

Ⅰ. Introduction
This case report describes the orthodontic forced eruption for a permanent canine with a subgingival recurrent dental caries. The various techniques were proposed for this situation.1 Various treatment options are illustrated in Figs. 1 and 2. The patient’s economic condition was not enough for implant supported prosthesis, preserving root was chosen. Bone reduction is needed for crown lengthening procedure. Therefore, crown lengthening procedure is not desirable for implantation for future condition (i.e. after extraction of the crown lengthened tooth). Thus, orthodontic forced eruption was chosen.
Clinical value of orthodontic forced eruption has been supported by many reports.2,3,4,5,6,7,8,9,10,11,12,13
Forced eruption of the root affects the periodontal fibers. This leads a coronal shift of the marginal gingiva and the supporting bone.2 The treatment goal is to expose subgingival caries and maintain biologic width to allow restoration without causing periodontal complications.14,15
Ⅱ. Case Report
A 69-year-old female patient presented for periodic check. (Fig. 3). The results of the extraoral evaluation were unremarkable.

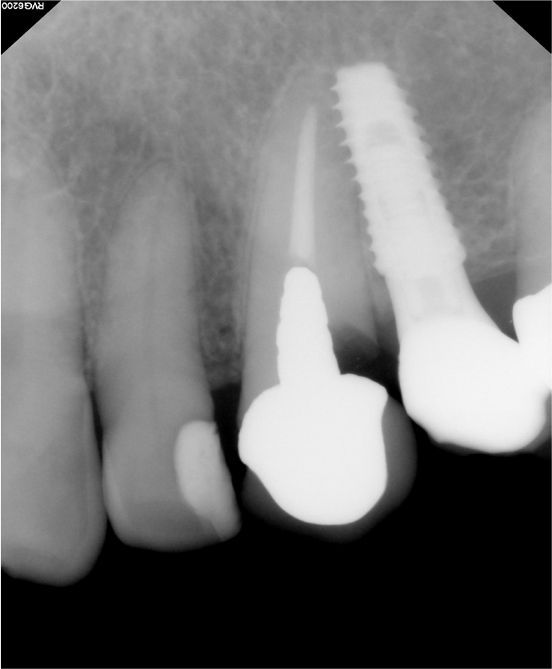
The intraoral evaluation revealed recurrent caries of maxillary left canine in the existing prosthesis. The tooth had extensive carious lesion. A periapical radiograph of the maxillary left canine (Fig. 4) showed recurrent caries under the fixed dental prosthesis.
After dental prophylaxis and oral hygiene education, the fixed dental prosthesis and cast custom post were removed. (Fig 5). For forced eruption, the hook was inserted into the root of canine and cemented with Zinc Phosphate Cement (Elite cement, GC, Japan) (Fig 6).


