

Ⅰ. Introduction
Dental implants are widely used as a standard restorative technique for tooth loss. With advances in implant technology, the demand for dental implants is rapidly increasing, and dental implants are being used in patients of different age groups and with systemic diseases. Unfortunately, with the increase in the number of surgeries, several complications have been reported. Complications of dental implant surgery include nerve damage, infection, bleeding, bone resorption, and failure of osseointegration.1
Generally, inferior alveolar nerve (IAN) damage during mandibular implant placement is caused by incorrect localization of the inferior alveolar canal during preoperative radiographic evaluation.2 When planning for mandibular implant surgery, the length and width of the implant fixture are determined by measuring the width of the bone and the distance between the alveolar crest and IAN on panoramic radiographs3 or computed tomography (CT) images.4 However, in few cases, the bone density is too low to locate the inferior alveolar canal, or the outline of the alveolar ridge is not favorable owing to severe bone resorption. In addition, iatrogenic nerve damage can be induced even if preoperative imaging evaluation is performed because of errors in clinical evaluation, anatomical variations, or lack of operator skill. Herein, we present two cases of IAN damage and introduce factors that should be considered when planning mandibular implant surgery or removal of dislocated implants.
Ⅱ. Case report
1. Case 1
A 66-year-old woman was referred from local clinic because of fixture sinking in the #47 region during implant surgery. The patient had a brain aneurysm and carotid arteriosclerosis and took an antithrombotic agent. The patient complained of swelling and pain in the right mandible. Panoramic radiography showed that the implant fixture was located in the right inferior alveolar canal (Fig. 1A). CT showed the implant fixture near the inferior margin of the mandible (Fig. 1C) and buccal cortical bone loss at the #47 site with increased attenuation leading to the fixture (Fig. 1D). In addition, diffuse swelling was observed on the buccal side of the mandible extending to the mental foramen, that confirmed right IAN damage. Although the patient had not been previously diagnosed with osteoporosis and had no history of related medications, CT showed an osteoporotic bone pattern.
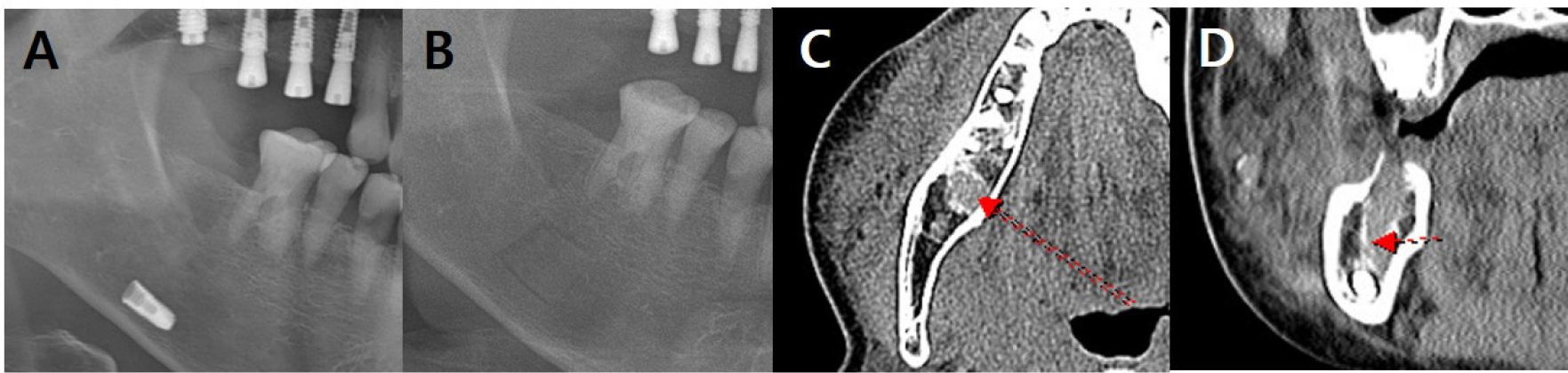
Fig. 1.
