

Ⅰ. Introduction
Ⅱ. Case Report
1. Surgical procedures of alveolar ridge preservation via intrasocket granulation tissue repositioning
2. Case presentation
Ⅲ. Discussion
Ⅳ. Conclusion
Ⅰ. Introduction
After tooth extraction, the alveolar ridge is prone to rapid resorption, particularly at sites compromised due to periodontal or endodontic pathologies. Within the first 6 months, a substantial proportion of the ridge width, often exceeding 50%, may be lost, primarily due to collapse of the socket walls and coronal migration of soft tissues.1,2 These morphological changes can adversely impact both the esthetic and functional outcomes of subsequent implant therapy.3
To address this, various alveolar ridge preservation (ARP) strategies have been developed, typically involving socket grafting with or without barrier membranes, along with attempts to achieve primary closure.4,5,6,7,8 However, conventional ARP protocols often rely on complete debridement of intrasocket tissue and tension-based flap advancement, which can increase the risk of soft tissue contraction, scarring, or wound dehiscence, particularly in the esthetic zone. Moreover, standard releasing incisions may compromise the mucogingival junction or vestibular depth, leading to suboptimal soft tissue outcomes.3 Recent studies have challenged the routine removal of intrasocket granulation tissue, suggesting that, particularly in chronic periodontal lesions, such tissue may retain progenitor cells with regenerative potential, including mesenchymal stem-like populations.9,10 Clinical data further indicate that selective preservation of viable tissue may enhance early healing and reduce the need for secondary grafting procedures.11,12,13
In light of these findings, we propose a biologically driven technique, termed intrasocket granulation tissue repositioning, in combination with a novel extra-socket incision, known as the Bone-Key (BK) incision. This approach involves selective elevation and coronal repositioning of the viable intrasocket granulation tissue to assist in soft tissue closure while preserving the mucogingival junction and avoiding excessive flap tension.
The present technical note outlines a clinical case in which the intrasocket granulation tissue repositioning method was used in conjunction with the BK incision. Here, we describe the surgical sequence, healing progression, and radiographic outcomes, offering an alternative concept for soft tissue management in ridge-preservation therapy.
Ⅱ. Case Report
1. Surgical procedures of alveolar ridge preservation via intrasocket granulation tissue repositioning
A full-thickness flap was carefully elevated at the extraction site using a minimally invasive approach. To minimize tension and preserve the mucogingival junction, an extrasocket incision, referred to as a BK incision, was designed and performed using a No. 15 scalpel in an area with sufficient underlying bone volume (Fig. 1A). Following full-thickness flap elevation (Fig. 1B), the intrasocket granulation tissue was preserved rather than removed. The tissue was gently detached in a subperiosteal plane, keeping it viable and intact for coronal repositioning (Fig. 1C). The extraction socket was debrided to remove necrotic or nonviable tissues while maintaining the integrity of the intrasocket granulation tissue lining. The socket was then filled with bone graft material to maintain ridge volume (Fig. 1D). Subsequently, the preserved granulation tissue was repositioned coronally to function as a biological seal over the grafted socket (Fig. 1E). The flap was then repositioned and sutured with minimal tension using simple interrupted sutures (Fig. 1F).
This intrasocket granulation tissue repositioning protocol emphasizes the use of patient-derived granulation tissue as a functional component in socket closure, whereas the BK incision facilitates atraumatic soft tissue handling and favorable wound stabilization.
