

Ⅰ. Introduction
Ⅱ. Materials and Methods
1. Ethical approval
2. Participants and data collection
3. Survey method
4. Statistical analysis
Ⅲ. Results
1. Respondent characteristics and implant practice patterns
2. Experience with unidentified implant systems and information-seeking behavior
3. Awareness and use of identification services and willingness to adopt AI tools
Ⅳ. Discussion
Ⅴ. Conclusion
Ⅰ. Introduction
Dental implant therapy has become one of the fastest growing areas in dentistry over the past several decades.1 In South Korea, the commercialization of domestic implant systems, rapid technological advancements, and introduction of partial National Health Insurance coverage in 2014 have substantially increased the accessibility of implant treatment. As of 2019, approximately 600,000 individuals receive dental implants annually, and they have become a common treatment option for middle-aged and older adults.2 More than ten million implants are estimated to have been placed cumulatively in Korea, and given the rapidly aging population, the demand for implant therapy is expected to continue to increase.3
In addition to the increasing number of implant placements, the importance of follow-up management is also increasing.4 The average replacement interval for implant-supported prostheses is approximately 7–8 years, and complications such as peri-implantitis, prosthesis fractures, and screw loosening have been reported.5 However, the Korean implant market comprises more than 300 product types from numerous implant systems, and patient dental records are distributed across individual clinics. Consequently, both patients and clinicians frequently experience difficulty identifying the previously placed implant system. In one survey, 97.1% of dentists reported encountering patients whose implant types could not be identified during treatment, and unnecessary implant removal procedures were reported due to such uncertainty.6
To address these issues, the Korean Academy of Oral and Maxillofacial Implantology (KAOMI) launched an “implant identification service” in September 2018.7 Through this campaign, participating dentists could send radiographic images via mobile messaging and designated KAOMI reviewers could provide a presumed implant system and model based on visual inspection. However, the campaign had notable limitations: the average response rate was approximately 35%, the average response time exceeded five hours, and low-quality images, such as partial captures or photographs taken using mobile phones, often hindered accurate identification. Recently, artificial intelligence (AI)-based implant identification technologies have emerged with potential improvements in efficiency and accuracy.8 Nevertheless, there is a lack of quantitative evidence regarding the challenges dentists face in clinical practice, the frequency of insufficient implant information, and the level of acceptance of such AI-based systems.
This study investigated the implant practice patterns, experiences related to unknown implant types, information-seeking behaviors, criteria for selecting implant systems, and acceptance of AI-based implant identification services among practicing dentists in Korea. The findings aimed to provide empirical data to support the clinical need for implant information management and inform future efforts toward standardizing implant information systems and AI-driven identification tools.
Ⅱ. Materials and Methods
1. Ethical approval
This study was approved by the Institutional Review Board of the Yonsei University Dental Hospital (IRB No. 2-2021-0097). Before participating, all participants were provided with information on the purpose and procedures of the study. For the online survey, participants were required to check an electronic consent box (“I agree to participate in this study”) before accessing the questionnaire. All responses were collected anonymously, and no personally identifiable information (e.g., name, resident registration number, contact details, or IP address) was obtained.
2. Participants and data collection
A cross-sectional online survey was conducted between October 2021 and May 2022. Eligible participants were licensed dentists in clinical practice in South Korea at the time of the survey. Convenience sampling was employed due to logistical constraints. The survey link was primarily distributed through the KAOMI, and some participants were informed offline through academic or institutional networks before completing the online survey. Individuals who were unable to read or understand the questionnaire (e.g., non-Korean speakers, low literacy) or who did not agree to participate were excluded from the analysis. Five hundred dentists provided consent and completed a self-administered online questionnaire.
3. Survey method
The questionnaire consisted of three major sections: (1) implant practice patterns; (2) experiences and perceptions related to implant information; and (3) general characteristics of the participants. The survey included 25 items addressing the number of implants placed, number of implant patients, proportion of National Health Insurance implants, experience with unknown implant systems, and methods used to obtain implant information. Most items were structured as multiple-choice questions. The awareness and prior use of manual implant identification services were assessed using two separate questionnaire items. The wording of these items and other key outcome questions are provided in Supplementary Table S1 to allow readers to evaluate the structure of the survey and interpret the responses.
4. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 28.0; IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the data. For each survey item, frequencies and percentages were calculated to examine the response distributions. Because the study was designed as an exploratory survey to describe dentists’ experiences and perceptions, inferential statistical analyses were not performed.
