

Ⅰ. Introduction
Ⅱ. Case Report
1. Case Presentation
2. Surgical and Orthodontic Procedures
3. Prosthetic Procedures
Ⅲ. Discussion
Ⅳ. Conclusion
Ⅰ. Introduction
Implant rehabilitation in the esthetic zone is often challenging because successful treatment requires not only adequate alveolar bone volume but also sufficient restorative space and proper implant positioning.1 Following tooth loss, alveolar ridge resorption may further complicate implant placement, particularly in cases associated with trauma, infection, or pre-existing bone defects.2,3 Furthermore, anterior crowding and malalignment may limit the mesiodistal space available for implant restoration and compromise the esthetic and functional outcomes of prosthetically driven treatment.
Although alveolar ridge preservation (ARP) has been proposed to reduce post-extraction ridge resorption and maintain ridge architecture for future implant placement, severe defects frequently require additional site development procedures.4,5 Furthermore, orthodontic treatment may be necessary to establish appropriate space and alignment before implant placement, as osseointegrated implants cannot be repositioned orthodontically after surgery.6 Therefore, treatment sequencing should be a critical consideration when both space deficiency and alveolar defects coexist.
This clinical report describes the staged interdisciplinary treatment of a 20-year-old female presenting with a crown-to-root fracture of the maxillary right central incisor accompanied by severe alveolar bone loss and inadequate restorative space due to anterior crowding. A sequential treatment approach involving ARP, orthodontic space creation, block bone grafting, implant placement, and prosthetic rehabilitation was used to achieve favorable esthetic and functional outcomes.
