

Ⅰ. Introduction
Medication-related osteonecrosis of the jaw (MRONJ) has been reported with antiresorptive agents such as bisphosphonates and denosumab, and more recently with angiogenesis inhibitors and immune modulators. Lenvatinib (Lenvima; Eisai Co., Ltd., Tokyo, Japan) is a multi-kinase inhibitor known to suppress several receptor tyrosine kinases, including VEGFR, FGFR, PDGFR, RET, and KIT. This therapeutic agent was approved by the Food and Drug Administration (FDA) for the treatment of thyroid cancer in 2015 and advanced hepatocellular carcinoma (HCC) in 2018.1
Mauceri et al. reported a case of lenvatinib-related osteonecrosis in 2019.2 The patient, a 58-year-old male diagnosed with thyroid cancer, developed osteonecrosis at the site of tooth extraction in the maxilla during lenvatinib treatment, leading to the diagnosis of MRONJ.
According to the 2022 AAOMS position paper, diagnosis of MRONJ requires the following criteria: (1) current or previous treatment with antiresorptive or antiangiogenic agents, (2) exposed bone or bone that can be probed through an intraoral or extraoral fistula in the maxillofacial region persisting for more than eight weeks, and (3) no history of radiation therapy to the jaws or obvious metastatic disease of the jaws.3 Therefore, MRONJ diagnosis thus requires the concomitant use of anti-resorptive agents along with angiogenesis inhibitors or immune modulators, excluding lenvatinib monotherapy as the sole cause.
Herein, we present a case of mandibular osteomyelitis following lenvatinib therapy for recurrent HCC and discuss the review of the existing literature.
Ⅱ. Case Report
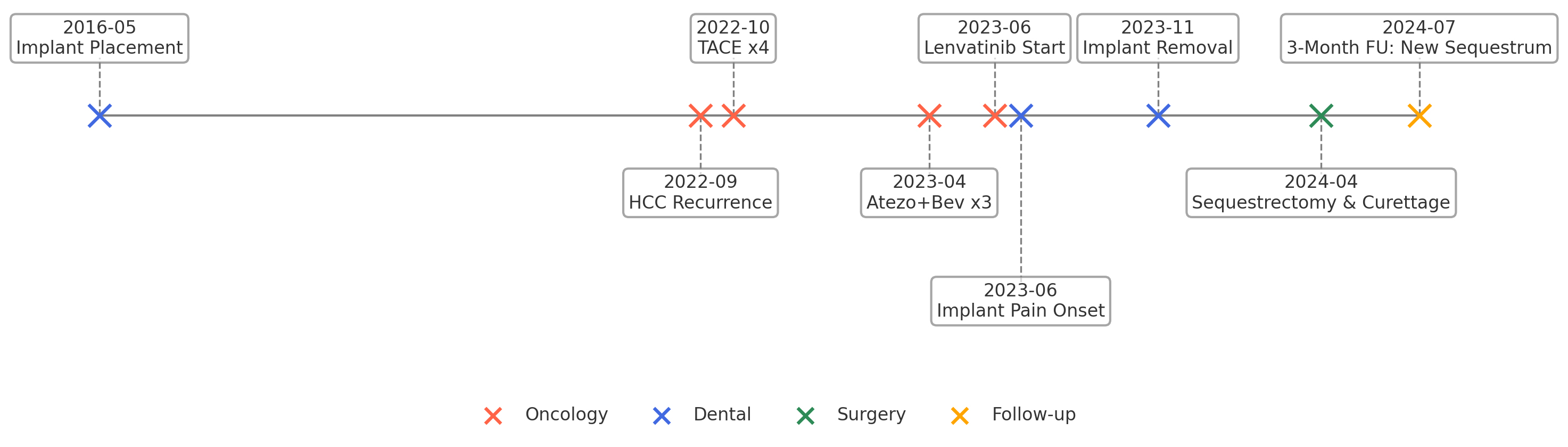
A 56-year-old male patient was presented to the Department of Oral and Maxillofacial Surgery at Yonsei University Gangnam Severance Hospital on November 6, 2023, with complaints of lower right gum pain that had started a few months prior. The patient was diagnosed with hepatocellular carcinoma (HCC) in 2007 and underwent right hemihepatectomy. In 2022, a computed tomography (CT) scan revealed recurrence, leading to four sessions of transarterial chemoembolization (TACE). Magnetic resonance imaging (MRI) 3 months later revealed marginal recurrence, and three cycles of atezolizumab plus bevacizumab chemotherapy were administered starting in April 2023. As this treatment failed, 13 cycles lenvatinib therapy were initiated in June 2023 (12 mg orally once a day for one month), with each lasting 4 weeks, were administered.
In 2016, dental implants were placed in Areas 47, 46, 45, and 44. In June, 2023, the patient experienced intermittent pain in these areas. Panoramic and other radiographic examinations revealed bone destruction around the implants (Fig. 1). In November 2023, implants i47 and 46 were removed at another institution.

Five months after implant removal, the patient revisited our outpatient clinic with persistent discomfort and increased swelling. Examination revealed swelling and warmth on the lower right side of the face. Intraoral examination revealed swelling and purulent discharge from the buccal vestibule and gingiva at the implant removal sites. Cone-beam computed tomography revealed significant progression of bone destruction and cortical disruption compared to those taken 5 months prior (Fig. 2). Excluding medication history, the clinical findings alone were consistent with Stage 2 MRONJ according to the AAOMS criteria.