Ⅲ. Results
1. Respondent characteristics and implant practice patterns
Five hundred dentists completed the survey. The sociodemographic characteristics are summarized in Table 1. Most respondents were male (74.8%) and the largest age group was dentists in their 40s (53.4%), followed by those aged ≤ 30 years (34.4%). Regarding implant surgery experience, 40.6% had ≥10 years of experience and 26.4% had 5–10 years of experience. Private practitioners accounted for 67.6% of the respondents, followed by associate dentists (20.4%).
Table 1.
Sociodemographic characteristics of survey respondents (n = 500)
Note. Thirteen respondents held multiple specialties, including advanced general dentistry, oral and maxillofacial surgery (n = 5), pediatric dentistry (n = 1), orthodontics (n = 2), prosthodontics (n = 4), and periodontology (n = 1). These respondents were excluded from the total number of advanced general dentistry specialists (n = 248).
The clinical characteristics related to implant practice are presented in Table 2. Among the respondents, 88.2% reported that they currently perform implant surgery. In the previous month, 29.5% placed 10–19 implants, 22.0% placed 5–9 implants, and 20.0% placed ≥30 implants. Monthly implant patient volume showed a similar pattern, with 28.6% treating 10–19 patients and 24.5% treating ≥30 patients. The proportion of National Health Insurance implants was < 20% among 46.9% of the respondents and 20–39% among 29.7%. Regarding the implant system used, 23.4% reported using one system, whereas 66.2% used two to three systems.
Table 2.
Clinical characteristics of implant practice among dentists
2. Experience with unidentified implant systems and information-seeking behavior
Among the respondents who answered this item, 96.4% (425/441) reported having encountered clinical situations in which the type of implant fixture placed in the patient could not be identified (Fig. 1). Among the respondents who reported encountering unidentified implant systems (n = 425), 53.4% (227/425) asked patients to contact their previous dentist, 17.4% (74/425) consulted a colleague, and 15.5% (66/425) contacted the implant company. A manual identification service, in which experts reviewed the submitted radiographs, was used by 12.7% of the respondents (54/425). Other approaches were reported in 0.9% (4/425) of the cases.
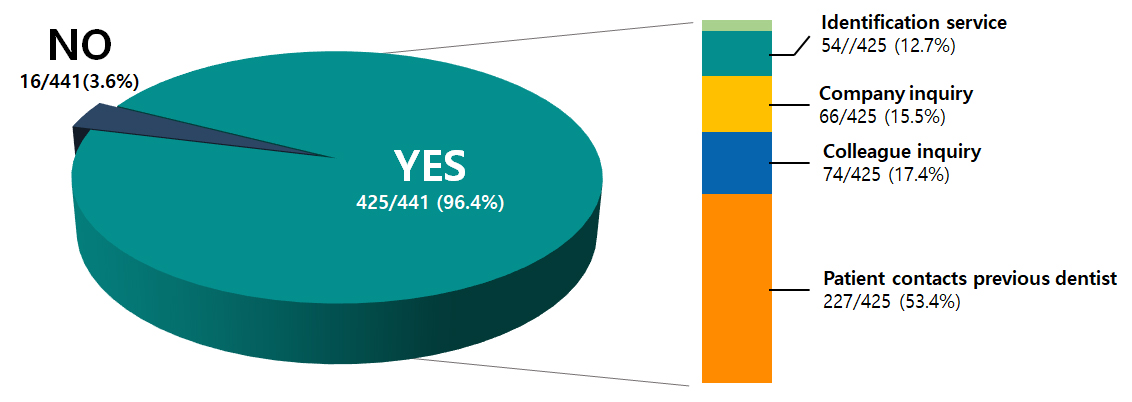
Fig. 1.
Among respondents who answered currently perform implant surgery, proportion of dentists who have encountered cases in which the type of implant fixture could not be identified during patient care (left), and methods used to obtain implant information in such cases (right). Categories include: Patient contacts previous dentist, Colleague inquiry, Company inquiry, Identification service, and Other.
