

Ⅰ. Introduction
A shallow vestibule with mobile soft tissue along the edentulous ridge represents a major challenge for achieving adequate denture retention and stability,1 often resulting from alveolar ridge resorption following tooth extraction.2 These conditions also pose challenges in implant therapy,3 particularly when ridge augmentation procedures require coronal advancement of vestibular tissues for primary wound closure using vertical and/or periosteal releasing incisions.2
To restore vestibular depth, several vestibuloplasty techniques have been proposed. The earliest technique, described by Kazanjian,4 involves a split-thickness apically positioned flap (APF) with healing by secondary epithelialization. However, this approach is prone to relapse secondary to wound contraction and coronal reattachment of the muscualture.5 To reduce relapse, the addition of a free gingival graft (FGG) was later introduced.6 Edlan and Mejchar described an alternative technique7 using a superficial U-shaped incision, with vertical limbs extending to the ridge crest and a horizontal base directed toward the lip. This design allows elevation of a superficial flap that is repositioned onto the bone surface, while the deep mucoperiosteal flap is mobilized outward. This method is technically similar to the lip-switch technique.8 Another option is submucosal vestibuloplasty,9 which is suitable for sites with adequate bone volume, healthy mucosa, and coronal muscle attachments. Both open and closed approaches have been described.10 In the closed approach, scissors are used to undermine the tissue between vertical incisions to create a tunnel, followed by removal of the intervening connective tissue. This technique is technically simpler than the previously described methods.>To restore vestibular depth, several vestibuloplasty techniques have been proposed. The earliest technique, described by Kazanjian,4 involves a split-thickness apically positioned flap (APF) with healing by secondary epithelialization. However, this approach is prone to relapse secondary to wound contraction and coronal reattachment of the muscualture.5 To reduce relapse, the addition of a free gingival graft (FGG) was later introduced.6 Edlan and Mejchar described an alternative technique7 using a superficial U-shaped incision, with vertical limbs extending to the ridge crest and a horizontal base directed toward the lip. This design allows elevation of a superficial flap that is repositioned onto the bone surface, while the deep mucoperiosteal flap is mobilized outward. This method is technically similar to the lip-switch technique.8 Another option is submucosal vestibuloplasty,9 which is suitable for sites with adequate bone volume, healthy mucosa, and coronal muscle attachments. Both open and closed approaches have been described.10 In the closed approach, scissors are used to undermine the tissue between vertical incisions to create a tunnel, followed by removal of the intervening connective tissue. This technique is technically simpler than the previously described methods.
Although vestibuloplasty techniques were originally developed to improve denture retention and stability, they can also be applied to enhance peri-implant health.11 However, the Edlan–Mejchar technique is associated with relapse,12 and APF with FGG is linked to considerable patient morbidity and postoperative complications.13 In addition, both procedures are highly technique-sensitive.
Keratinized tissue comprises the keratinized gingiva surrounding natural teeth and the keratinized mucosa around implants. Attached gingiva or mucosa refers to immobile tissue located apical to the marginal soft tissue and supported by a dense collagen fiber network with periosteal attachment.
In this study, we propose a modified submucosal vestibuloplasty technique performed during second-stage implant surgery to achieve adequate vestibular depth and clinically attached mucosa. This approach is less technique-sensitive and is associated with reduced patient morbidity and fewer complications.
Ⅱ. Case report
1. Surgical procedure
The modified submucosal vestibuloplasty is performed during second-stage implant surgery. A midcrestal incision is made along the alveolar ridge crest adjacent to the previously placed implant (Fig. 1A). The coronal portion of the buccal flap was elevated as a full-thickness flap to expose the implant cover screw and approximately 3 mm of the buccal bone (Fig. 1B). The apical portion of the buccal flap is elevated as a superficial split-thickness flap using a blade, creating a thin outer epithelial layer and a deeper layer containing the majority of the connective tissue (Fig. 1C). This deeper connective tissue and periosteum are then separated from the underlying bone and apical tissues through a horizontal incision at the apical level, followed by blunt dissection (Fig. 1D and 1E). The cover screw is replaced with a healing abutment, and simple interrupted sutures are placed around the healing abutment. A double horizontal mattress suture is used to secure the flap and periosteum at the most apical aspect of the vestibule (Fig. 1F).