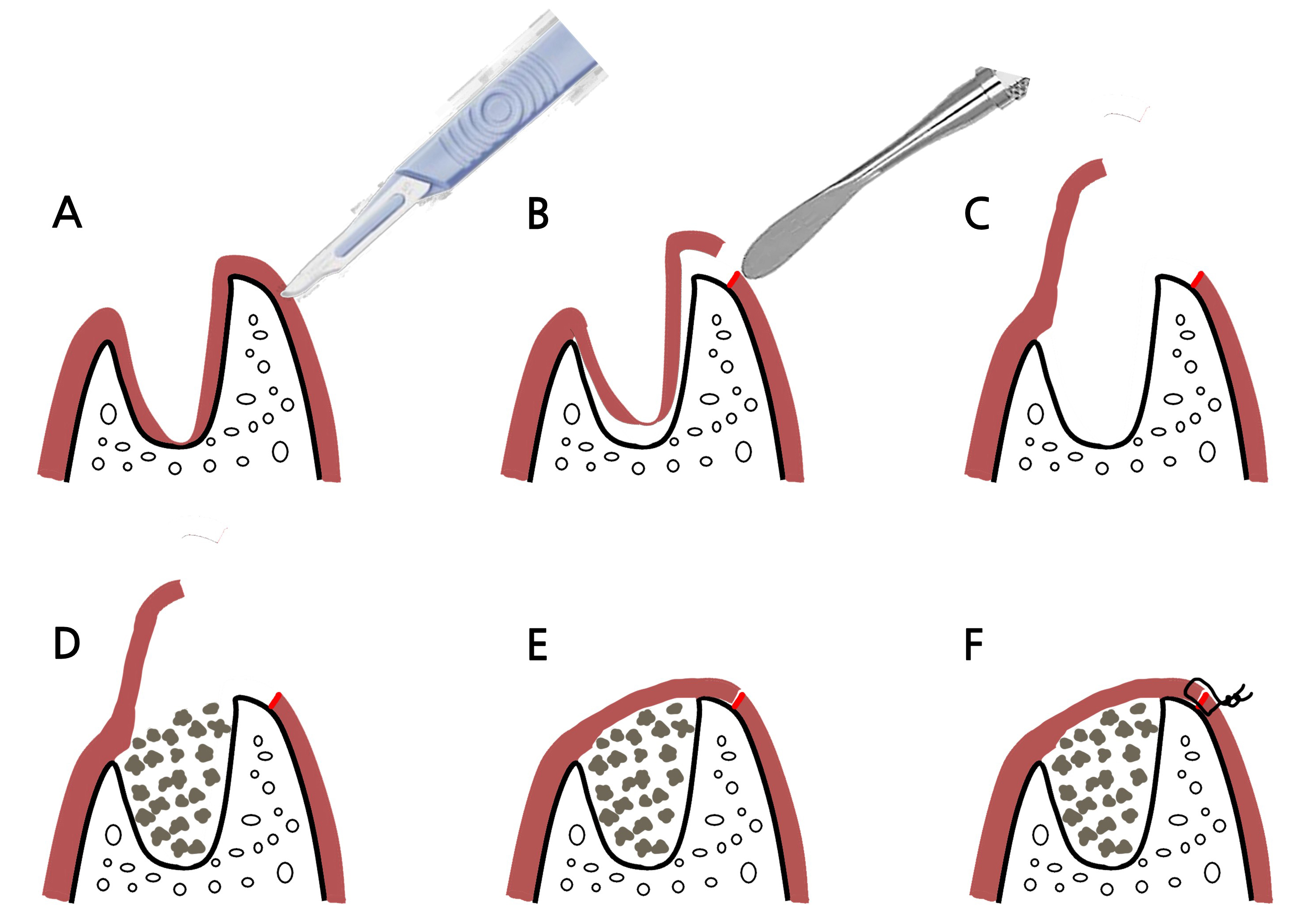
Fig. 1
Schematic illustration of the intrasocket granulation tissue repositioning technique. (A) Extrasocket incision using a No. 15 blade for Bone-Key incision, (B, C) Full-thickness flap elevation including the intrasocket granulation tissue, (D) Graft placement using octacalcium phosphate-based synthetic bone graft material, (E, F) Coronal repositioning of the viable granulation tissue followed by tension- free flap closure.
2. Case presentation
A 42-year-old female patient with no relevant medical history presented to a dental clinic in 2023 with a chief complaint of increased mobility of the maxillary anterior tooth. Radiographic and clinical examinations revealed advanced alveolar bone loss around tooth #11, with particularly pronounced loss in the labial aspect of the socket (Fig. 2). After a comprehensive evaluation, ARP via the intrasocket granulation tissue repositioning technique was planned for the extraction site, followed by delayed implant placement.