Ⅱ. Case Report
1. Case Presentation
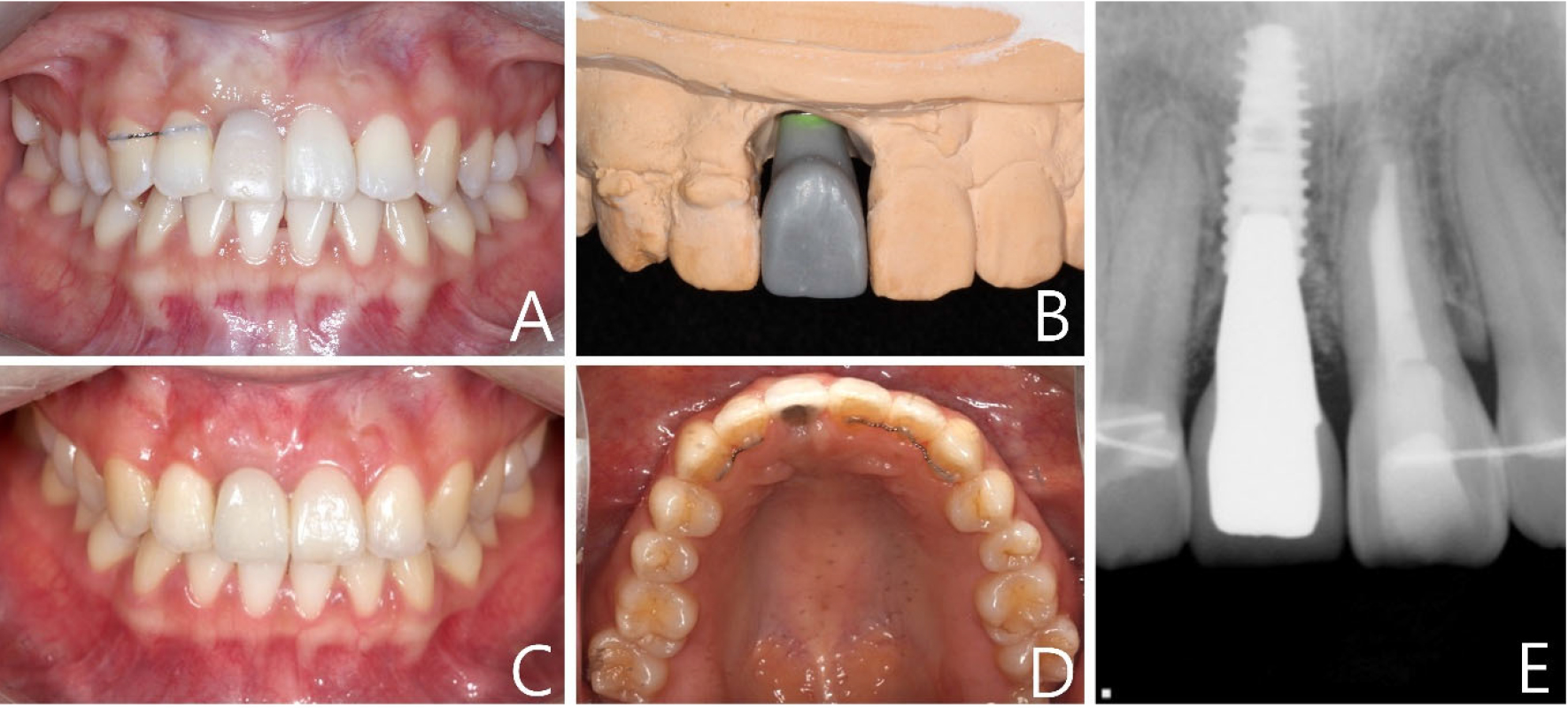
A 20-year-old female was referred from the Department of Endodontics with complaints of discomfort in the right maxillary central incisor following trauma that occurred 12 years earlier. Clinical examination revealed a crown-to-root fracture, Class II mobility, gingival swelling, and pus discharge associated with the right maxillary central incisor (Fig. 1). Radiographic evaluation revealed previous root canal treatment of both maxillary central incisors, whereas cone-beam computed tomography (CBCT) revealed severe alveolar bone loss involving both the labial and palatal walls, leaving only one-third of the apical root supported by the remaining alveolar bone.
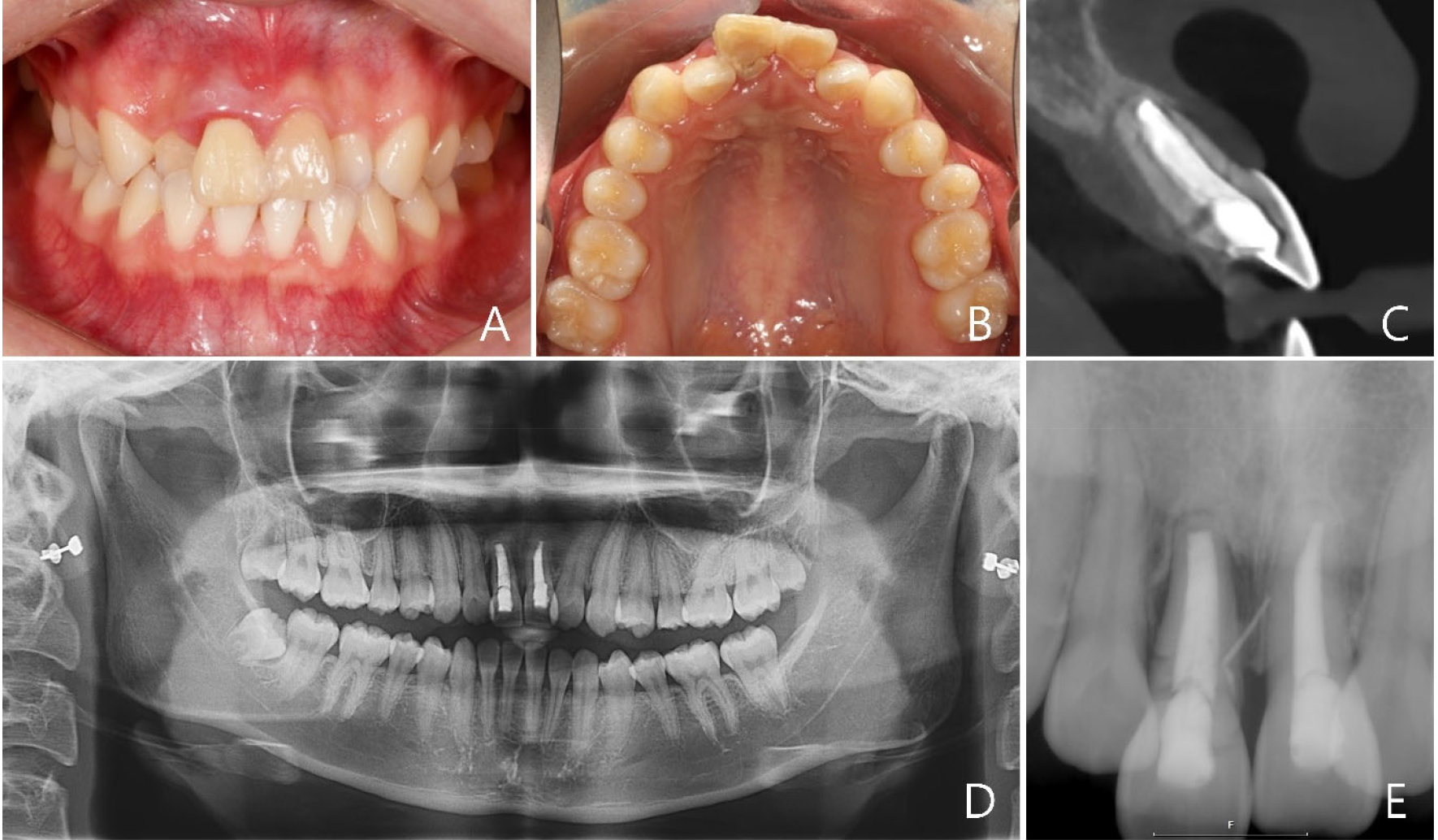
Fig. 1.
Clinical and radiographic findings at the initial visit. (A) Frontal intraoral view showing anterior crowding and limited restorative space, (B) occlusal view of the maxillary arch, (C) sagittal CBCT image demonstrating severe alveolar bone loss associated with the right maxillary central incisor, (D) panoramic radiograph, and (E) periapical radiograph.
Besides the compromised hard tissue condition, crowding and malalignment of the maxillary anterior dentition were observed, with both lateral incisors exhibiting crossbites. Orthodontic evaluation demonstrated 5.0 mm of available restorative space at the right maxillary central incisor. Maxillary arch space analysis performed