Radiographic findings in case 1 at the first visit. (A) Panoramic radiograph shows the implant in the right mandible, (B) Panoramic view after implant removal. Because the image was taken immediately after surgery, a bony window line is observed. (C, D) Coronal and axial CT images showing increased attenuation leading to the fixture. Loss of buccal cortical bone in the #47 area is observed, suggesting a post-procedural change. Diffuse swelling is observed on the buccal side of the mandible, and the mental foramen area is affected. The trajectory of the IAN is indicated by a red arrow. IAN, inferior alveolar nerve; CT, computed tomography.
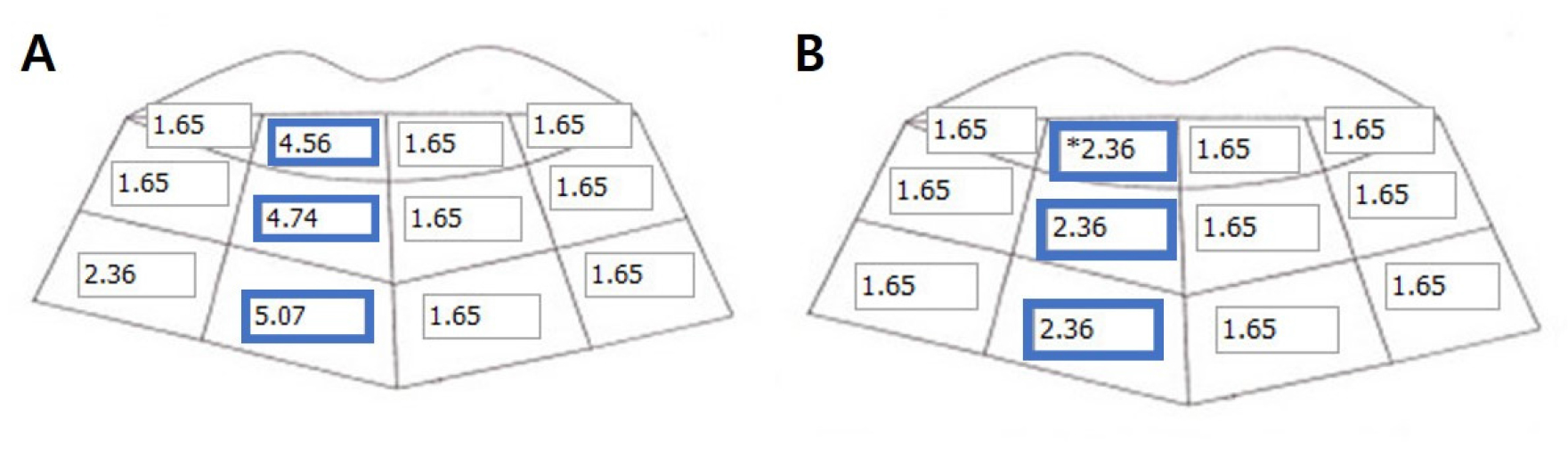
Fig. 2.
The contact threshold nerve mapping. (A) Pre-operative nerve mapping; The contact (A) pre-operative nerve mapping, (B) Post-operative nerve mapping. Improvement in all types of sensation (direction, two-point discrimination, pressure perception, and thermal sensitivity) improved after the implant removal (Blue boxes).
Nerve mapping performed one day after surgery showed a high degree of hypoesthesia. Examination based on the 'Seoul National University Dental Hospital Oral and Maxillofacial Surgery Sensory Nerve Measurement Method’ revealed contact thresholds of 1.65–5.07 and 1.65 on the right and left sides, respectively (Fig. 2A). Direction recognition was 0% and 95% on the right and left sides, respectively. The two-point discrimination threshold was > 25 mm and 10 mm on the right and the left sides, respectively. The pressure perception threshold was 170 g and 50 g on the right and left sides, respectively. Thermal stimulation revealed no sensation on the right side and sensitivity on the left side (Table 1). Based on these findings, the patient was diagnosed with hypoesthesia in the right mandible, particularly in the lower lip and chin.
Table 1.