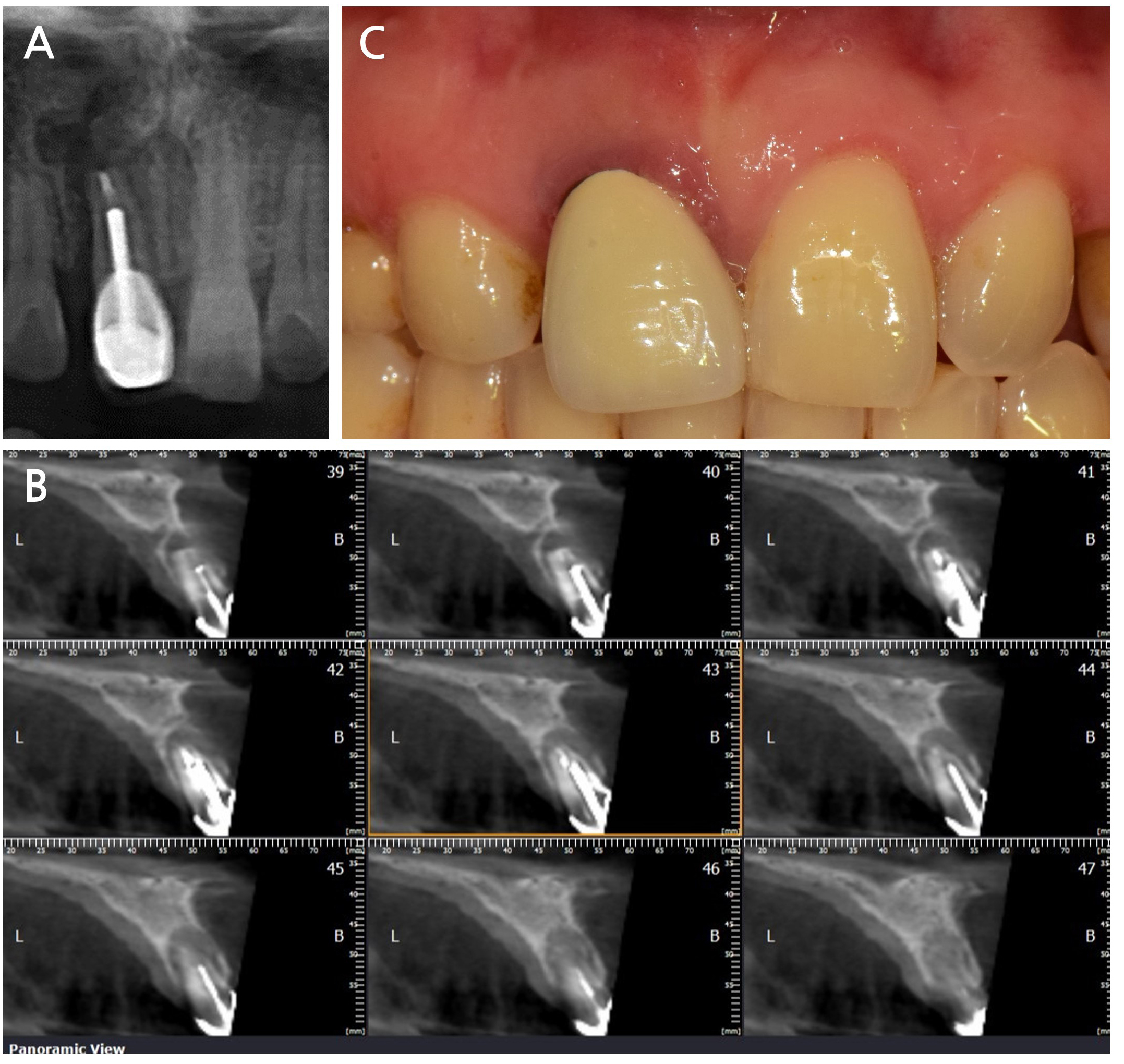
Fig. 2
Initial clinical and radiographic findings. (A) Periapical radiograph and (B) cone-beam computed tomography images revealing advanced bone loss on the labial aspect of tooth #11, (C) A clinical photograph showing inflamed, reddish gingiva around tooth #11, indicating localized periodontal inflammation.