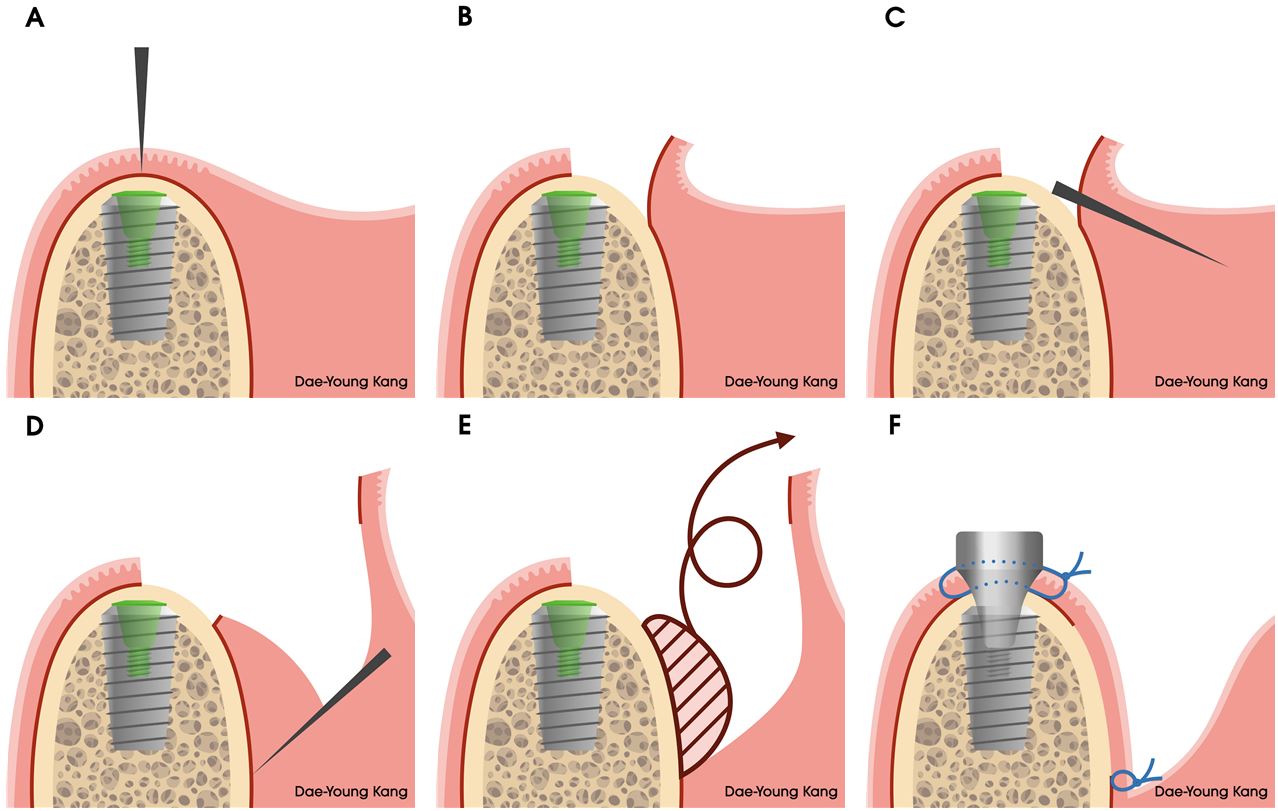
Fig. 1
Schematic illustration of the modified submucosal vestibuloplasty around an implant. (A) A midcrestal incision is made along the alveolar ridge crest at the implant site, (B) A full-thickness flap is elevated to expose the cover screw, (C) A superficial incision is made to elevate a split-thickness flap, (D) The deeper connective tissue and underlying periosteum are separated from the superficial flap through a horizontal incision at the apical level, (E) These tissues are removed by blunt dissection, (F) A healing abutment is attached, and simple interrupted sutures are placed around the implant. A double horizontal mattress suture is used to anchor the flap and periosteum at the most apical level of the vestibule.
2. Case presentation
A 65-year-old systemically healthy woman presented to the Department of Periodontology in Dankook University Dental Hospital for implant rehabilitation of a mandibular edentulous area. Clinical and radiographic examinations revealed missing teeth at sites #35, #36, #37, #46, and #47, with severe alveolar bone atrophy, particularly in the right posterior region, as well as a periapical radiolucency associated with tooth #44. Implant placement with simultaneous guided bone regeneration (GBR) was planned at sites #35, #37, #46, and #47.