Sensory-nerve test results. The right mandible showed lower discrimination ability than the left in all tests of the direct, two-point discrimination, pressure perception, and thermal sections. After surgery, all sensations were improved in direction, two-point discrimination, pressure perception, and thermal test
| Right | Left | ||||
| Pre-op | Post-op | Pre-op | Post-op | ||
| Direction | 0% (0/20) | 35% (7/20) | 95% (19/20) | 85% (17/20) | |
| Two-point discrimination | > 25 mm | 14 mm | 10 mm | 10 mm | |
| Pressure perception | 170 g | 35 g | 50 g | 30 g | |
| Cold perception | Not cold | Less cold | Cold | Cold | |
One day after the event, prednisolone 30 mg was prescribed for five days, followed by 15 mg for two days. Immediate removal of the foreign body under general anesthesia was planned. However, the patient was clinically diagnosed with asthma during the workup and general anesthesia was contraindicated. In addition, symptoms of upper respiratory infection appeared the day before surgery, and the risk of postoperative pulmonary complications of general anesthesia was high. Therefore, surgery was delayed until asthma control. During the systemic disease evaluation period, mecobalamin 500 mcg was twice daily for 30 days.
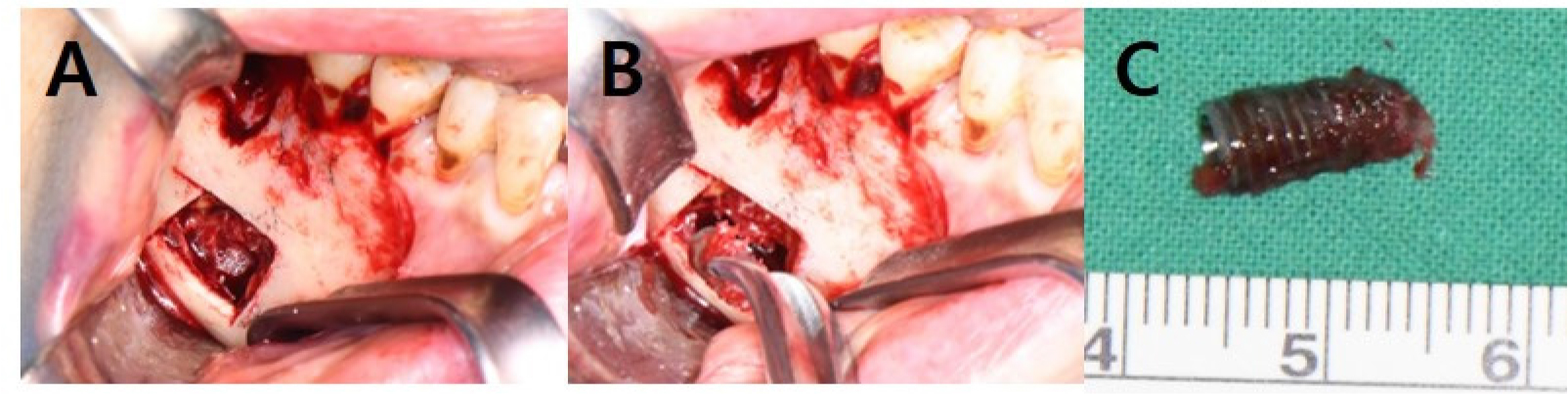
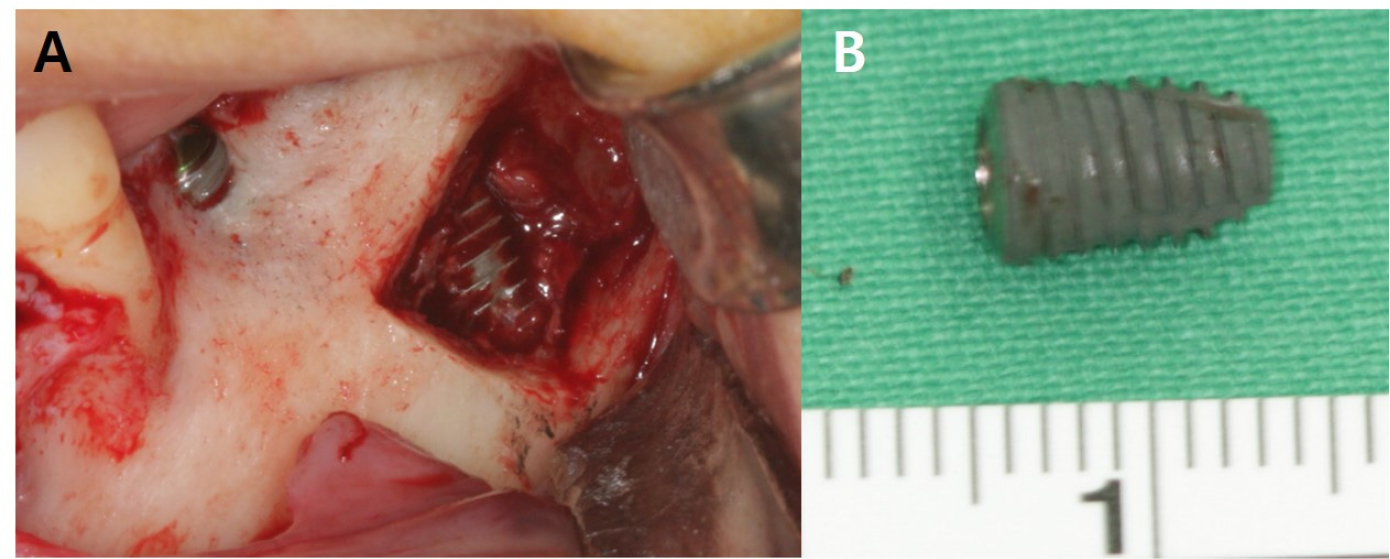
Approximately one month after the event, sensation on the right side of the lip and chin was 20–30% lower than that on the left, and the patient complained of a burning or dull feeling. The implant fixture was removed under intravenous sedation using a full-thickness mucoperiosteal incision in the buccal and posterior mucosa in the #45–47 region. Lateral subperiosteal dissection was performed to expose the right mandibular body. A bony window was created using Piezosurgery® (Mectron, Carasco, Italy) to minimize the bony gap. In addition, the inner aspect of the bony window was narrowed as much as possible to obtain sufficient stability without additional plate fixation; therefore, no additional surgery was required (Figs. 1B and 3). The implant was attached to the IAN, and dissection between the nerve and implant was performed prior to extracting it from the bone marrow. A fibrin sealant was used to cover the implant removal site and secure the bony window in its original position (Fig. 4).
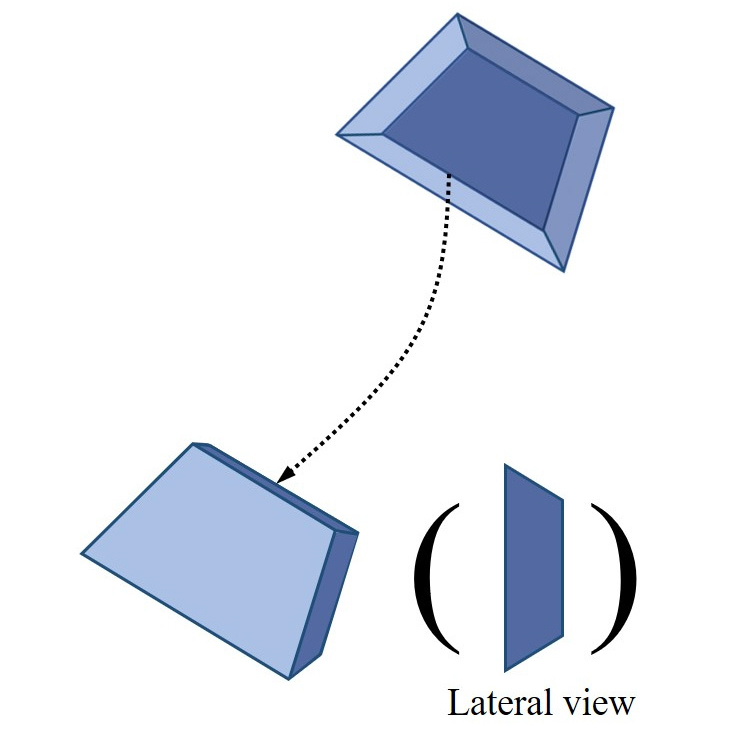
Fig. 3.