All surgical procedures were performed by a single experienced periodontist (BKP). Under local anesthesia, an extra-socket BK incision was made on the palatal aspect using a No. 15 scalpel (Fig. 3A). A full-thickness flap, including the intrasocket granulation tissue, was carefully elevated to access the extraction socket (Fig. 3B and 3C). After gentle debridement of the necrotic tissues, a resorbable collagen membrane was applied exclusively to the labial socket wall where severe alveolar bone loss was evident (Fig. 3D). Biomimetic octacalcium phosphate-based synthetic bone graft material (Bontree plus®; HudensBio Co., Gwangju, Korea) was then grafted into the socket. The preserved intrasocket granulation tissue was repositioned coronally over the grafted area and sutured to serve as a biological sealing layer (Fig. 3E and 3F). All sutures were removed after 2 weeks of healing (Fig. 4).
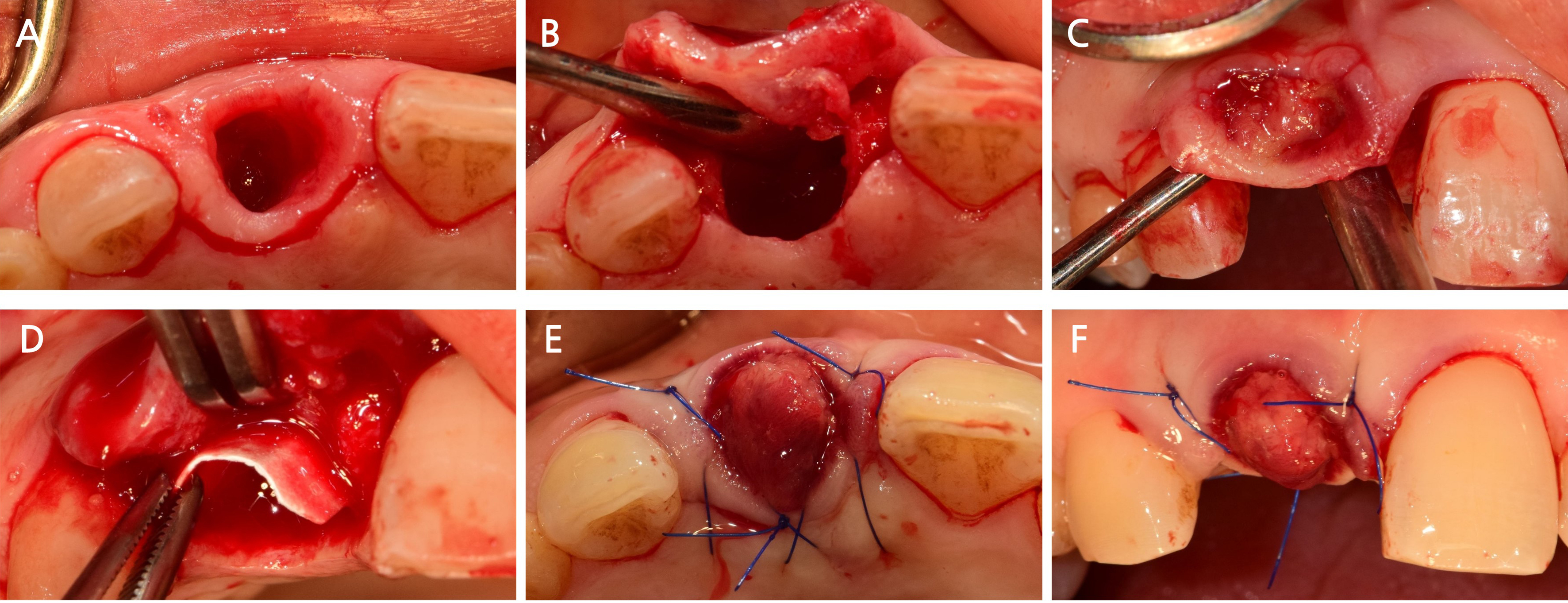
Fig. 3
Intraoperative sequence of the surgical procedure. (A) Extrasocket Bone-Key incision created palatally to facilitate flap mobilization, (B) Elevation of full-thickness flap including intact granulation tissue, (C) Granulation tissue preserved and elevated without rupture, (D) Octacalcium phosphate-based synthetic bone graft material placed after labial bone surface debridement and collagen membrane coverage, (E, F) Repositioning of the granulation tissue coronally to seal the socket, followed by tension-free flap closure.
