

Ⅰ. Introduction
As digital dentistry has become widespread and increasingly popular in clinical practice over the past few years, the field of dental treatment using intraoral scanners and 3D printers has widened considerably. Various attempts have been made to actively utilize digital technologies for dental treatment. Digital dentistry plays an important role in implant surgery. First, the modern clinical concept has shifted from a surgically-driven approach to a prosthetically-driven approach.1 The second advantage is that the predictability in clinical and laboratory procedures has improved with the state-of-the-art digital tools.2
Implant surgical guides are great tools to assist in planning and performing implant surgery for both dentists and patients. In addition, they facilitate the proper positioning and angulation of implants when used properly. Computer-assisted implant surgery using surgical guides can be divided into computer-guided (static) and computer-navigated (dynamic) surgery. Dynamic surgical guides are based on optical and precise tracking technology so that implant placement can be observed in real time. Nevertheless, static surgical guides are more commonly used because dynamic surgical guides have limitations due to their relatively high cost and equipment space problem.3
Several types of static surgical guides have been reported based on current trends. When static surgical guides are fabricated on the model after taking an impression, they are limited to marking the initial position of implant placement.4 Since the use of computed tomography (CT) images has greatly increased in the past decades, the shape of the remaining alveolar bone can be detected in order to maintain the insertion path. In addition, various software programs have been continuously developed and adopted worldwide to establish an accurate surgical plan using cone beam computed tomography (CBCT) images and apply them to implant surgery.5 Implant surgical guides using CAD-CAM technology have been widely used in implant surgery. Consequently, their main advantages have also been reported as follows: (a) implant surgery with high accuracy, (b) reduction in technique sensitivity by the practitioner, (c) ease of use, (d) reduction in postoperative patient discomfort, and (e) improved accuracy and predictability of surgical results.4,6
The seating and stability of implant surgical guides are essential to accurately transfer the planned surgery into the oral cavity. However, in spite of many advances over the past decades of research, the factors affecting the accuracy and precision of implant surgical guides are still partially unknown.7 Although recent studies have shown that the most influential factors that may affect the stability are surgical guide support, template position, fixation, fabrication process, flap approach, and implant insertion protocol. Among these factors, surgical guide support is considered to be a very important factor in the accuracy of guided implant surgery.7 In previous studies, it was reported that the use of tooth-supported surgical guides, a key factor for success, was more stable than mucosal- or bone-supported surgical guides.8,9 In particular, because it is difficult to secure the stability of implant surgical guides for fully extracted or edentulous patients, various methods have been proposed to improve the stabilization of implant surgical guides. Anchor pins or screws are most commonly used to fix templates.10 However, this method has the following critical limitations. First, it is much more difficult to secure stability than to obtain adequate support from hard tissue. When placing an implant after fixation, saline irrigation is not allowed in the surgical area. Finally, it is not easily detachable during surgery.
Multiple implant placements after tooth extraction represent one of the most complex cases of implant prostheses. Therefore, in this case, a pre-planned treatment and its implementation are essential for precise implant positioning and angle setting, which are more difficult with free-handed surgery owing to human error.
This study was designed to explore a two-step surgical guide system to increase the stability of implant surgical guides in a patient with full extraction. In addition, this study attempted to report a clinical case in which fixed prosthetic restoration was completed by (a) converting mucosal-supported surgical guides into tooth- and mucosal-supported surgical guides, and (b) maintaining the vertical dimension through intraoral scanning.
