

Ⅰ. Introduction
Dental implant treatment is the standard treatment for tooth loss. According to recent studies, the success rate of implants is reported to be 98.6%.1 Implant surgery can be easily applied to patients with tooth loss; however, in some patients, precise and careful surgery is needed. The failure rate of implants may increase, especially if the patient has received radiation therapy after suffering from oral or head & neck cancer or has undergone treatments such as bisphosphonate therapy.2,3 However, some previous studies present opposing opinions claiming the success of implant in irradiated patients even after many years.2, 3, 4
Radiation therapy affects not only the malignant cells itself but also the tissue and bone by damaging the vascularization and remodeling cycle which is regulated by osteoblasts and osteoclasts.5 These complications lead to poor healing of the bone, which can affect the success of dental implant treatment.6 Therefore, oral rehabilitation treatment, including dental implant treatment, for patients who have undergone radiation therapy is known to be challenging.7
Comparison of irradiated and non-irradiated patients who underwent dental implant treatment after oral cancer surgery showed differences in results and the presence of complications.8 Therefore, precise evaluation of tissue healing must be considered before applying dental implants in irradiated patients. regeneration (GBR), and chemotherapy was suggested as important variables for success of implants by previous studies.9, 10, 11, 12
This study aimed to determine the effect of radiation therapy on the survival rate of implants in long-term followed-up patients, considering factors such as the location of the implants (maxilla or mandible), average radiation dose, and type of oral cavity or head and neck cancers that the patient had.
Ⅱ. Materials and methods
This study included patients who visited the Department of Oral and Maxillofacial Surgery for dental implant treatment and received radiation therapy for oral cancer between 2010 and 2020. A total of 23 patients (male:female ratio = 13:10, mean age 61 years, range 44–86 years) were included. Implant surgeries were performed by an experienced surgeon. This study was approved by institutional review board (IRB) of Asan Medical Center (No. S2018-0257-0001).
A total of 83 implants were placed at various locations in the oral cavity, including the anterior and posterior areas of the maxilla and mandible (6 and 36 implants in anterior and posterior maxillary areas, respectively; 11 and 30 implants in anterior and posterior mandibular areas, respectively). Bone grafting and implant surgeries were performed in 17 patients. Of the 83 implants, 64 were applied through a one-stage surgery, and 19 through a two-stage surgery. In the case of two-stage surgery, the second surgery was performed approximately 3 months after the first. Prosthetic treatment was administered 2 weeks after the one-stage or the second surgery. Follow-up checks for dental implant status were performed at intervals of 3 months in the first year, 6 months in the second year, and 1 year from third year onwards. The latest follow-up year varied among the patients, and the total follow-up period ranged from 2 to 142 months.
The cumulative survival rate (CSR) was analyzed by the Kaplan–Meier analysis, considering variables such as the location of the dental implant, average radiation dose, and types of cancers that patients had. The variables for implant placement location were analyzed by classifying with respect to the maxilla and mandible. In oral cavity cancer, the implantation and irradiation sites are near or at least on the same side of the jaw, which indicates that the implantation site has been under the direct effect of the radiation. However, in other head and neck cancers, the implantation site differs from the irradiation site, indicating that radiation has an indirect effect on the implantation site. In addition, variables for average radiation dose were analyzed by dividing them into groups of radiation doses ≥60 Gy and <60 Gy. The radiation dose after oral cavity cancer and other head and neck cancers was analyzed based on the general principles of radiotherapy. For curative intent, the total cumulative dose is 66–74 Gy, which is >60 Gy on average, and in the case of postoperative therapy, it is 50–66 Gy.13 Finally, variables for cancer types were analyzed by dividing them into groups of oral cancer and other head and neck cancers. In this study, oral cavity cancers included tongue, bottom-of-tongue, maxillary, and mandible cancers. The other head and neck cancers included tonsil, esophageal, nasopharyngeal, supraglottic, and thyroid cancers. Implant placement was considered successful if the implant lasted until follow-up checks with no mobility, absence of pain or bleeding, and minimal marginal bone level change.14
Ⅲ. Results
A total of 83 dental implants were placed in 23 patients. Average rest period between radiation therapy and the first implant surgery for each fixture was 6.46 years, and average radiation dose for the radiation therapy was 56.97 Gy. The mean follow-up period after implant insertion was 5.16 years.
There were two cases of death during the follow-up period. Seven of the 83 implants failed. Among the seven failure cases, two implants were applied in the posterior maxillary area, four in the posterior mandibular area and one in the anterior mandibular area.