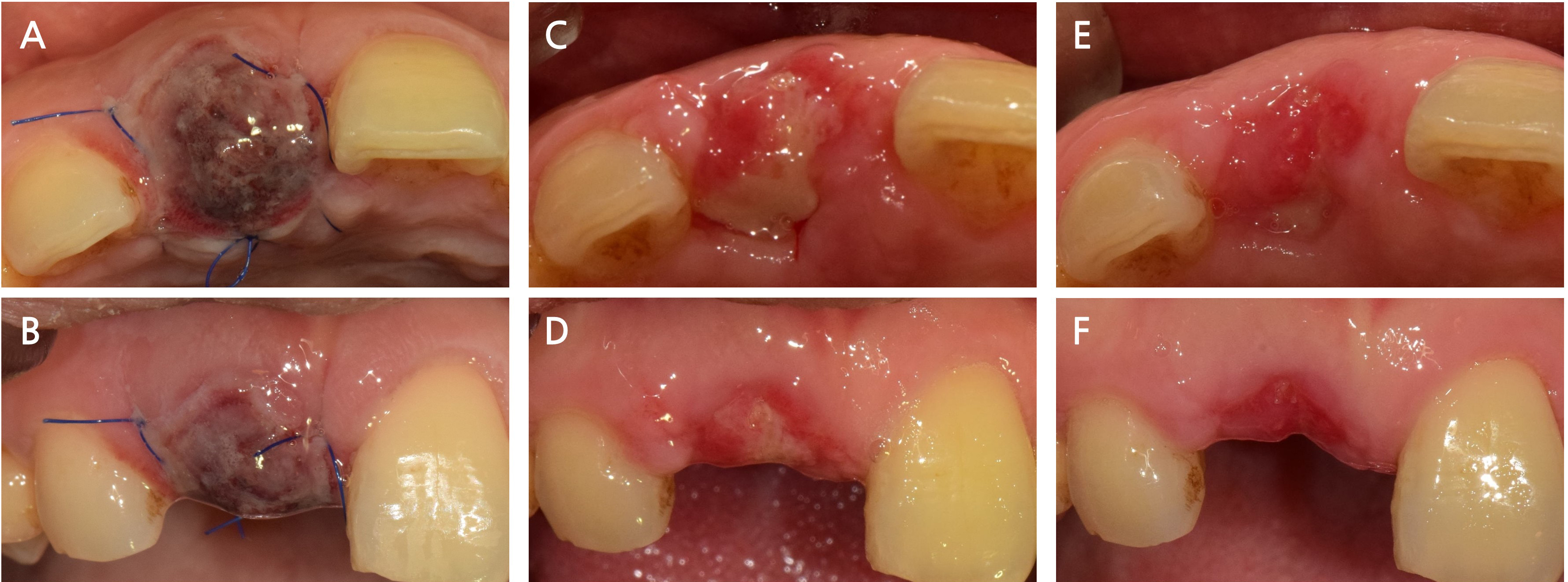
Fig. 4
Postoperative healing sequence. (A, B) Two days after surgery: initial soft tissue closure with mild edema; socket seal appears intact without signs of bleeding or dehiscence, (C, D) Two weeks after surgery: progressive epithelialization and maturation of the flap margin observed; no signs of inflammation or graft exposure, (E, F) Three weeks after surgery: well-integrated soft tissue architecture with stable keratinized gingiva and no signs of wound complications.
Following 2 months of uneventful healing (Fig. 5A to 5C), an internal-type dental implant (Superline®; Dentium, Suwon, Korea) was placed using a computer-guided surgical guide (Fig. 5D and 5E). The final prosthetic restoration was delivered 6.5 months after the initial ARP procedure using intrasocket granulation tissue repositioning (Fig. 5F and 5G). Radiographic and clinical evaluations performed 18 months after surgery confirmed a stable peri-implant marginal bone levels without resorption, along with healthy surrounding soft tissues, indicating periodontal stability (Fig. 5H and 5I).
