement for a fewer number of implants. However, considering the patient’s strong preference for fixed prosthesis and long-life expectancy, the patient selected the third option. Therefore, the decision was made to construct a fixed implant–supported prosthesis with sinus augmentation and GBR.
The cone-beam computed tomography (CBCT) scan revealed severe bone loss in both the anterior and posterior areas of the maxillary alveolar bone (Fig. 1C). In addition, we observed considerable mucosal thickening of the right maxillary sinus floor extending more than one-third of sinus height (Fig. 1D). When informed about the radiographic signs, the patient reported medical history pertaining to respiratory problems and nasal symptoms, which had been persistent for more than several months prior to the visit. We then referred the patient to an otolaryngologist for examination and treatment of the maxillary sinus before starting dental treatment. The patient was diagnosed with chronic rhinosinusitis by the otolaryngologist and was advised to undergo dental surgery after several weeks of medication.
A surgical plan was established to place seven implants in the maxilla with additional bone graft; a sinus lift was planned in both posterior maxillae after the extraction of all remaining teeth. The remaining teeth (#13, #12, #22, and #23) were extracted under local anesthesia (2% lidocaine with 1:100,000 epinephrine; Yuhan, Seoul, Korea) (Fig. 2A). After extraction, the socket was grafted, and the thin labial plate was horizontally augmented with xenogeneic bone (Bio-Oss; Geistlich Pharma AG, Wolhusen, Switzerland) (Fig. 2B). Resorbable collagen membrane (Bio-Gide; Geistlich Pharma AG) was placed to promote GBR (Fig. 2C). A membrane fixation suture was performed for the stability of the grafted bone, and a releasing incision was performed for primary closure without tension using a 5-0 absorbable suture (Monosyn; B Braun, Melsungen, Germany) (Fig. 2D).
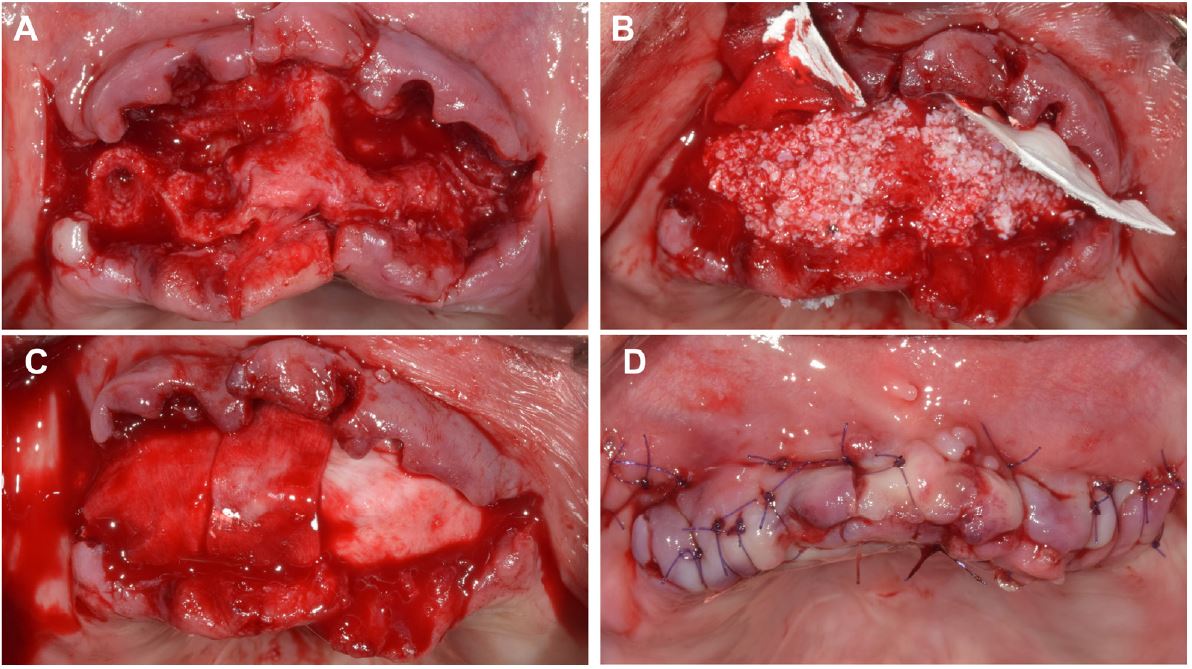
Fig. 2.
Clinical photographs of guided bone regeneration. (A) Compromised socket with severe alveolar ridge resorption is observed after teeth extraction, (B) Xenogeneic bone materials are grafted, (C) Resorbable collagen membrane is covering the grafted site, (D) Tension free suture is performed with a releasing incision.