The overall implant CSR was 91.6% when analyzed using the Kaplan–Meier method. Regarding the location of the implants, the CSR was 95.3% for implants in the maxilla and 87.5% for implants in the mandible (Fig. 1 and Table 1). In contrast, when the radiation dose was applied to the analysis, the CSR with a radiation dose <60 Gy was 91.7% and with that of ≥60 Gy was 91.5% (Fig. 2 and Table 2). The type of cancer reflected the location of the radiation received by the patient, and this variable affected the CSR of the implants. The CSRs for patients with oral cavity and other head and neck cancers were 82.9% and 100%, respectively (Fig. 3 and Table 3).
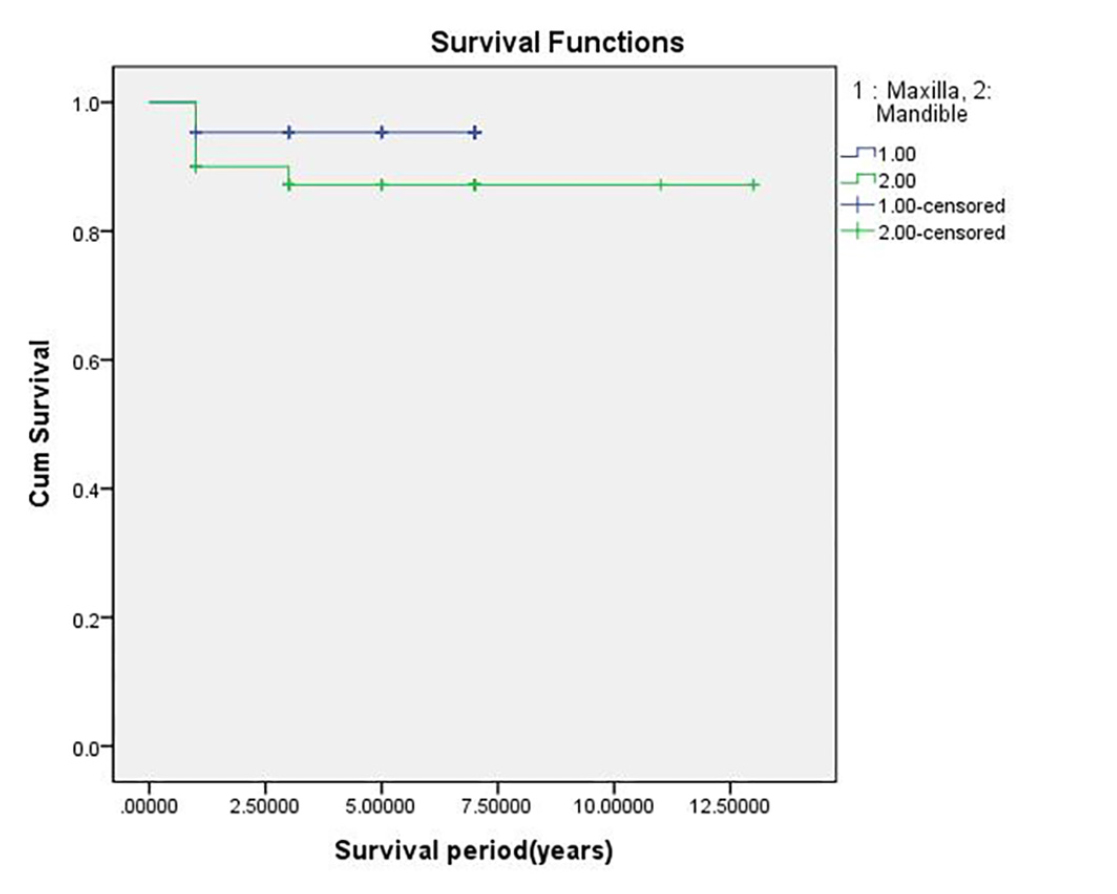
Table 1.