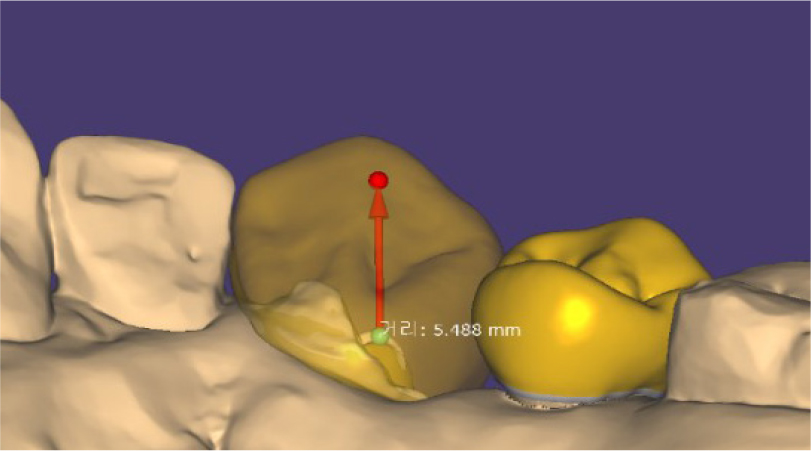
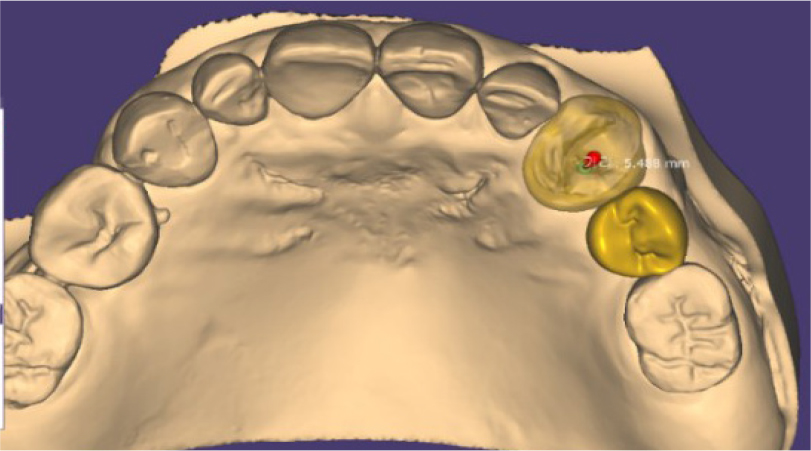
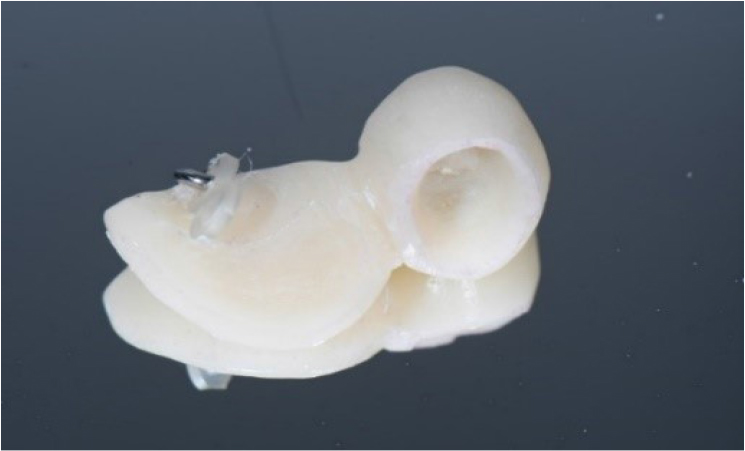
Differently from other cases, the forced eruption was planned with CAD program (Exocad, Align Technology, CA) (Figs. 7 and 8). The implant supported appliance for forced eruption was designed as following. The direction of force applied to the root was designed corresponding with tooth axis. The distance between the root and the appliance was designed as 5.5 mm. Because of the ferrule effect and biological width, the amount of eruption of 4 mm was needed. Considering orthodontic relapse, the overcorrection was planned as 5.5 mm. And corresponding prosthesis was designed. The appliance was fabricated with 3D printing resin (Temporary resin, Dentis, Korea) and 3D printer (Zenith, Dentis, Korea). The hook was attached by 3D printing resin (Temporary resin, Dentis, Korea). And the appliance was cemented using RMGI cement (Fujicem, GC, Japan). Between the tooth and appliance, the power chain was engaged. As the forced eruption appliance is supported by the adjacent implant, the orthodontic bracket and wire were not needed (Figs. 9 and 10). The adjacent implant was served as an absolute anchor.

Oral hygiene instructions were provided about the use of an interproximal brush in this area. Figs 10 and 11 show the delivery of forced eruption appliance.
After 2 months, the extrusive movement was completed. Figs. 12 and 13 show the post-operative state of the dentition when forced eruption was completed. After 6 weeks of period, the reorganization of the periodontal tissue around the root was successfully achieved (Fig. 14).




Ⅲ. Discussion
When orthodontic forced eruption was performed, plaque retention could be increased. Thus, oral hygiene plays a key role in the orthodontic forced eruption.1 Despite of tooth brushing instruction, the additional dental caries was generated compared with initial state. A possibility can be proposed that the barrier around the elastic and appliance could make the oral hygiene poor. This appliance has a buccal wall for the esthetics, so the plaque could not be removed easily. To improve this, the buccal wall could be removed to get a good oral hygiene.
The amount of extrusion was calculated by considering the “biologic width.”14 It was approximately 4 mm. After the extrusion, the tooth still retained a crown-root ratio of approximately 1:1. It is favorable for maintaining periodontal support. Compromised crown to root ratio of 1:1 did not have the negative effect to tooth mobility due to interposition of connective tissue.
After 6 weeks period, the height and width was stabilized. And cast post and PFZ crown was delivered.
Different from the conventional method using orthodontic bracket and wire, this technique used implant supported fixed dental prosthesis as absolute anchor. Without the need of orthodontic bracket and wire esthetics and comfortable processes could be achieved by utilizing an implant as an absolute anchor. CAD program enables the clinician to manipulate the angle and direction of forced eruption in the most appropriate way.