During the healing period, chronic rhinosinusitis was successfully resolved with antibiotics and bronchodilators (clarithromycin 250 mg, theobromine 300 mg, two times daily) for 6 weeks, as prescribed by the otolaryngologist.
After 2 months, sinus elevation and bone graft of the left posterior maxilla by the lateral approach were performed using xenogeneic bone (Bio-Oss; Geistlich Pharma AG) and resorbable collagen membrane (Bio-Gide; Geistlich Pharma AG) (Fig. 3A, 3B, and 3C). Primary closure was obtained by tension-free releasing incision. Two weeks later, the same procedure was successfully performed for the right maxillary sinus without any problems related to sinusitis such as suppuration or excessive bleeding (Fig. 3D, 3E). Clinical photographs showed the primary closure of the right posterior maxilla and the uneventful healing of the left posterior maxilla (Fig. 3F).
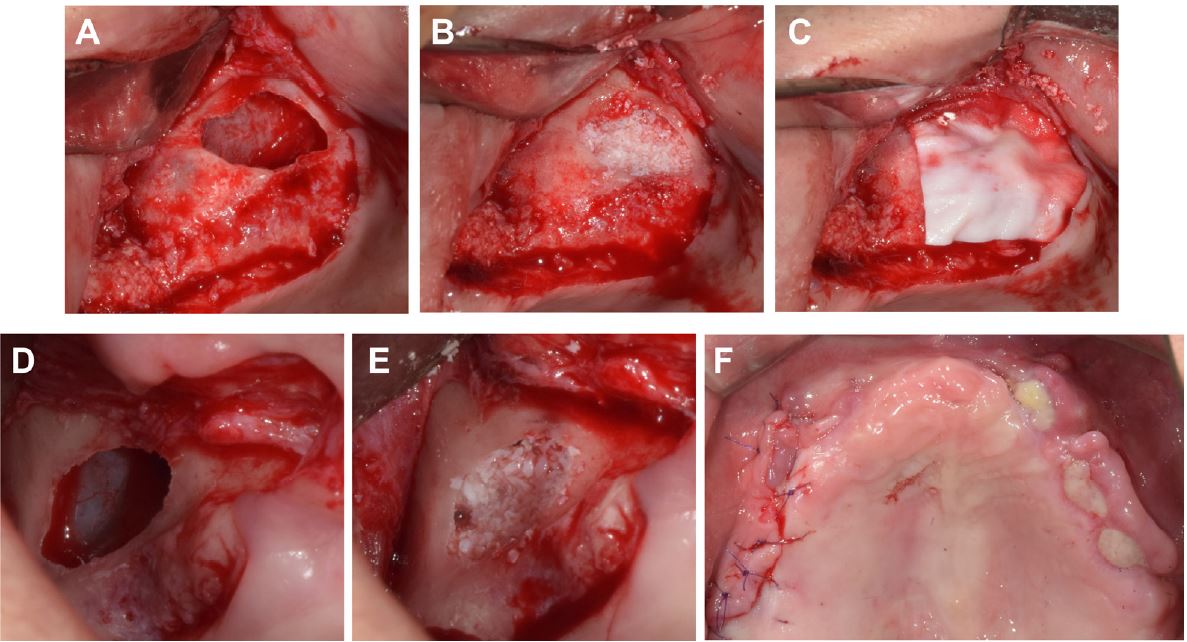
Fig. 3.
Clinical photographs of the lateral approach for sinus floor elevation and bone graft. (A) A window is opened, and the sinus membrane is elevated on the left maxilla, (B) Xenogeneic granules are grafted on the left maxilla, (C) A resorbable collagen membrane is covering the grafting material, (D) A window is opened, and the sinus membrane is elevated on the right maxilla, (E) Xenogeneic granules are grafted on the right maxilla, (F) The flap is sutured.
Postoperative CBCT revealed horizontally augmented alveolar bone in the anterior area (Fig. 4A) and vertically augmented maxillary sinus floors following successful elevation with mucosal thickening (Fig. 4B) that was reduced more than that of preoperative CBCT (Fig. 1C).