All surgical procedures were performed under local infiltration anesthesia using 2% lidocaine with 1:80,000 epinephrine by a single periodontist. Following a midcrestal incision, internal submerged implants were placed at sites #35, #37, #46, and #47 (Superline II; Dentium, Suwon, Korea). Vertical and horizontal GBR was carried out after decortication using a titanium mesh with a spacer (CTi-mem, CTi-spacer; Neobiotech, Wonju, Korea) and deproteinized bovine bone mineral (Bio-Oss; Geistlich, Wolhusen, Switzerland). The flap was mobilized using a periosteal releasing incision, and wound closure was achieved with interrupted sutures using 6‒0 monofilament nylon (Ethilon; Ethicon, Somerville, NJ, USA). All sutures were removed after two weeks (Figs. 2 and 3). Healing at all surgical sites was uneventful.
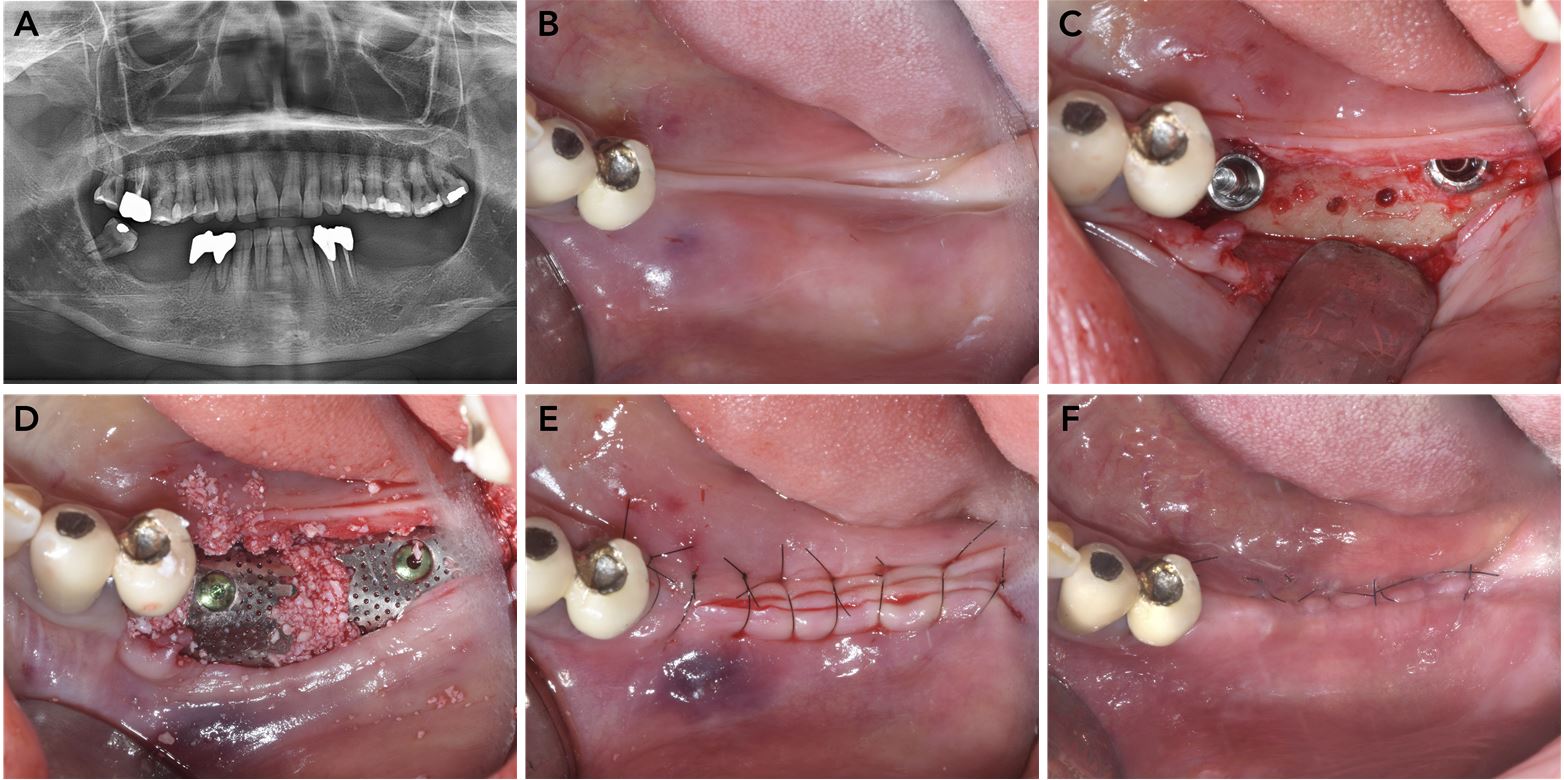
Fig. 2
Implant placement with guided bone regeneration in the left mandible. (A) Panoramic radiograph at the initial examination, (B) Preoperative occlusal view of the left mandibular edentulous area, (C) Implant placement and decorticationj, (D) Guided bone regeneration using a titanium mesh and deproteinized bovine bone mineral, (E) Wound closure with simple interrupted nylon sutures, (F) Suture removal after two weeks.