Ⅱ. Case Description
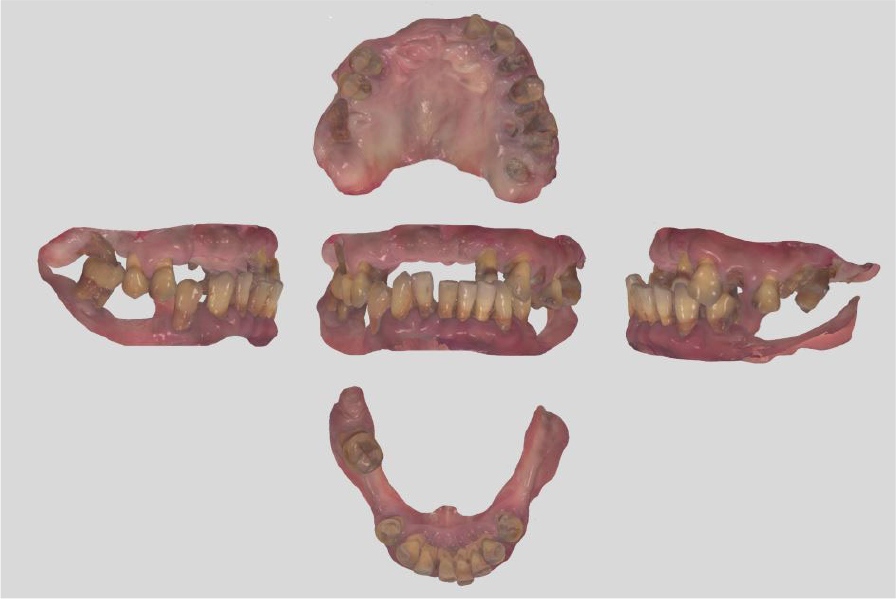
A 51-year-old male patient with no history of any serious disease visited a dentist with chief complaints of full-mouth implant treatment. Based on the initial clinical and radiographic examinations, the patient had severe periodontitis and was found to have multiple teeth with grade 3 mobility and heavy calculus deposition. In addition, many residual roots and teeth with advanced dental caries were observed (Fig. 1). A vertical stop was made in the left maxillary canine and left mandibular first premolar, and mastication was performed consistently on these teeth. No centric occlusion-centric relation (CO-CR) discrepancy was observed. The vertical dimension maintained by the left maxillary canine and left mandibular first premolar was judged to be satisfactory during the initial examination. In addition, full mouth scanning with an intraoral scanner (Trios 3; 3Shape, Copenhagen, Denmark) was conducted to use it as a reference point for the vertical dimension of the provisional prosthesis in future (Fig. 2).

As a result, the following treatment plan was established: (a) extraction of the remaining teeth in the maxilla and mandible, and (b) implant placement using implant surgical guides. Specifically, a total of 10 implants were planned to be placed at the maxillary lateral incisors, canines, first premolars, first molars, and second molars on both sides, whereas a total of eight implants were planned