3. Awareness and use of identification services and willingness to adopt AI tools
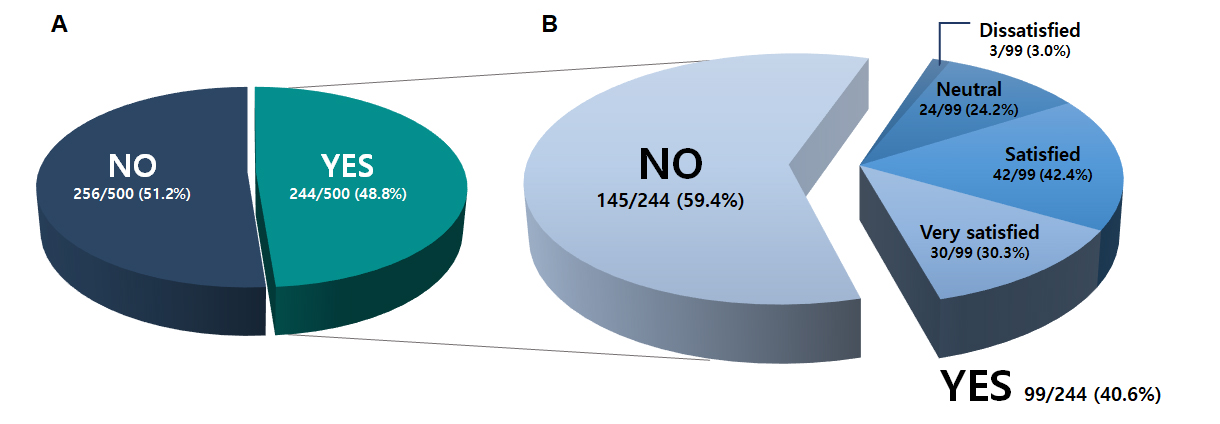
Among all respondents, 48.8% (244/500) were aware of the existing manual implant identification service provided through expert review, whereas 51.2% (256/500) were not. Among those who were aware of the service, 40.6% (99/244) reported having used it, whereas 59.4% (145/244) had not. Among users who provided satisfaction ratings (n = 99), 42.4% were satisfied, 30.3% were very satisfied, 24.2% were neutral, and 3.0% were dissatisfied (Fig. 2).
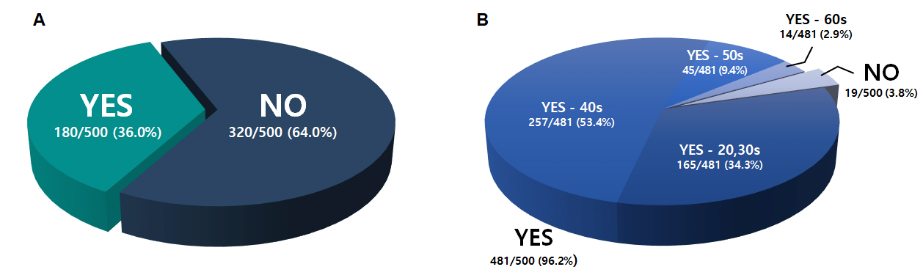
Regarding their ability to visually identify implant systems on radiographs, 64.0% (320/500) were unable to distinguish between implant systems, whereas 36.0% (180/500) reported that they could. When asked about adopting an AI-based implant identification tool, 96.2% (481/500) expressed willingness to use the system. Among those who answered “Yes,” respondents in their 40s comprised the largest subgroup (53.4%), followed by those in their 20s to 30s (34.3%), 50s (9.4%), and 60s (2.9%) (Fig. 3).
Ⅳ. Discussion
This study examined dentists’ implant practice patterns, experience with unknown implant systems, information-seeking behaviors, awareness and use of manual identification services, and willingness to adopt AI-based identification tools. These findings should be interpreted as reflecting perceptions within a clinical cohort of dentists actively engaged in implant practice rather than providing population-level prevalence estimates.
The difficulty of identifying implant systems placed by other providers has long been recognized in the literature.9,10 With the global expansion of implant therapy, the number of implant systems, abutment designs, and connection types has grown substantially, creating challenges for clinicians who must maintain or restore implants placed elsewhere. Previous studies have shown that radiographic recognition of implant systems is highly operator dependent and often inaccurate, especially when hundreds of similar systems are used.11,12 These challenges are amplified in regions such as South Korea, where an exceptionally diverse implant market exists, and treatment records are often unavailable to the receiving clinician. Our finding that 96.4% of dentists encountered unidentified implant systems is consistent with earlier reports showing high rates of implant identification uncertainty among general practitioners.
To compensate for missing implant information, respondents relied primarily on indirect communication pathways, most commonly asking patients to contact their previous dentist, followed by consultation with colleagues or manufacturers. Similar patterns have been reported internationally.13 Although several web-based resources have been developed to assist clinicians, their practical utility remains unclear. “WhatImplantIsThat?” is a widely used international platform that aggregates radiographic images submitted by clinicians; however, its effectiveness is limited by variable image quality, the absence of standardized metadata, and the need for users to visually search hundreds of implant designs manually.14 These limitations parallel the findings of the present study. Just over one-third of the respondents were aware of manual or expert-based identification services and an equally small proportion had ever used them. Nonetheless, user satisfaction among those who had used such services was high, suggesting that structured implant identification support is valued, but remains underutilized due to issues of accessibility, workflow inefficiency, and inconsistent diagnostic reliability, rather than a lack of perceived usefulness.