between the right and left second premolars revealed a 1.2-mm arch length deficiency associated with anterior crowding. These findings indicate that orthodontic treatment is necessary to establish adequate restorative space and favorable tooth alignment before implant placement.
The combination of severe alveolar bone loss, limited restorative space, and unfavorable tooth alignment precludes prosthetically driven implant placement. Consequently, immediate implant placement was not considered appropriate because adequate three-dimensional implant positioning and predictable development of an optimal emergence profile could not be achieved under the existing hard and soft tissue conditions.
Although a fixed dental prosthesis was considered as an alternative treatment option, implant rehabilitation was ultimately selected because of the patient’s young age, treatment preference, and desire to preserve the adjacent teeth. Therefore, a staged interdisciplinary treatment plan was established to address alveolar defect and space deficiency before implant rehabilitation.
2. Surgical and Orthodontic Procedures
Under local anesthesia with lidocaine containing 1:100,000 epinephrine, the right maxillary central incisor was extracted. To minimize post-extraction ridge collapse and preserve the extraction site for future implant rehabilitation, ARP was carried out using the ice cream cone technique with deproteinized bovine bone mineral (Bio-Oss; Geistlich Biomaterials, Wolhusen, Switzerland) and a resorbable collagen membrane (Bio-Gide; Geistlich Biomaterials) (Fig. 2).7 An interim prosthesis was delivered on the day of extraction.