to be placed at the mandibular canines, first premolars, first molars, and second molars on both sides. Subsequently, it was decided to wait for healing after delivering provisional dentures to the upper and lower jaws. The final prosthesis was designed with three pieces, including one anterior segment and two posterior segments, on both upper and lower jaws.
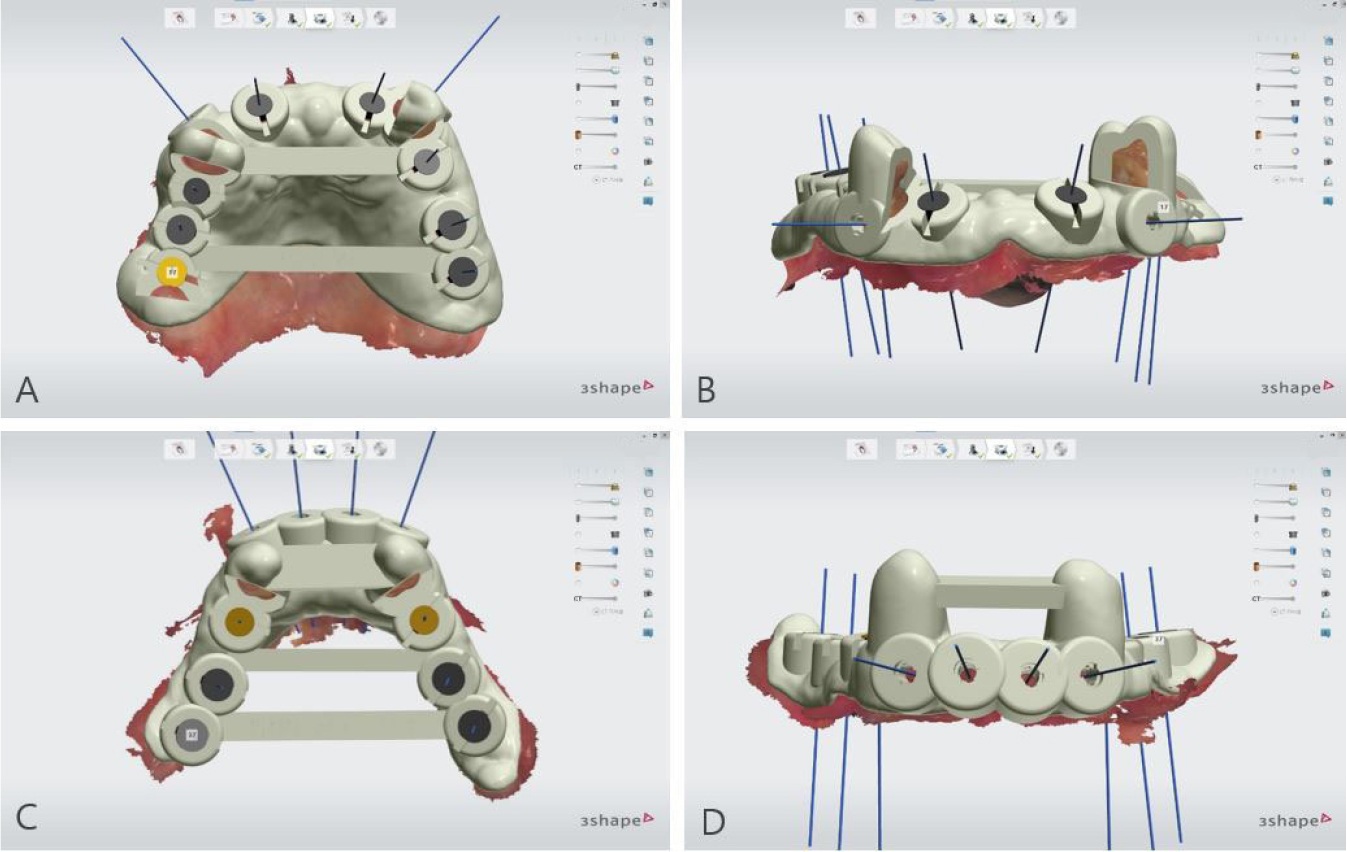
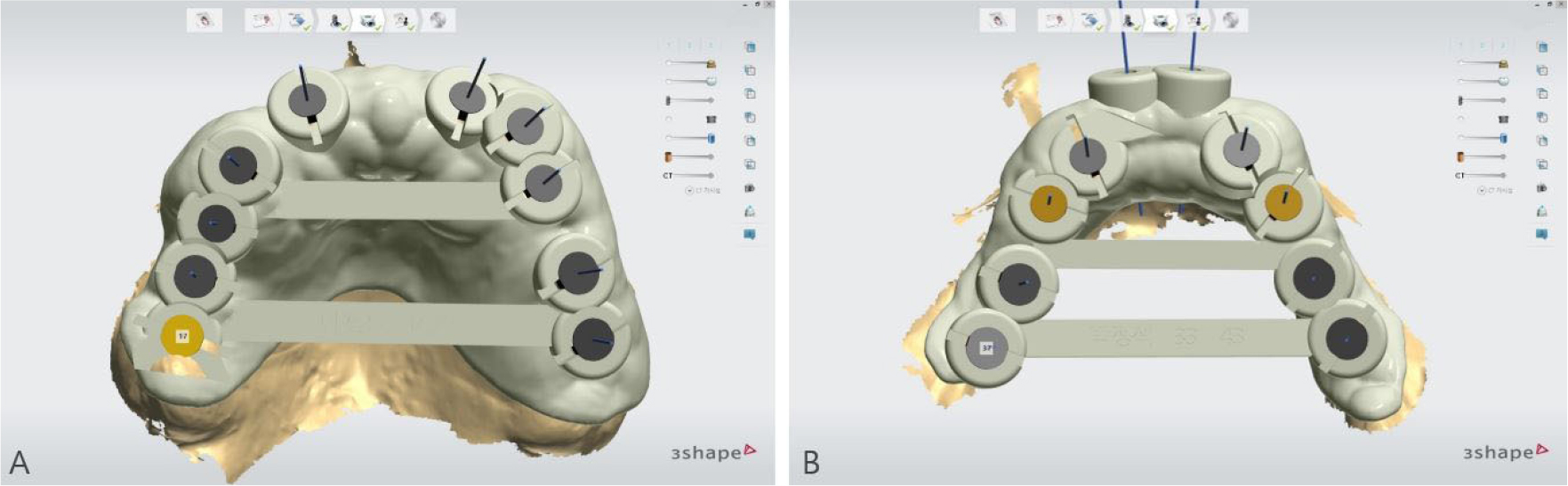
To overcome the limitations of the mucosal-supported surgical guides in the edentulous area, all teeth, except two teeth for each of the upper and lower jaws, were extracted (Fig. 3). Next, implant surgical guides were designed by superimposing the intraoral scanning data on the remaining teeth as shown in the CBCT images. The diagnostic model was designed by duplicating the initial vertical dimension by superimposing the upper and lower jaw scanning data obtained after extraction from the initial scanning data. In addition, the position of implantation was planned according to the simulated design (Figs. 4 and 5) using the implant planning software (Implant Studio; 3Shape). Subsequently, the second step of the implant surgical guide was designed after virtually extracting the remaining teeth from the scanned data, considering the location of the implants to be placed at the extraction site (Fig. 6). Finally, provisional dentures were designed to maintain the initial vertical dimension (Dental System; 3Shape) (Fig. 7).