Schematic diagram of the osteotomy line. The oblique line window opening was done using piezosurgery. By performing an osteotomy along the diagonal line, the surface of the window bone was maximized, and fixation force was obtained without a plate. Since using plates and screws was not required, the possibility of subsequent bone damage and additional nerve damage could be reduced. Moreover, there was no need for further surgery, such as plate removal.
Postoperatively, the patient reported gradual reduction in dullness. However, neurological symptoms, such as a feeling of electricity on touching the lip on the right side, persisted. Nerve mapping performed two months after surgery showed improvement in hypoesthesia. The contact threshold, direction recognition, and two-point discrimination threshold on the right side were 1.65–2.36 (Fig. 2B), 35 %, and > 14 mm, respectively. The pressure perception threshold was 35 g and 30 g on the right and left sides, respectively. The temperature stimulation test revealed lesser sensitivity to cold on the right side compared with the left (Table 1). These findings suggested a partial improvement in sensation in the right mandible compared with that before the operation.
2. Case 2
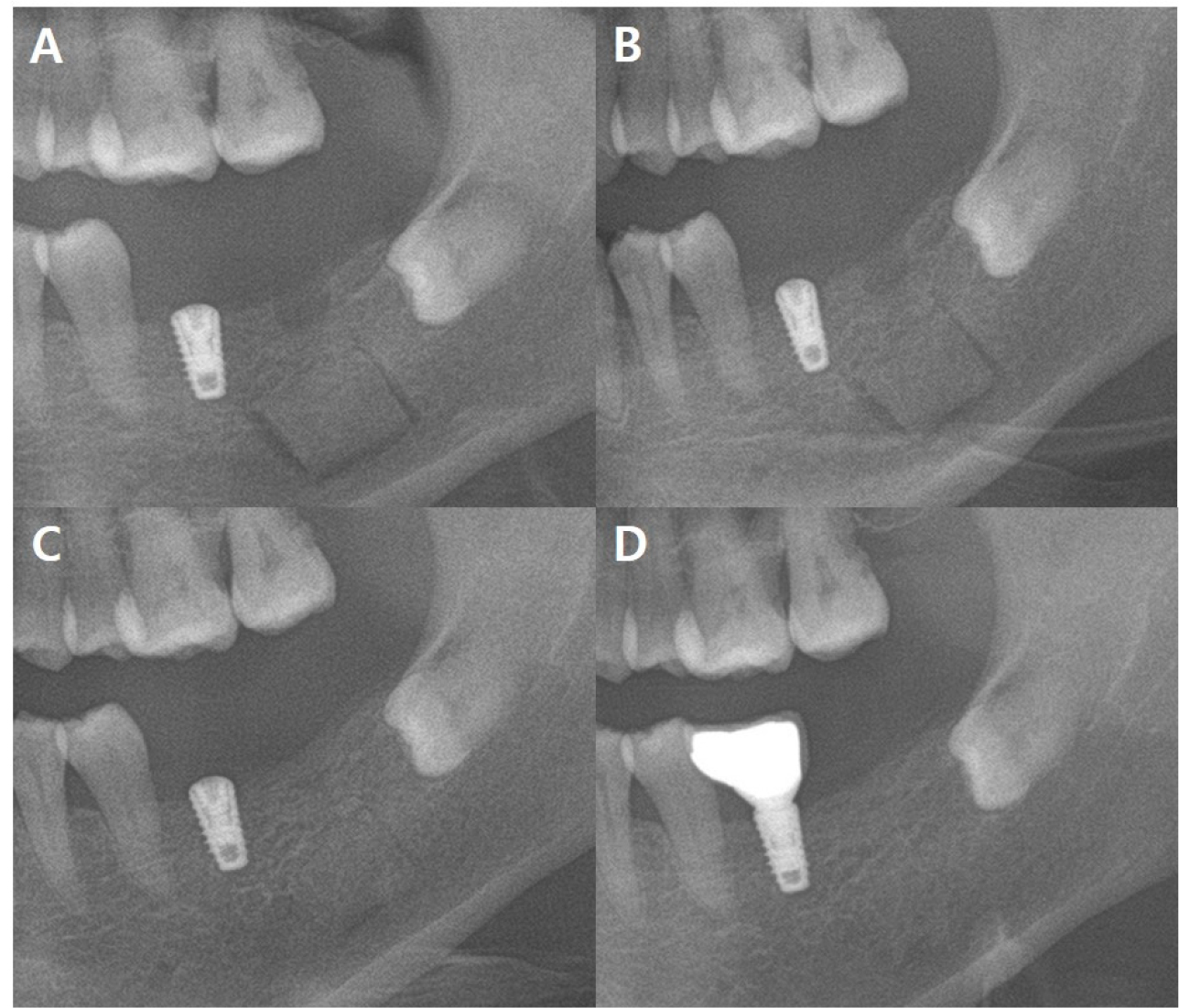
A 52-year-old woman was referred for the removal of an implant fixture in the #37 region that intruded into the mandible during implant surgery. The patient had a grade 2 intellectual disability, and the above event occurred because of a lack of cooperation during surgery. While adjusting the vertical depth using a hand wrench, the patient accidentally closed her mouth. Therefore, the implant fixture sank into the mandible. Sinking of the implant fixture in the left mandible was confirmed using CT (Fig. 5).