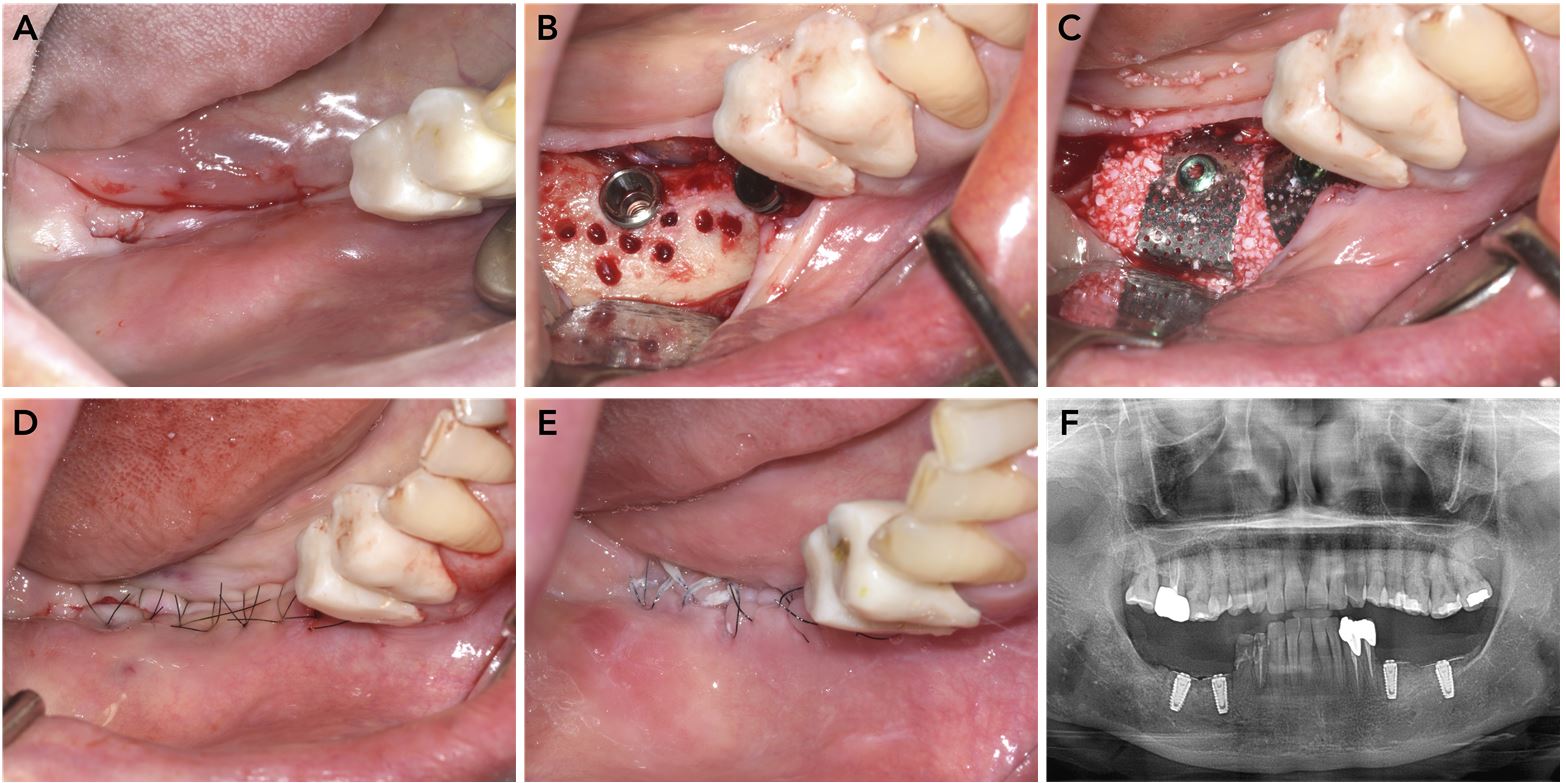
Fig. 3
Implant placement with guided bone regeneration in the right mandible. (A) Preoperative occlusal view of the right mandibular edentulous area, (B) Implant placement and decortication, (C) Guided bone regeneration using a titanium mesh and deproteinized bovine bone mineral, (D) Wound closure with simple interrupted nylon sutures, (E) Suture removal after two weeks, (F) Postoperative panoramic radiograph.