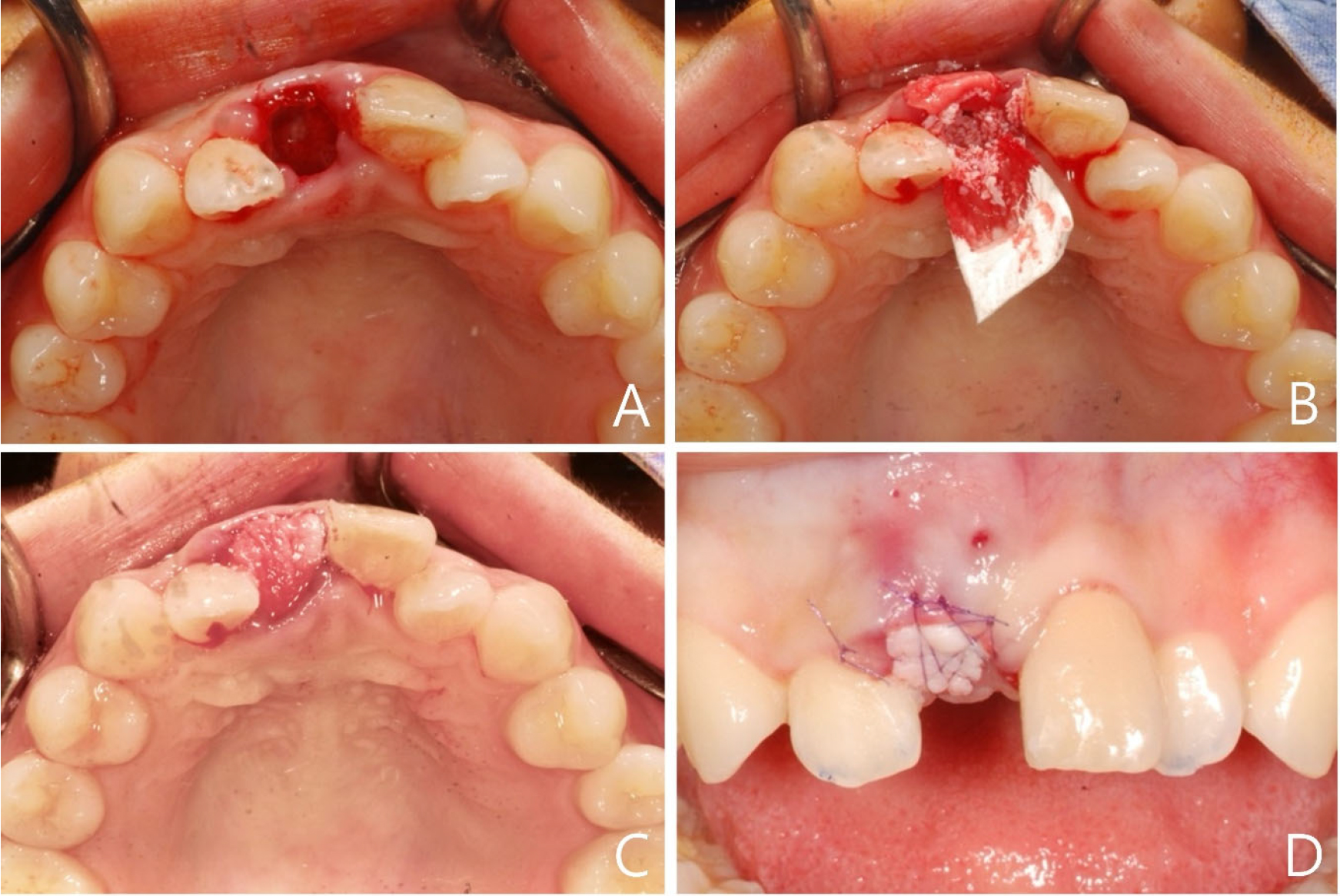
Fig. 2.
Extraction and alveolar ridge preservation (ARP) procedures. (A) Occlusal view after extraction of the right maxillary central incisor, (B) ARP using deproteinized bovine bone mineral and a resorbable collagen membrane with the ice cream cone technique, (C) extraction socket covered with a resorbable collagen membrane, (D) clinical view after suturing and delivery of the provisional restoration.
Because restorative space deficiency and anterior crowding were considered major limitations of implant rehabilitation, orthodontic treatment was initiated during the healing period to establish adequate alignment and restorative space. Composite bite ramps were placed on both mandibular molars, and the maxillary anterior teeth were aligned using interproximal reduction and direct bonding. After 1.5 years of orthodontic treatment, the patient was referred back with improved alignment, and the available restorative space for the right maxillary central incisor had increased to 8.2 mm.
CBCT demonstrated an hourglass-shaped ridge morphology, indicating preservation of the vertical ridge contour but a persistent horizontal deficiency that remained insufficient for implant placement (Fig. 3). Although simultaneous bone block grafting was not feasible at the time of extraction, the preserved vertical ridge provided a stable recipient site for secondary ridge augmentation. Therefore, secondary site development was performed using an allogeneic block bone graft (ICB; Rocky Mountain, Denver, USA), which was adapted to the residual ridge and stabilized with two titanium fixation screws (1.6 × 10 mm).