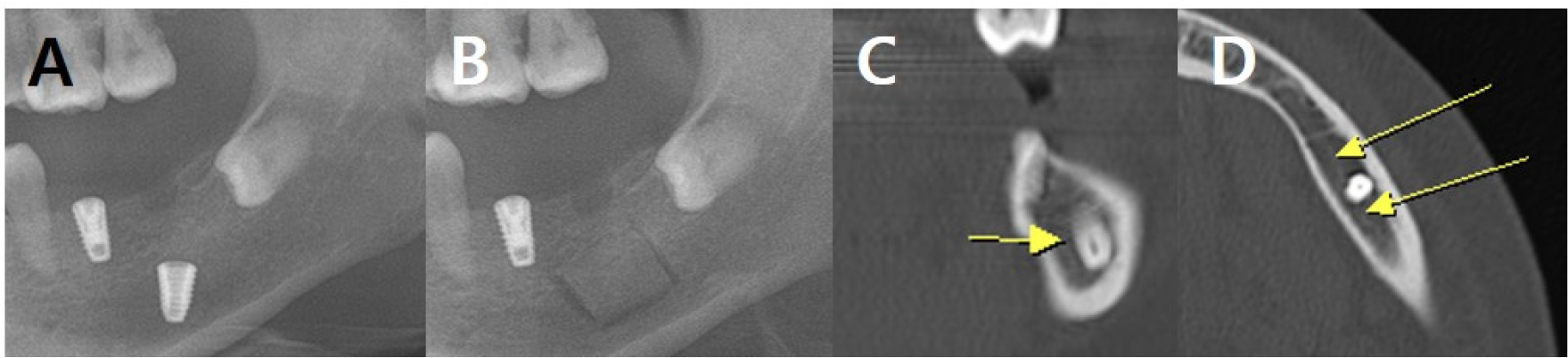
Fig. 5.
Radiographic findings in case 2 at the first visit. (A) Panoramic radiograph shows the implant in the left mandible, (B) Panoramic view showing the outline of the bony window for implant removal, (C and D) Coronal and axial CT images showing that the fixture in the #37 region is inserted almost to the lower margin of the inferior alveolar canal. The inferior alveolar canal runs biased to the lingual side, and it seems to be slightly invaded by the fixture, but it seems to be pushed to the lingual side (Yellow arrows indicate the buccal cortex of the inferior alveolar canal).
Prednisolone 10 mg four times a day for seven days and mecobalamin twice daily for seven days were prescribed two days after the event. The implant in the #37 region was surgically removed under general anesthesia 10 days after the event. The surgical technique was similar to that in Case 1. To minimize nerve damage, implant removal was performed by creating a bony window in the left buccal bone (Fig. 6) using Piezosurgery® (Mectron, Carasco, Italy). After implant removal, the bone was fixed without a plate. Although the patient could not directly express discomfort due to intellectual disability, sensory differences could be confirmed through reactions such as continuous contact with the lip. Because she had an intellectual disability, it was not possible to observe minute sensory changes through nerve mapping, as in Case 1. Postoperatively, prednisolone (5 mg four times a day ) was prescribed for 5 days. At the 2-month follow-up, mecobalamin (500 µg twice a day) was prescribed for 90 days. The 10-month follow-up image revealed adequate bone healing (Fig. 7). The patient did not show any abnormal behavior such as touching the lips, which could suggest paresthesia.