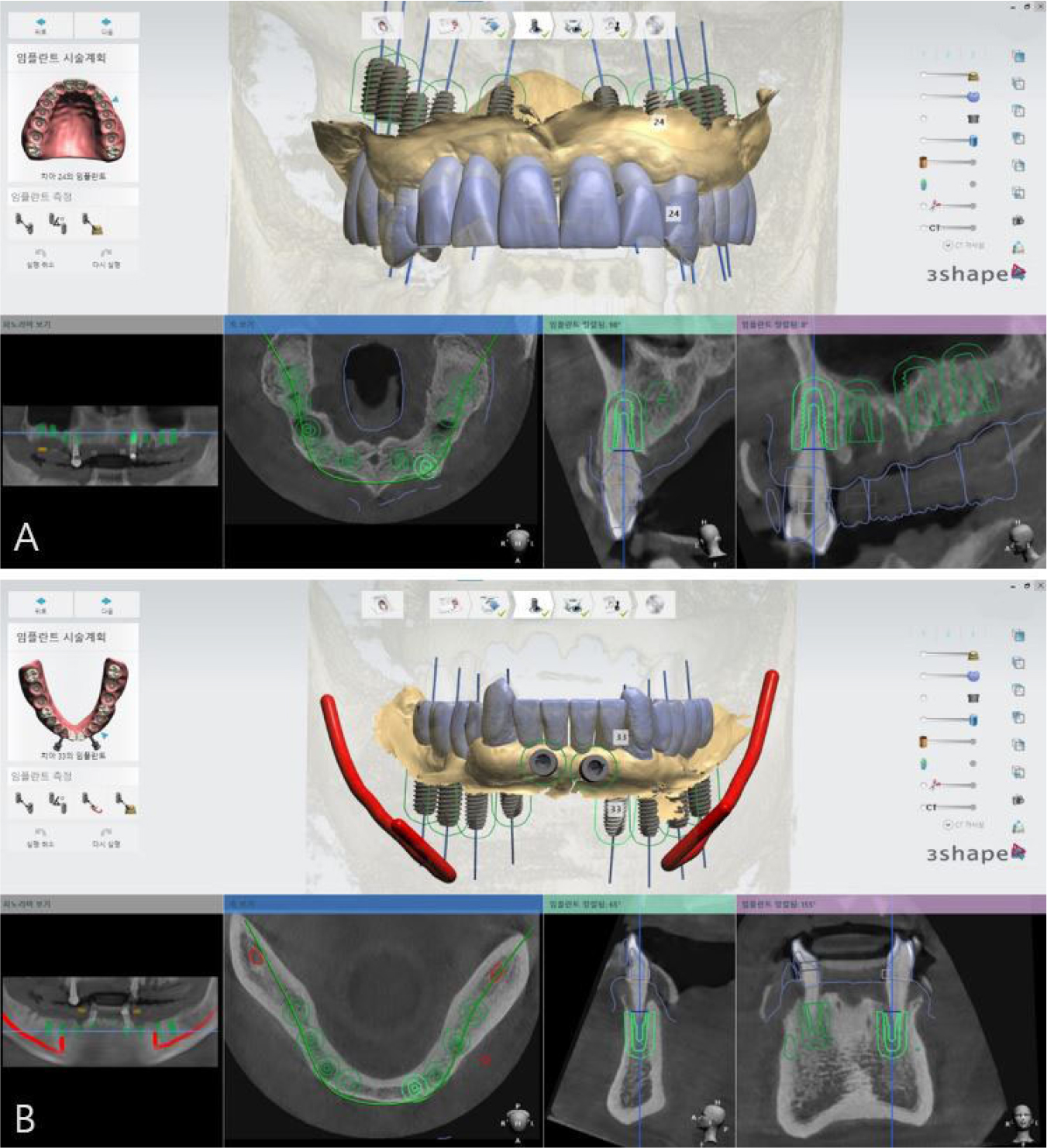

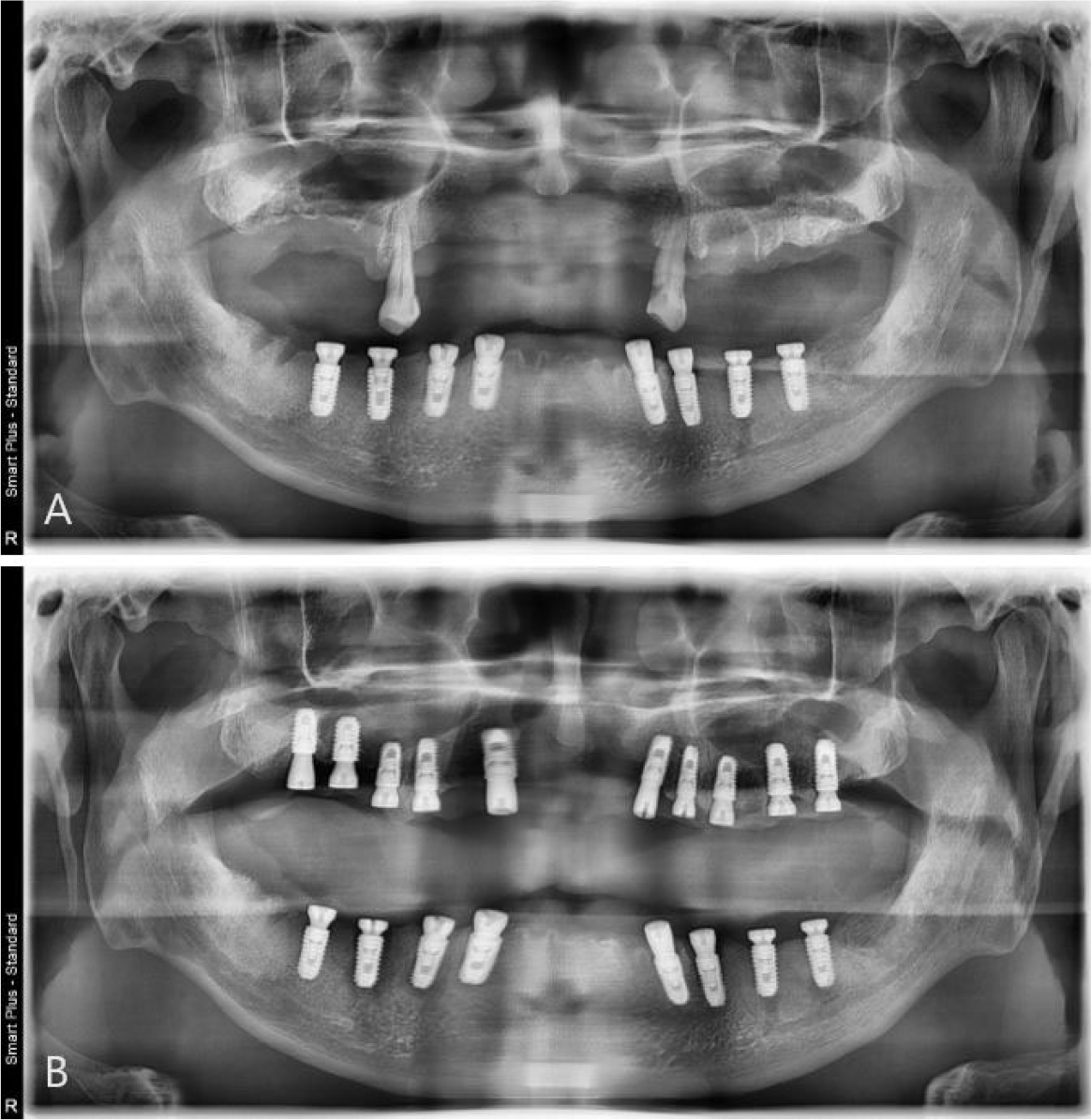
During implant surgery, an implant surgical guide was placed on both sides of the canines before extraction of the remaining mandibular canines. Up to this procedure, all implants required for the patient, except canines, were completed successfully (TS-III; OSSTEM, Seoul, Korea). After the extraction of canines on both sides, which were used as supporting components (i.e., anchor teeth) for the implant surgical guide, a second-step implant surgical guide was used to place the implants on the canine areas immediately (Fig. 8A). In addition, provisional dentures were delivered after the surgical procedures. Similar to the mandibular surgery, after the extraction of the supporting teeth for the implant surgical guide, a second-step implant surgical guide was used to place the implants immediately after the extraction (Fig. 8B). Finally, provisional dentures were stably delivered after the surgical procedures. After a 2-month osseointegration period, implant failure was observed in the right mandibular first molar, therefore, the fixture was removed and re-surgery was performed in that area. However, provisional fixed restorations were made using custom abutments and 3-piece polymethylmethacrylate (PMMA) for other successfully healed areas (Fig. 9).