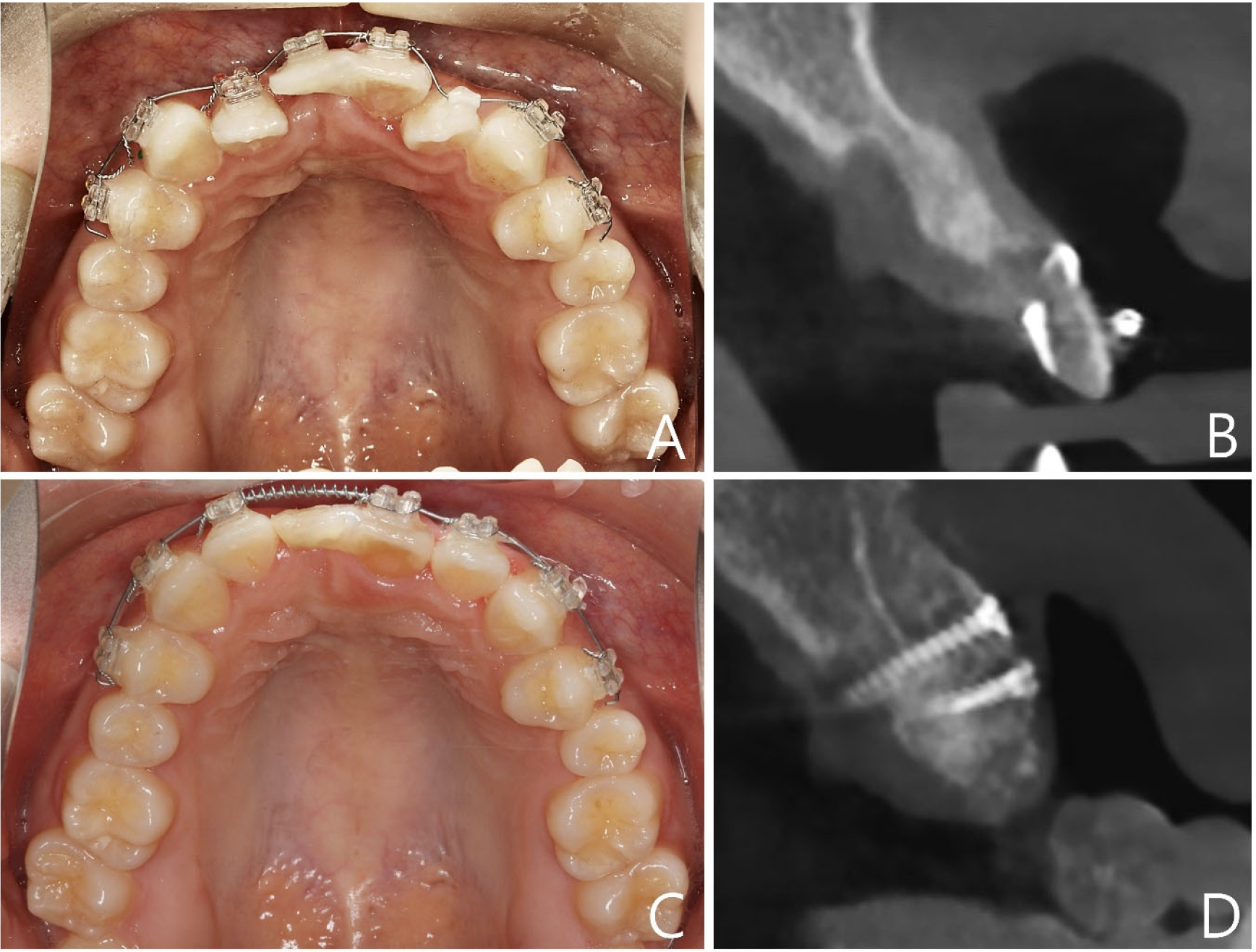
Fig. 3.