Ⅲ. Discussion
The IAN is a sensory branch of the trigeminal nerve that innervates the lower lip and chin. IAN damage can cause hypoesthesia, hyperesthesia, paresthesia, dysesthesia, or anesthesia.5, 6, 7 Since this nerve is not a motor nerve, it does not directly affect the movement of the facial muscles. However, it causes discomfort due to decreased sensation in the lower lip and chin region when talking, swallowing, and chewing, reducing the patient's quality of life.8 When a nerve is damaged, the duration and possibility of recovery vary depending on the extent of damage; moreover, complete recovery does not always occur. In case of axonal damage, recovery is incomplete even after 1 year.9 According to a meta-analysis published in 2016, 80% of patients who showed altered sensation returned to normal sensation within 6 months and approximately 91% within 1 year.10
Up to 13% of IAN damage occurs during implant fixture placement,11 which is 3.4 times higher than that occurring during third molar extraction.12 Therefore, when placing mandibular implants, it is necessary to carefully select the type of implant fixture and allow a safe area ≥2 mm from the IAN canal based on the panoramic radiography and CT findings. Second, bone density should be evaluated before implant surgery,13 and surgeons must drill more delicately during surgery, especially in middle-aged female patients.14 If bone density is low, fixture placement at the tissue level can be considered. This reduces the possibility of sinking by reducing the drilling depth. Second, the osteotomy should not be widened. In a wide osteotomy, the force required to hold the fixture in the cortical bone decreases. Further, a hand wrench must be used actively used; however, care should be taken as excessive force increases the possibility of sinking. In addition, when CT analysis shows that bone density below a certain level is expected, other restorative techniques should be given priority, or delayed implants should be considered instead of immediate implants. Furthermore, patients should be preoperatively informed of the high possibility of nerve damage because of the low bone density. Finally, patient cooperation during surgery should be considered. Even if the operation is simple, in patients with poor cooperation, general anesthesia or sedation may be considered instead of local anesthesia to ensure safety and minimize complications from implant surgery.
The IAN is a sensory nerve. Therefore, accurate evaluation and follow-up of damage are difficult. Moreover, it is difficult to estimate the post-injury sensory state. In the presented cases, nerve mapping, a sensory-nerve evaluation method used at Seoul National University Dental Hospital, was performed before and after surgery to overcome these limitations. Nerve mapping is an objective evaluation method. It evaluates the contact detection threshold for two-point discrimination and pinprick, direction perception, and thermal discrimination on applying a cold stimulus on the skin of the lower lip and chin, which the IAN innervates.15 When IAN damage is expected, nerve mapping allows close monitoring of sensory changes. This method relies on the patient's subjective sensation. However, by measuring the change, it is possible to precisely monitor nerve function before and after surgery or a drug prescription.
Piezosurgery minimizes soft tissue damage in oral surgery16 and enables precise bone removal by oscillating with an ultrasonic frequency17. In addition, unlike existing bone-reduction devices such as high- and low-speed turbines, there is no thermal damage. 18 In both our cases, a piezosurgical device was used for bone removal. The position of the sunken implant fixture was accurately determined using CT, a bony window as small as possible was created, and sufficient fixation without plate fixation was achieved by performing an inclined osteotomy. Bone healing was confirmed after 10 months.
Ⅳ. Conclusion
In middle-aged women, who are likely to have low bone density, a more delicate surgical approach is necessary during mandibular implant surgery. More care should be taken to prevent nerve damage, such as minimizing the size of the implant fixture and drilling, determining the bone density in advance using CT and panoramic radiography, and considering other anesthesia techniques if the patient's cooperation is poor. When nerve damage occurs due to a foreign body, such as a misaligned implant, it is important to minimize additional damage during removal. In addition, posttraumatic care with regular objective evaluations is important.