Provisional fixed prostheses were fabricated without any changes in vertical dimensions. This is a result of superimposition of the intraoral scanning data using implant scan bodies with previous scanning data. Intraoral scanning of the entire jaw at the abutment level was performed after confirming osseointegration in the right mandibular first molar region. After scanning the upper and lower jaws at the abutment level, the same vertical dimension of the provisional prosthesis was applied to the final prosthesis: (a) the left inter-occlusal relationship was scanned with the 3-piece PMMA restoration inserted on the right side, and (b) the right bite was scanned with the PMMA restoration inserted on the left side.
The treatment was completed without any discomfort after delivery of the final prosthesis because the vertical dimension or occlusal surface shape of the prosthesis was exactly the same as that of the provisional prosthesis (Figs. 10 and 11).


Ⅲ. Discussion
There are not only many factors to be considered but also numerous opportunities for clinical errors in the treatment process in the case of full-mouth implant restoration followed by multiple teeth extraction. The most critical limitations are as follows: (a) it is difficult to secure retention and stability when using the implant surgical guides, and (b) some errors may occur when taking impressions and establishing an intermaxillary relationship. When using implant surgical guides, if there are no residual teeth, the retention and stability of the device are poor, and even if they are fixed using mini-screws (i.e., anchor pins), errors occurring during the process cannot be ignored. Moreover, it is difficult to perform saline irrigation to prevent bone heating owing to insufficient watering.
In these complex cases, a prosthetic-driven implant surgery is required for a long-term stability of hard and soft tissues around the implants.11 The implant surgery method used in this study reflected attempts to overcome these limitations: (1) it transitionally converts the mucosal-supported surgical guides into tooth- and mucosal-supported surgical guides to improve the retention and stability of the surgical guides, and (2) it implements a modeless maintenance of the patient’s vertical dimension in full mouth rehabilitation.
Surgical guide support can have a great effect on the retention and stability of the surgical guides.7 Mucosal-supported templates are affected by seating, depending on the thickness of the keratinized mucosa, local anesthesia, and the width of the alveolar bone.8,12 Therefore, in this case, a number of implants were accurately placed in the posterior regions using tooth-supported surgical guides with high stability by simply modifying the treatment process. For the teeth used as supporting parts, implants were inserted immediately after extraction through the second-step guide of the two-step surgical guide system, and a bone graft was performed. Through the two-step surgical guide system, it was possible to deliver more accurately prosthetically-driven top-down treatment plans established using CAD-CAM simulation in the patient's oral cavity. In addition, because the surgical guides were designed, the existing vertical dimensions could be copied continuously. However, this process cannot be implemented unless it is a digital workflow.
In the analog workflow, the most significant information is captured by impression-taking, occlusal relationship acquisition, and mounting. In addition, the vertical dimensions were recorded using various clinical methods. In this case, if the patient's current vertical dimension is to be maintained, various methods are required to confirm the adequacy of the vertical dimension in clinical trials. Moreover, numerous methods are used when transferring the exact vertical dimension; however, (a) this method cannot reproduce the patient's exact current state, and (b) the possibility of making errors can be increased through several steps. However, in the digital workflow, all steps from the initial state to the intermediate and final stages were recorded using intraoral scanning. Consequently, dentists and dental technicians can easily access the scanning data of the initial and interim stages of the entire process.13
Regardless of the type of prosthetic treatment, interim restoration is required to (a) maintain the patient’s comfort and aesthetics, and (b) evaluate the function and form of the prosthesis. In this case study, it is significant that by applying this digital workflow, the planned vertical dimension could be implemented from provisional dentures through provisional fixed prosthesis to the final implant prosthesis without any discomfort to the patient.
Ⅳ. Conclusion
This study aimed to explore the (a) tooth-mucosal supported guide surgery by developing a two-step surgical guide system in a case requiring full-mouth implant restoration after full extraction, and (b) rehabilitation with a modeless implant restoration by reproducing the vertical dimension through intraoral scanning. This study suggests that the accuracy and convenience of the treatment can be improved by increasing the stability of the implant surgical guides through a two-step surgical guide system using a digital workflow.