Orthodontic space creation and changes in alveolar ridge morphology. (A) Occlusal view before orthodontic treatment showing anterior crowding and limited restorative space, (B) sagittal CBCT image after alveolar ridge preservation (ARP) demonstrating preservation of the vertical ridge contour with insufficient buccolingual bone volume, (C) occlusal view after orthodontic treatment showing improved alignment and restorative space, (D) sagittal CBCT image obtained 6 months after allogeneic block bone grafting demonstrating increased bone volume for implant placement.
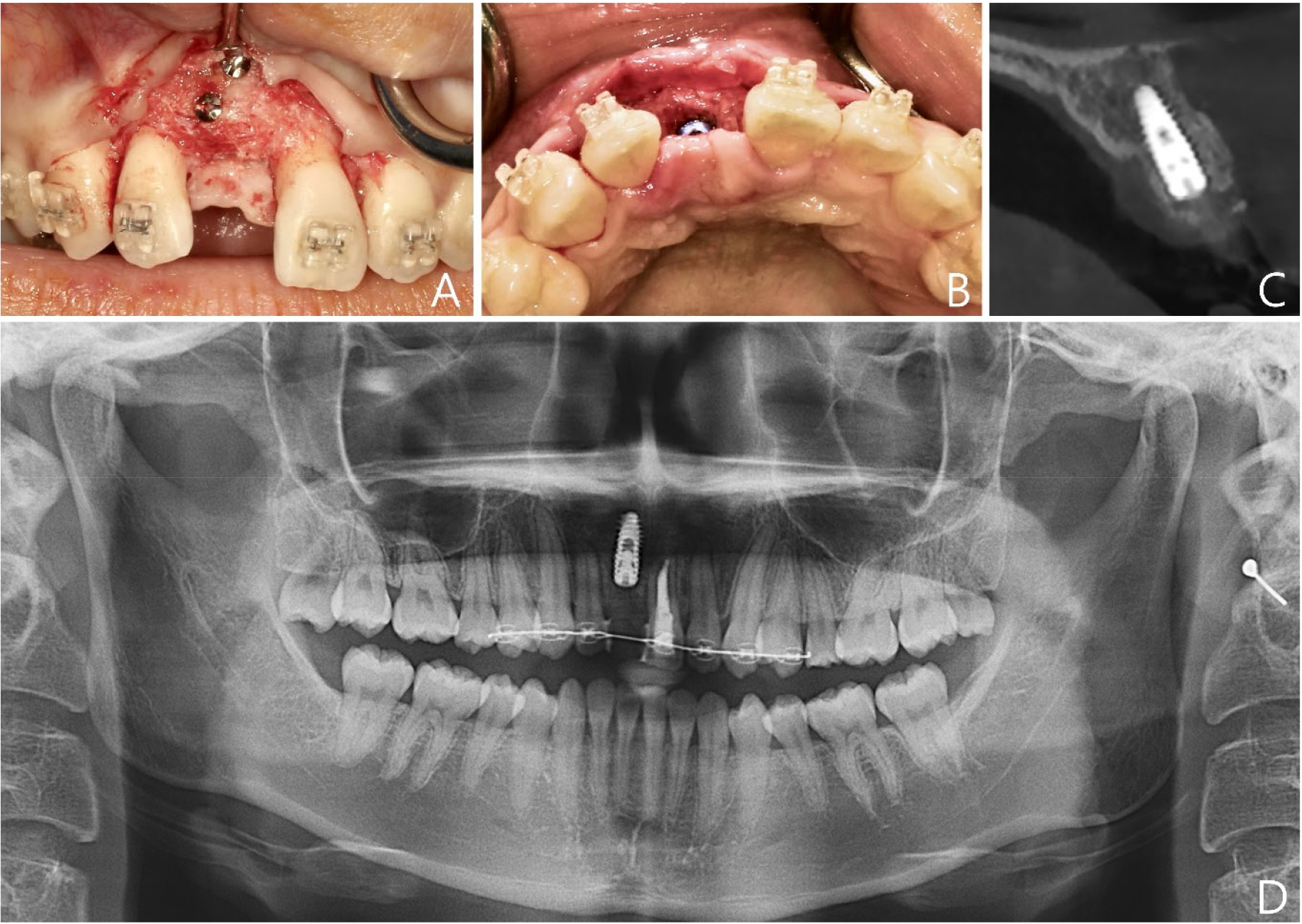
Six months after block bone grafting, CBCT confirmed an adequate bone volume for implant placement. Virtual implant planning was performed using an implant planning software (R2GATE; Megagen, Daegu, South Korea) based on the reconstructed ridge contour, available bone volume, digital diagnostic wax-up, and the planned position of the adjacent teeth. A bone-level implant (IU; Warentec, Seongnam, South Korea; diameter 4.0 mm, length 11.5 mm) was placed using a digitally fabricated surgical guide, and the fixation screws were removed simultaneously (Fig. 4). No additional bone augmentation was required at the time of implant placement, and primary implant stability exceeding 45 Ncm was achieved.