The modified submucosal vestibuloplasty was performed during second-stage implant surgery after a four-month healing period (Figs. 4 and 5). Preoperative clinical photographs showed complete absence of both buccal and lingual vestibules, with a concave contour of the augmented alveolar ridge. Under local anesthesia, a midcrestal incision was made adjacent to the implant site, and a full-thickness flap was elevated to expose the titanium mesh. The titanium meshes and spacers were then removed. The apical portion of the flap was superficially elevated using a blade to achieve tissue thinning. The underlying connective tissue and periosteum were separated from the bone and apical tissues through a horizontal apical incision and blunt dissection. Healing abutments were attached, and simple interrupted sutures were placed around the healing abutments using 6‒0 monofilament nylon (Ethilon). A double horizontal mattress suture was used to anchor the flap at the most apical level of the vestibule using 5‒0 monofilament nylon (Ethilon). The newly formed vestibule remained stable following suture removal and after final prosthesis delivery.
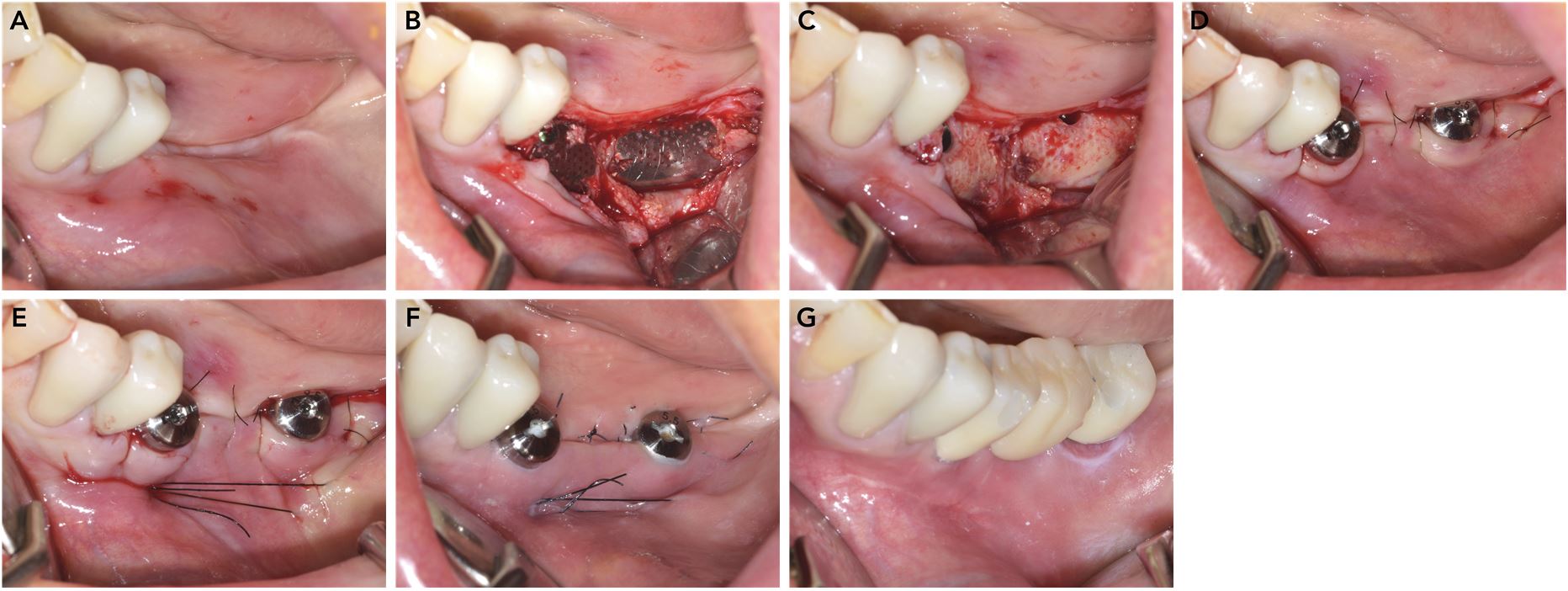
Fig. 4
Implant second-stage surgery in the left mandible. (A) Preoperative occlusal view, (B) Elevation of a full-thickness flap through a crestal incision, (C) Removal of the spacers and titanium meshes, (D) Attachment of healing abutments and placement of simple interrupted sutures following the buccal thinning procedure, (E) Placement of a double horizontal mattress suture to anchor the flap at the most apical level of the vestibule, (F) Suture removal after two weeks, (G) Final implant-supported bridge.