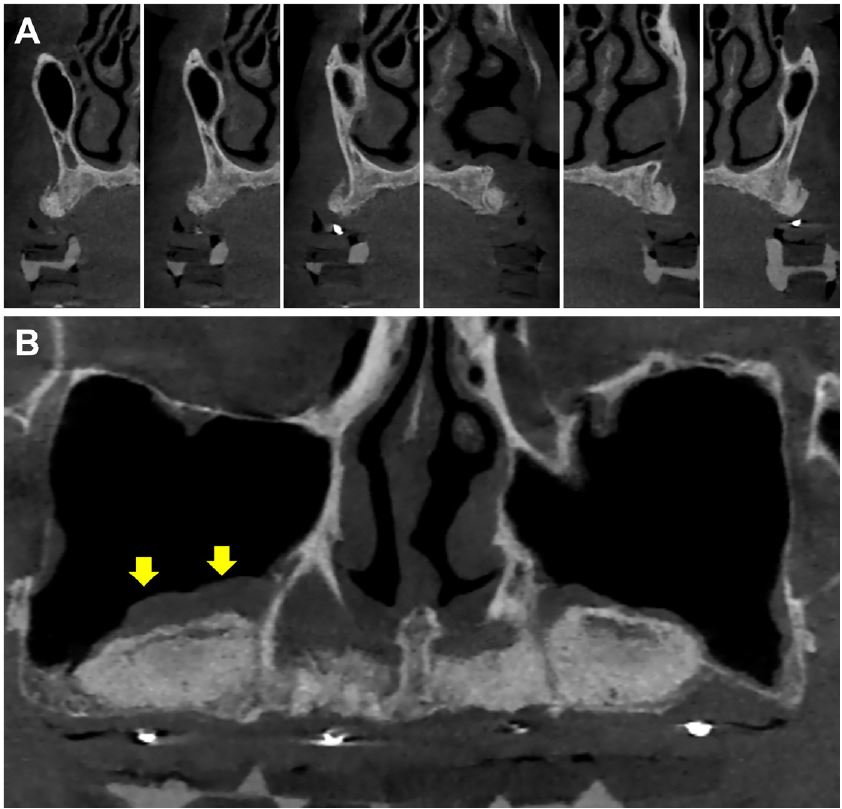
Fig. 4.
Cone-beam computed tomography (CBCT) view with radiologic guide obtained 5 months after sinus lift. (A) Horizontally augmented alveolar bone ridge in the anterior region, (B) Vertical augmentation in the sinus space is observed. Yellow arrows represent the subsided level of mucosal thickening at the right sinus floor.
After 6 months, seven implants that were sandblasted with alumina and had acid-etched surfaces (TS III SA; OSSTEM, Seoul, Korea) were placed under local anesthesia via guided surgery (OneGuide Kit; OSSTEM). A surgical guide stent was designed in collaboration with a prosthodontist for the optimal prosthodontic requirements of the precise augmented bone region using a CBCT reference image and three-dimensional (3D) implant planning software.
Minimally invasive surgery was initially attempted using a commercial guide surgery kit (OneGuide Kit; OSSTEM) (Fig. 5A); however, xenogeneic bone (Bio-Oss; Geistlich Pharma AG) was grafted onto the inter-implant area between #21i and #23i and onto the coronal part of #23i and #24i because of the exposure of one to two threads of the implant fixture. For this additional procedure, only a horizontal incision was performed (Fig. 5B). All implant fixtures achieved primary stability, and healing abutments were connected, except for implants placed in grafted sites connected by cover screws (Fig. 5C). Table 1 shows the size of the implant and the information on the initial torque.

Fig. 5.
Clinical photographs for the implant placement. (A) Implant surgery using a surgical guide with three additional anchor screws for fixation, (B) Additional bone graft is performed only for the #21i, #23i, and #24i areas, and primary closure is performed, (C) One-month postoperative follow up.
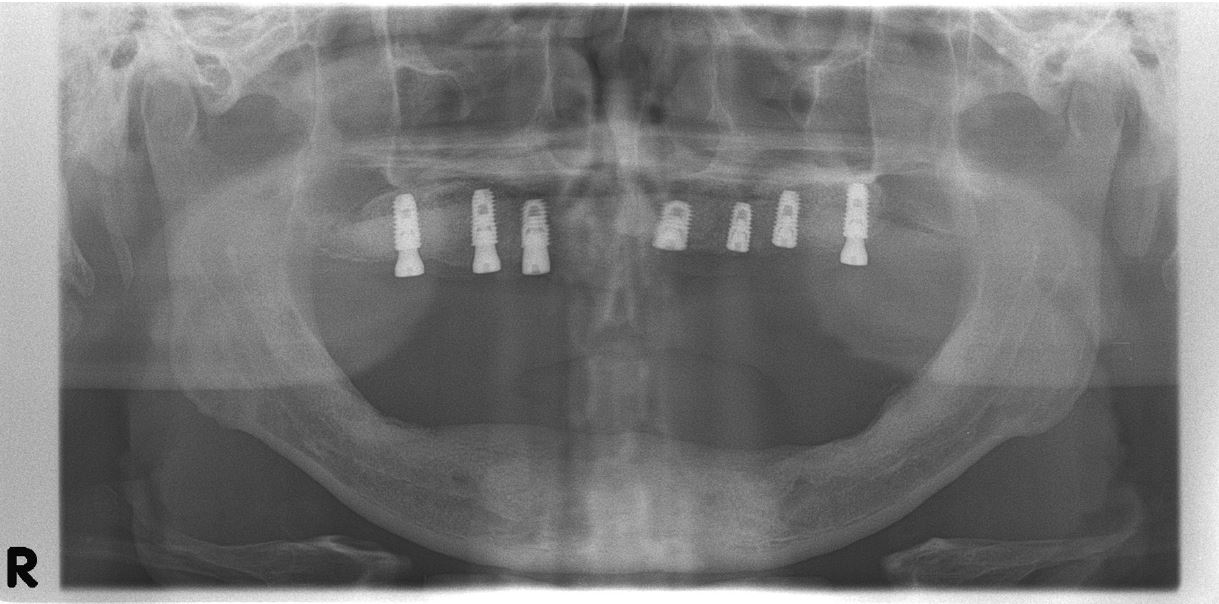
Postoperative panoramic radiography shows the precise placement of implants within the anterior and both sinus augmented areas 1 month after the surgery (Fig. 6). After the healing period, provisional denture was delivered on completely healed soft tissue and periodically adjusted to minimize the patient’s discomfort.