The finding that most dentists reported difficulty identifying implant systems on radiographs underscores the inherent limitations of conventional imaging modalities.15 Panoramic radiography, although widely used, often lacks sufficient resolution to distinguish fine design features such as thread geometry, platform switching, or microgrooves, and periapical radiographs may similarly fail to differentiate among implant systems when the macro-design characteristics overlap. These limitations reflect the broader challenges described in recent AI implant identification research, which show that even trained dental professionals exhibit markedly low diagnostic accuracy when visually classifying implant systems, particularly when images are of low-quality or distorted.16
With the rapid advancement of AI in radiographic interpretation, several studies have explored AI-based models for dental implant identification. Deep learning algorithms have demonstrated impressive performance in distinguishing implant systems with high accuracy and efficiency.8,17 Some models have achieved accuracy rates exceeding those of experienced clinicians, suggesting that AI can address a clinically meaningful gap by providing rapid and objective classification. These models can analyze subtle geometric or radiographic patterns that are not easily perceived by human observers, thereby reducing the dependence on prior patient records or external consultations.
Importantly, the present study revealed a substantial willingness among dentists to adopt AI-based identification tools, with interest observed across all age groups. However, the high willingness to use AI-based implant identification tools observed in this study should be interpreted as reflecting conceptual openness and perceived clinical need rather than immediate readiness for real-world implementation. The survey did not address the practical factors that strongly influence adoption in clinical settings, such as cost, reimbursement, medicolegal liability, data governance, or integration into the existing clinical workflow. As a result, expressed willingness may overestimate actual adoption behavior when such constraints are considered. Nevertheless, this level of receptiveness is notable in the broader context of AI adoption in dentistry. Previous studies have generally reported a cautious uptake of AI technologies in clinical practice. Schwendicke et al. reported that concerns regarding data quality, responsibility, and trust slowed the clinical adoption of diagnostic AI systems.18 Similarly, Eschert et al. found that most clinicians rarely use AI in daily practice and express notable concerns regarding liability and data security, despite acknowledging its potential benefits.19 Against this background, the strong enthusiasm observed for implant identification tools in this study may reflect a domain in which clinicians perceive immediate and practical clinical needs, making them particularly receptive to AI-based support.
This study had several limitations. Convenience sampling may limit generalizability, and self-reported responses may be subject to recall or social desirability biases. In addition, recruitment was primarily conducted through implant-related academic and professional networks (KAOMI); therefore, the sample may represent an implant-engaged subgroup of dentists. This recruitment context may have influenced the reported frequencies of encountering unidentified implant systems, as well as the level of interest in AI-based identification tools, potentially reflecting the perspectives of dentists more actively engaged in implant treatment. Convenience sampling and self-reported data might affect the interpretation of the willingness to adopt AI tools, particularly regarding potential overestimation. In addition, the analyses were descriptive in nature, and no inferential statistical tests were performed because the study was designed as an exploratory survey aimed at characterizing dentists’ experiences and perceptions. Additionally, we did not evaluate the diagnostic accuracy of the clinicians' radiographic identification abilities or compare their performance with that of existing AI models. Future studies should examine whether AI-assisted identification improves clinical outcomes, reduces unnecessary implant removal, or enhances treatment efficiency. The evaluation of cost-effectiveness and user experience is essential for successful clinical adoption.
Overall, the findings highlighted significant unmet needs in implant information management, a fragmented landscape of identification methods, and strong clinician interest in AI-based solutions. The continued development of validated AI models coupled with standardized implant information systems may help address the long-standing challenges in implant maintenance and support safer and more efficient patient care.
Ⅴ. Conclusion
In this survey of practicing dentists, unknown implant systems remained a common clinical challenge, and dentists relied on multiple informal methods to obtain missing information. Awareness of existing identification services is limited, whereas the willingness to adopt AI-based tools is high. These findings reflect the perceptions of clinicians participating in this survey and highlight the need for accessible implant information support systems and further development of validated AI-based identification technologies.
Supplementary Material
Supplementary materials are available at The Korean Academy of Oral & Maxillofacial Implantology website (https://www.hst-j.org).
- KAOMI_2026002_Table_S1.pdf
Supplementary Table S1. Questionnaire items related to implant identification services