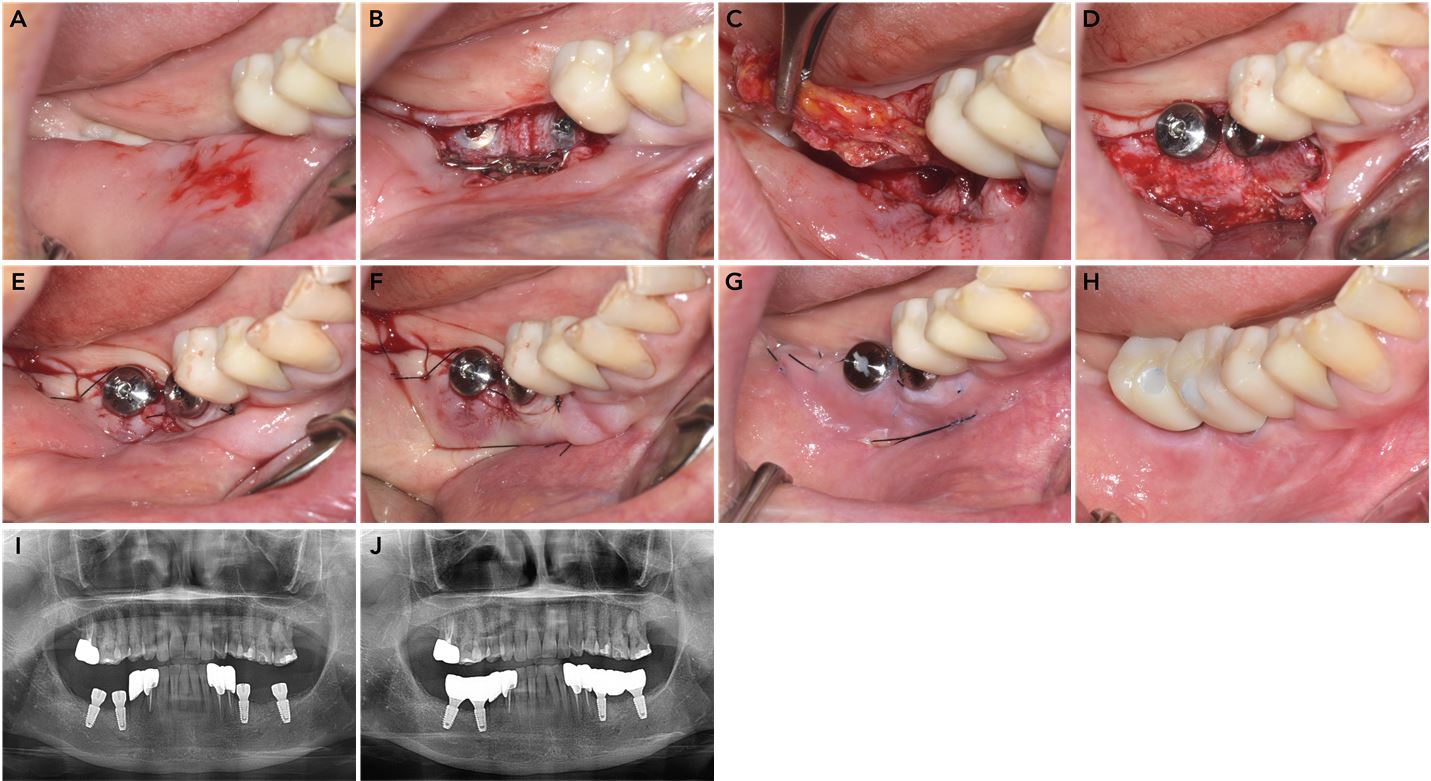
Fig. 5
Implant second-stage surgery in the right mandible. (A) Preoperative occlusal view, (B) Elevation of full-thickness flap through a crestal incision with removal of the titanium meshes, (C) Removal of buccal connective tissue and periosteum during the thinning procedure, (D) Attachment of healing abutments, (E) Placement of simple interrupted sutures, (F) Placement of a double horizontal mattress suture to anchor the flap at the most apical part of the vestibule, (G) Suture removal after two weeks, (H) Final delivery of the implant-supported prosthesis, (I) Panoramic radiograph obtained after second-stage implant surgery, (J) Panoramic radiograph obtained after final prosthesis delivery.