Fig. 2
X-ray and a cone beam computed tomography (CBCT) image taken at the second visit. (A) Panoramic view. Compared to previous images, the implants were confirmed to have been removed, with more severe bone destruction (long arrow), (B) Axial view (CBCT). Cortical bone destruction and sequestrum (short arrow) with periosteal reaction (dotted arrow) in the surrounding area is noted.
The patient was hospitalized and treated with intravenous antibiotics (ampicillin 2000 mg / sulbactam 1000 mg three times a day (Unasyn; Pfizer Inc., New York, NY, USA)) and underwent sequestrectomy and curettage under general anesthesia on the third day of hospitalization. After one week of hospitalization, the patient was discharged and continued taking oral antibiotics (cefdinir, 100 mg three times a day, Omnicef; Abbott Laboratories, Chicago, IL, USA). At the most recent follow-up, one month later, the patient reported no significant symptoms, and the surgical site showed good healing. However, at the 3-month follow-up, an additional sequestrum was observed in the affected area and removed (Fig. 3). Several outpatient visits were planned to monitor the healing process at the surgical site and check for recurrence. The chronological sequences of oncological treatments, lenvatinib administration, onset of oral symptoms, imaging studies, and surgical interventions are summarized in Fig. 4.

Ⅲ. Discussion
The 2022 AAOMS position paper no longer includes MRONJ as a diagnosis for the single-agent use of anti-angiogenic agents, tyrosine kinase inhibitors, mammalian target of rapamycin inhibitors, or immune checkpoint inhibitors.3 Therefore, this case cannot be strictly diagnosed as MRONJ. Instead, this was termed “osteonecrosis of the jaw induced by lenvatinib” or “lenvatinib-related osteonecrosis of the jaw,” which warrants further research.
Lenvatinib is a selective multi-targeted tyrosine kinase inhibitor (TKI) that targets VEGFR 1, 2, and 3; FGFR 1, 2, 3, and 4; and PDGFRβ.1 FGFR 4 inhibition is particularly important for lenvatinib’s anticancer effects.4 This agent has been approved in over 70 countries for several malignancies, including radioiodine-refractory differentiated thyroid carcinoma, unresectable HCC, unresectable thymic carcinoma, advanced renal cell carcinoma, and recurrent endometrial carcinoma.4 The global market for lenvatinib is expected to continue to grow.5
The known side effects of lenvatinib include hypertension, proteinuria, diarrhea, and fatigue, which are consistent with the adverse-event profile of other TKIs.4 Although TKIs have been known to contribute to MRONJ, reports specifically related to lenvatinib are rare.2
This patient in the present report was treated with atezolizumab and bevacizumab before lenvatinib, and although rare, bevacizumab could be associated with MRONJ.6 In the past 10 years, there have been two case reports of osteonecrosis of the jaw associated with bevacizumab. In these cases, the patients received bevacizumab 32 and 38 times, respectively.7,8 Both case reports identified the discontinuation of bevacizumab as a critical factor in the healing of osteonecrosis. The half-life of bevacizumab is approximately 20 days, and previous studies have demonstrated that cessation of bevacizumab for 5 to 6 weeks reduces the incidence of postsurgical complications associated with bevacizumab.9 In the present case, the patient received only three infusions of bevacizumab, after which bevacizumab was discontinued and the medication was changed to lenvatinib. Despite the discontinuation of bevacizumab, the osteonecrosis continued to worsen. Therefore, the effect of bevacizumab may be insignificant in this case.
In the present case, bone loss was observed around the implants, which is a common feature of peri-implantitis. Although bone loss in peri-implantitis is typically localized around an implant and has clear boundaries,10 the present case showed relatively extensive bone loss with indistinct margins, making it difficult to diagnose typical peri-implantitis. In addition, the patient reported persistent throbbing pain after implant removal, which is not a common symptom of non-acute peri-implantitis.
Reports of MRONJ around dental implants are increasing.11 Kwon et al. classified MRONJ around implants into implant surgery-triggered and non-implant surgery-triggered types.12 In this case, the patient developed peri-implant lesions 7 years after the implants were placed, suggesting the possibility of a non-implant surgery-triggered type. However, Boffano et al. reported that minor oral surgeries are approximately 40 times more frequent triggers of MRONJ compared to peri-implantitis.13 Given that the patient’s symptoms worsened after implant removal, the removal of the implant may have acted as a factor in worsening or triggering osteonecrosis, rather than treating it.
Furthermore, surgical resection and curettage was selected as the treatment regime in the present case. The previous consensus, which emphasized conservative approaches, has recently evolved to recognize the usefulness of early surgical intervention.14 For this patient, a more aggressive surgical approach was deemed necessary rather than the previously recommended debridement aimed at reducing soft tissue irritation. The patient healed well after surgical resection.
Advances in chemotherapy for malignant lesions are rapidly progressing; notably, reports of MRONJ associated with anticancer drugs are also increasing annually. Although this case did not meet the 2022 AAOMS MRONJ criteria, it suggests a potential association between lenvatinib therapy and jaw osteonecrosis. Given that the diagnosis of MRONJ relies mainly on the medication history and clinical findings, evolving guidelines may warrant the recognition of lenvatinib-associated osteonecrosis as a distinct entity.