3. Prosthetic Procedures
Following successful osseointegration, prosthetic rehabilitation was initiated, with an emphasis on achieving favorable esthetic integration and an appropriate emergence profile. A provisional restoration was fabricated using a polymethyl methacrylate (PMMA) crown according to the three-zone concept. The provisional restoration featured a convex esthetic (E) zone to support the cervical contour, a straight crestal (C) zone to preserve the peri-implant connective tissue, and a smooth bounded (B) zone to facilitate the gradual transition of the emergence profile.8 Following digital scanning with an intraoral scanner (Trios 3; 3Shape, Copenhagen, Denmark), the provisional restoration was delivered (Fig. 5) and used to support peri-implant soft tissue contouring and establishment of an appropriate emergence profile.
After stabilization of the peri-implant soft tissue architecture, a customized impression coping was fabricated using autopolymerizing acrylic resin (Pattern Resin LS; GC Corporation, Tokyo, Japan) to replicate the subgingival contour established by the provisional restoration. Final impression and shade matching were performed, and a screw-retained porcelain-fused-to-gold crown supported by a 1-piece castable abutment was delivered after occlusal adjustment (Fig. 5).
Follow-up examinations for up to 1.5 years demonstrated stable peri-implant marginal bone levels, satisfactory function, and harmonious esthetic integration. Periapical radiographs showed no significant changes in marginal bone levels compared with those obtained immediately after implant placement. Complete interdental papillary filling was also achieved, and no biological or prosthetic complications were observed during follow-up. The patient also reported satisfaction with both the esthetic appearance and functional outcome of the definitive restoration.
Ⅲ. Discussion
Implant rehabilitation of a maxillary central incisor is particularly challenging when severe alveolar bone loss is accompanied by crowding and inadequate restorative space. In the present case, immediate implant placement was not considered appropriate because both the severe alveolar defect and unfavorable tooth alignment compromised the possibility of prosthetically driven implant positioning. Successful implant rehabilitation in the esthetic zone requires not only sufficient bone volume but also proper mesiodistal space, implant angulation, and emergence profile.8
An important aspect of the present case was the role of orthodontic treatment in creating an appropriate restorative environment before implant placement. Because osseointegrated implants cannot be orthodontically repositioned after placement, orthodontic correction before implant surgery may be essential to establish adequate space and harmonious alignment for long-term restorative success.6 In the present case, orthodontic space creation served as a prerequisite for prosthetically driven implant rehabilitation rather than simply correcting tooth alignment.
Furthermore, ARP did not provide sufficient bone volume for direct implant placement even though it was performed immediately after extraction. Nevertheless, it contributed to the preservation of the ridge contour and facilitated secondary site development. The maintained vertical ridge morphology provided a stable foundation for subsequent block bone grafting, thereby reducing the complexity of subsequent augmentation procedures. Therefore, this case suggests that ARP can serve as a preparatory site-preservation strategy for severely compromised extraction sockets.
The present case highlights the importance of a staged interdisciplinary treatment involving endodontic, orthodontic, surgical, and prosthetic considerations. Within the limitations of a single clinical report, a sequential treatment approach involving orthodontic space creation followed by secondary site development may facilitate prosthetically driven implant rehabilitation for maxillary central incisor defects associated with crowding and severe alveolar bone loss.
Ⅳ. Conclusion
This clinical report demonstrates that a staged interdisciplinary treatment can facilitate implant rehabilitation in maxillary central incisor defects accompanied by crowding and severe alveolar bone loss. In complex esthetic cases where the restorative space and bone volume are compromised, sequential treatment involving orthodontic space creation and secondary site development may contribute to controlled functional and esthetic outcomes.