Ⅲ. Discussion
Adequate vestibular depth is essential for denture retention as well as for maintaining peri-implant health. The vestibule surrounding implants can be markedly reduced following coronal advancement of the flap during GBR procedures, particularly after releasing incisions and suturing. A shallow vestibule may compromise the maintenance of peri-implant soft and hard tissues and increase the risk of peri-implant disease.3 Therefore, restoration of lost vestibular depth with clinically attached mucosa during implant surgery is recommended.
Attached gingiva is considered important for maintaining periodontal health.14 Attached tissue is defined by its immobility, whereas keratinized tissue additionally provides a protective keratinized epithelial surface. However, the necessity of keratinized mucosa around implants remains controversial in the literature.15, 16 Clinically, the presence of keratinized tissue may reduce brushing discomfort and limit mobility of the peri-implant mucosa. Consequently, various surgical procedures have been performed to obtain an adequate width of keratinized tissue, often targeting approximately 2 mm, in conjunction with sufficient vestibular depth. Tarnow et al. defined the zone of attached tissue as a component of keratinized tissue based on the level of epithelial and connective tissue attachment: (1) the distance from the sulcus to the mucogingival junction (MGJ) in supracrestal attachment, as seen around healthy teeth or tissue-level implants; and (2) the distance from the bone crest to the MGJ in subcrestal attachment, as observed around healthy bone-level implants or sites with facial infrabony defects.17
Functional resistance to mastication and toothbrushing, as well as the immobility of tissues coronal to the MGJ, arise from the keratinized epithelium and the dense, collagen fiber-rich connective tissue, respectively. The Edlan–Mejchar technique and submucosal vestibuloplasty do not increase the amount of keratinized tissue; rather, they convert mobile, non-keratinized tissue apical to the MGJ into immobile, clinically attached non-keratinized tissue through removal of the elastic fiber layer.
In this case, non-keratinized yet clinically attached mucosa was successfully created, and vestibular depth was re-established by removing the submucosal elastic fiber layer beneath the non-keratinized mucosa. The procedure was simpler and less technically demanding than APF with FGG or the Edlan–Mejchar technique. To the best of our knowledge, submucosal vestibuloplasty has previously been used primarily in patients with dentures, and this case represents the first application of this approach in peri-implant sites.
Although FGG demonstrates high predictability, it has several limitations, including the need for an additional donor site, limited availability of donor tissue, and increased postoperative pain and bleeding because the palatal donor site heals by secondary intention.13 The Edlan–Mejchar technique is associated with few complications; however, it is technique-sensitive and carries a risk of relapse.12
The main advantage of the modified submucosal vestibuloplasty lies in its simplicity and low morbidity. Elevation of approximately 3 mm of a full-thickness flap after the initial incision helps preserve soft tissue thickness adjacent to the implant and may reduce the risk of bone resorption.18
This study has several limitations, including insufficient long-term follow-up to assess the stability of the newly formed attached mucosa, absence of quantitative measurements of vestibular depth and keratinized tissue changes, and lack of histologic evaluation to confirm barrier function and tissue immobility comparable to those of keratinized attached mucosa. Nevertheless, the simplicity and reduced morbidity of this technique make it a practical alternative to more complex conventional approaches.
Ⅳ. Conclusion
The modified submucosal vestibuloplasty technique presented in this case report can be used to restore vestibular depth during second-stage implant surgery. This approach provides a simple method to establish stable, non-keratinized yet clinically attached mucosa and restore the vestibule. However, further studies are required to evaluate the long-term stability and histologic characteristics of the newly formed mucosa.