Overall cumulative survival rate (CSR) of implants considering the implantation location (1: Maxilla, 2: Mandible). Considering the location of the implants, the CSR is 95.3% for implants in the maxilla and 87.5% for those in the mandible
| Implant location | Placed implant | Failed implant | Survival implant | CSR |
| Maxilla | 43 | 2 | 41 | 95.3% |
| Mandible | 40 | 5 | 35 | 87.5% |
| Total | 83 | 7 | 76 | 91.6% |
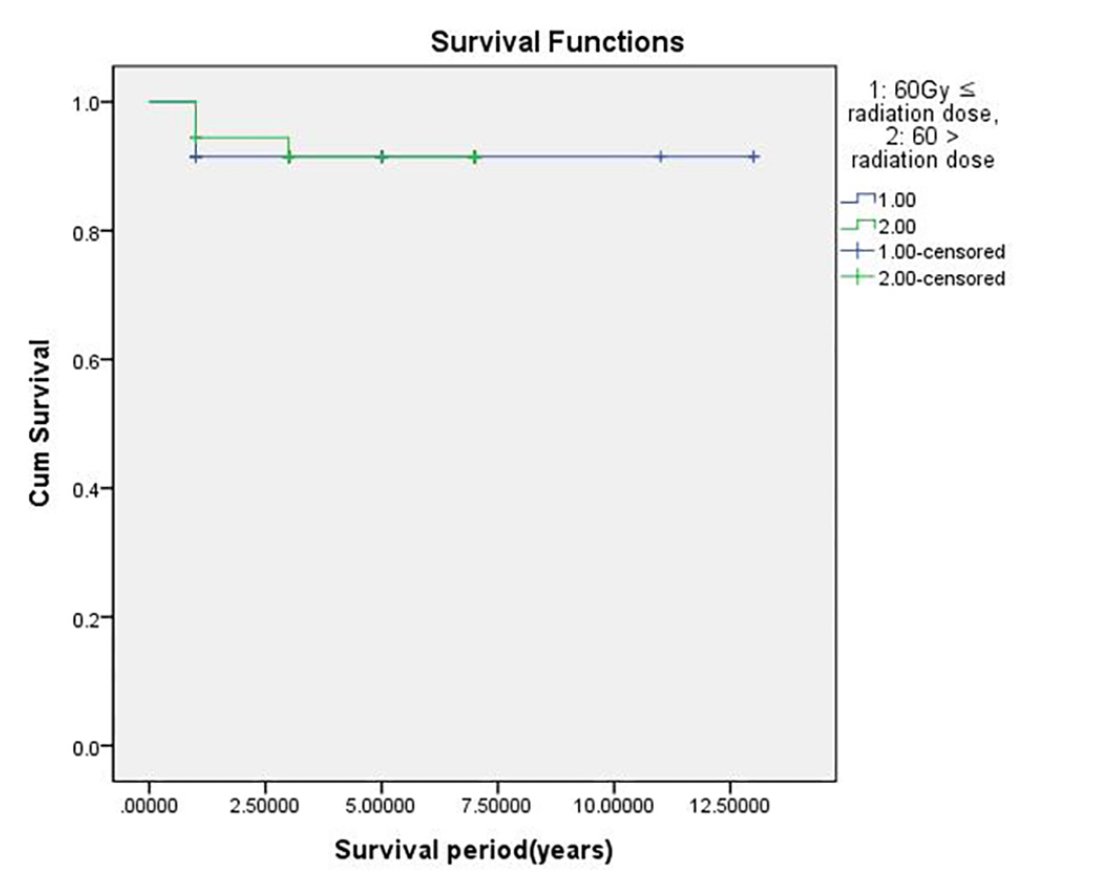
Table 2.
Overall cumulative survival rate (CSR) of implants considering the dose of radiation (1: radiation dose <60 Gy, 2: radiation dose 60 Gy). CSR of implants with a radiation dose <60 Gy is 91.7% and that with a radiation dose ≥60 Gy is 91.5%
| Radiation dose | Placed implant | Failed implant | Survival implant | CSR |
| 60Gy ≤ radiation dose | 47 | 4 | 43 | 91.5% |
| 60 > radiation dose | 36 | 3 | 33 | 91.7% |
| Total | 83 | 7 | 76 | 91.6% |
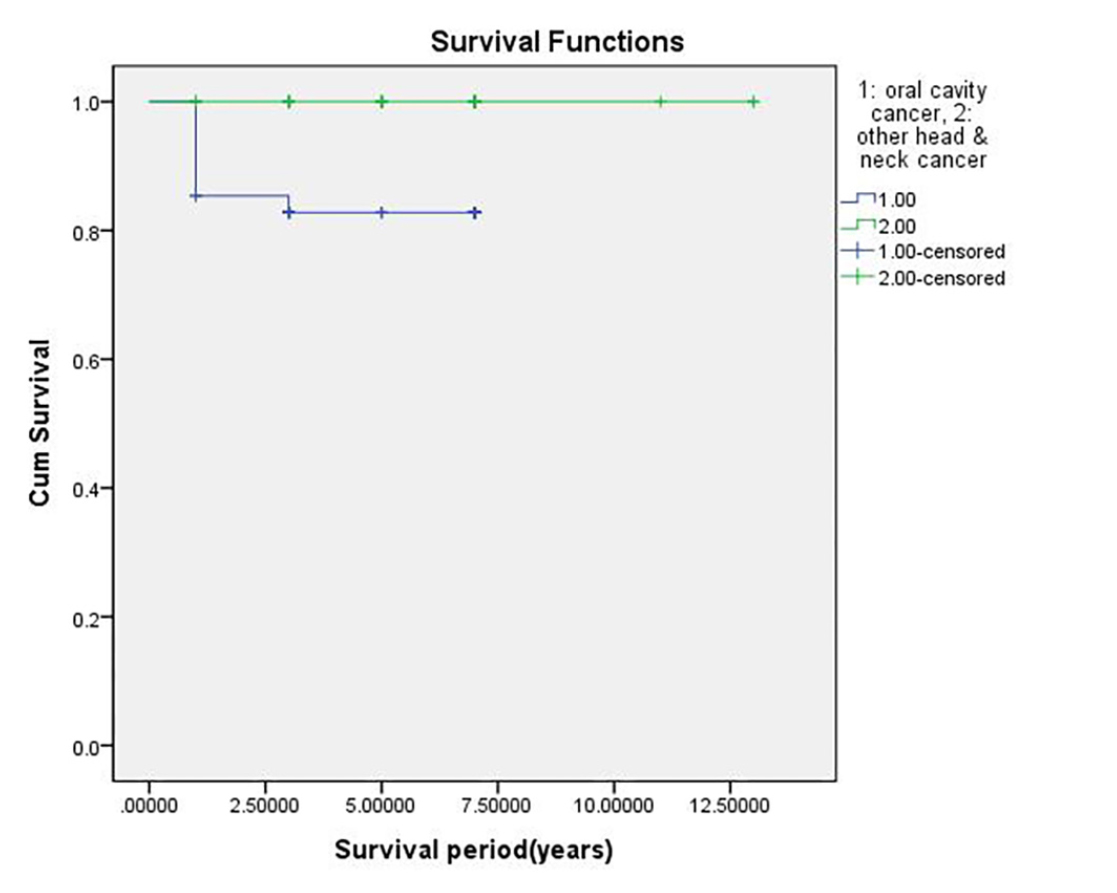
Table 3.
Overall cumulative survival rate (CSR) of implants considering the types of cancer (1: oral cavity cancers, 2: other head and neck cancers). CSRs of implants in patients with oral cavity cancers and other head and neck cancers are 82.9% and 100%, respectively
| Cancer type | Placed implant | Failed implant | Survival implant | CSR |
| Oral cavity cancer | 41 | 7 | 34 | 82.9% |
| Other head & neck cancer | 42 | 0 | 42 | 100.0% |
| Total | 83 | 7 | 76 | 91.6% |
Ⅳ. Discussion
According to previous research, there was a low success rate of implantation in the area treated with radiation.2, 3, 15 However, there were contradicting findings showing a good survival rate of implants inserted in irradiated jaws.16, 17, 18 However, in previous studies, the variables related to radiation therapy or implant location were not clearly classified, and precise statistical data were difficult to estimate. In particular, only few studies have classified the location of implant insertion and considered the types of cancer that the patients had.
Therefore, this study analyzed variables, such as the radiation dose, implantation location, and types of cancer. The implantation location reflects the anatomical differences between the maxilla and mandible. The proportion of cortical bones in the mandible is higher than that in the maxilla, which can account for the higher success rate of implants inserted in the mandible.19 Also, the type of cancer reflects the location of the irradiated area. For example, patients with oral cancer are subjected to radiation directly through the oral cavity. In contrast, patients with other head and neck cancers, such as esophageal, supraglottic, and nasopharyngeal cancers, are subjected to indirect radiation near the oral cavity. Therefore, in of oral cavity cancer, the effect of radiation is expected to be more direct and stronger in the jaw bones than in other head and neck cancers.