Ⅲ. Discussion
The placement of implant-supported prosthesis in the atrophic edentulous maxilla is often difficult because of insufficient bone caused by the severe resorption of the alveolar ridge and the pneumatization of the maxillary sinuses. The maxillary anterior alveolar bone undergoes a resorptive volume change of 29%–63% horizontally and 11%–22% vertically within 6 months after tooth extraction.10 GBR is currently the most reliable technique for horizontally reconstructing a narrow alveolar ridge because of its high predictability and low rates of complication.11
Although the sinus floor elevation and bone grafting procedure for the implant placement are associated with relatively few complications and a high success rate, the risk of complications for reconstructing the maxillary posterior area remains.12 The presence of sinusitis may negatively affect the surgical outcome (e.g., the occurrence of membrane perforation during surgery and postoperative sinus infection), thus resulting in a greater chance of implant failure.13
Among patients receiving dental implants, 24.7%–45.1% reported anomalies in the maxillary sinus during the preoperative evaluation.12,14 Even in patients with no symptoms or abnormalities during the preoperative examination, chronic sinusitis occurred in 4% after dental implantation, whereas half the patients had mucosal thickening of the maxillary sinus.15 Mucosal thickening may be one of the most common and noticeable findings in the evaluation of a sinus pathologic condition on CBCT imaging. One study reported a high risk of sinus pathology when the level of mucosal thickening was at least 5 mm.16 This is consistent with the findings of the current study, in which the patient’s mucosal thickness was 16–18 mm (as measured using a CBCT image), and the patient was diagnosed with chronic rhinosinusitis.
Rhinosinusitis is one of the most common types of sinusitis and is subdivided into the acute or chronic type depending on its onset time and the extent of clinical symptoms. Chronic rhinosinusitis is not an absolute contraindication for sinus surgery when the visible mucosal thickening is less than one-third to one-half of the maxillary sinus height.17 However, limited clinical evidence exists to predict the accurate relationship between preoperative radiographs and postoperative clinical results; inconsiderate medication has occasionally led to recurrence or even resistance to therapy. Therefore, the careful examination of patients’ medical history and symptoms in addition to radiography assessment may aid in reducing the risk of postoperative complications related to implant placement. Furthermore, medical consultation is necessary when the clinician is faced with suspected lesions in the maxillary sinus.
The accurate positioning of implants for completely edentulous patients is challenging; for this reason, in the past, cases of severe bone loss were largely considered contraindicative for implant placement. By performing bone augmentation and implant placement with a surgical guide, high accuracy of surgical procedures can be achieved, reducing technical discrepancy and anatomical damage.18 Therefore, in the current clinical case, 3D implant planning software and a surgical stent were used.
This case report showed successful implant placement after sinus elevation with proper management of common maxillary sinus pathologies without any complications during or after surgical operations. The case had a relatively short-term follow-up period for evaluation; therefore, it is limited by the absence of long-term results.
Ⅳ. Conclusion
Both GBR and bimaxillary sinus elevation with a lateral approach were adopted as treatment options for the reconstruction of the edentulous maxilla. We performed preoperative management for chronic rhinosinusitis according to the otolaryngologist’s treatment plan. Although the follow-up period was too short to evaluate the long-term success and the implants were not yet been loaded, a stable implant placement was achieved, and healthy sinus conditions were maintained without any complications for 8 months.