However, in the case of an irradiated jaw, the critical factors determining the survival rate of implants may be different. Irradiation affects the healing process after dental implant placement, such as soft tissue healing and osseointegration.20 Lack of blood supply to the mucosal tissue and low production of saliva after radiation therapy can accelerate peri-implantitis and gingival inflammation, which can affect the survival rate of dental implants.9 In addition, osteoradionecrosis after radiation therapy can be a serious complication of dental implant treatment, and the patient may require further surgical intervention. Therefore, in this study, the higher CSR of implants in the irradiated maxilla compared to that in the mandible can be explained by the anatomical features of abundant blood supply.
According to a previous study, the radiation dose received by the patient is inversely associated with the survival rate of the implant.11 However, in this study, the average radiation dose received by the patient had no significant effect on the CSR of the implant. This finding can be attributed to the type of cancer the patient had. In cases of oral cavity cancers, including maxillary, mandibular, and tongue cancers, the range of the target radiation is closer to the implant insertion location as compared with that in other head and neck cancers. This indicates that the location and range of radiation therapy have a critical effect on the survival or success of the implant after therapy.
This study has some limitations. Variables such as patient’s history of systemic disease, additional bone graft during implant surgery, and sociocultural variables, such as sex and age, were not considered. In addition, future studies should be carried out with a larger sample size to overcome the limitation of including a relatively small number of cases.
Ⅴ. Conclusion
Within the limitations of this study, the statistical estimation of the CSR of implants considering three different variables in patients who had undergone radiation therapy was a significant and reliable analysis. This estimation can help in predicting the survival rate of dental implants and improve the quality of treatment in patients who receive radiation therapy.