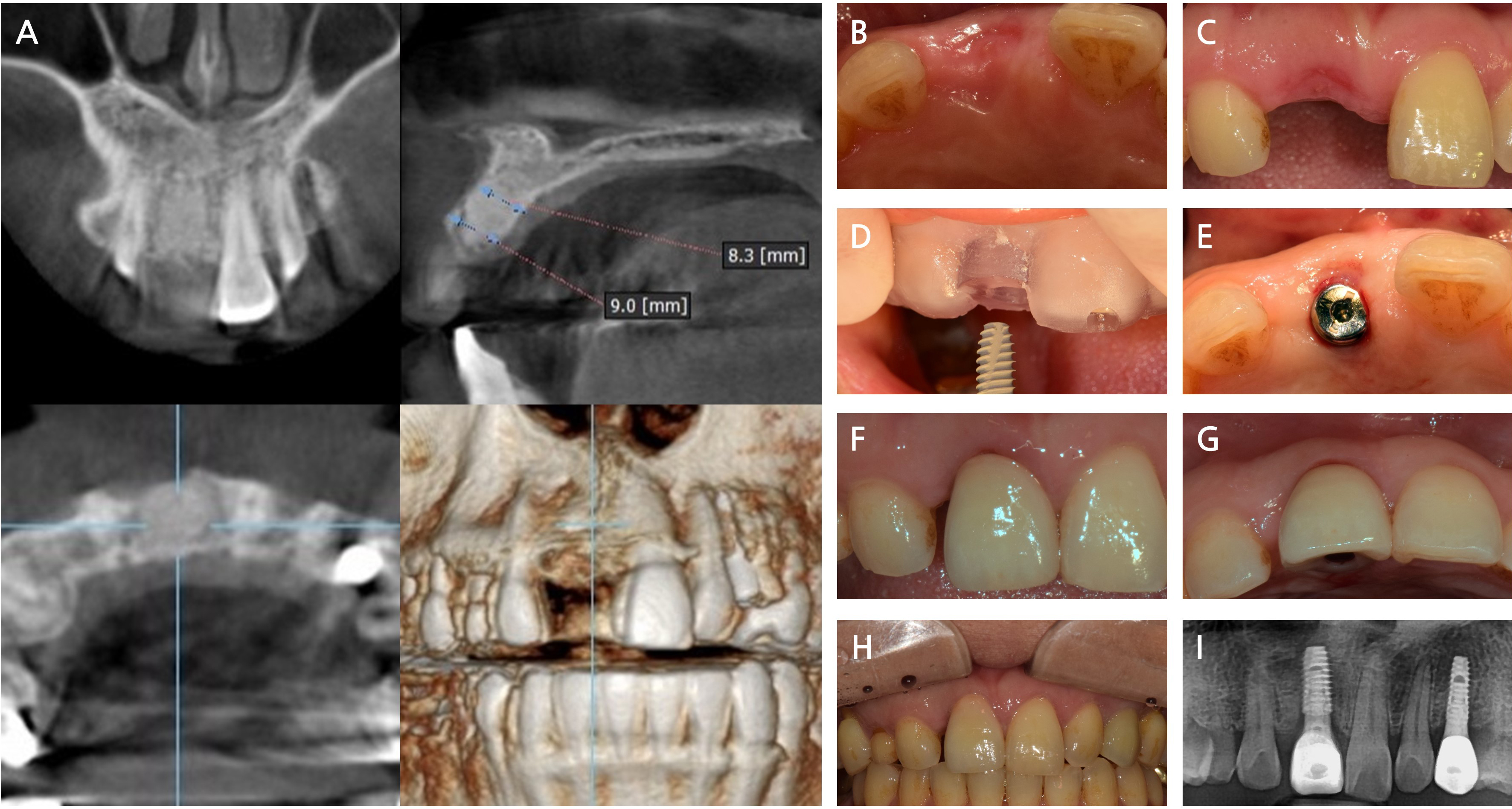
Fig. 5
Surgical procedure of implant placement and follow-up outcomes after alveolar ridge preservation (ARP) using intrasocket granulation tissue repositioning. (A) A cone-beam computed tomography image 2 months after ARP showing adequate bone volume for implant placement, (B, C) Preoperative clinical images demonstrating stable soft tissue contour and adequate ridge dimensions, (D) Implant placement using computer-guided surgery based on a customized surgical stent, (E) Healing abutment installed following implant insertion, (F, G) Final prosthesis delivered 6.5 months after ARP, showing satisfactory esthetic integration with the surrounding tissue, (H, I) Clinical and radiographic evaluation 18 months postoperatively, revealing stable marginal bone level and healthy peri-implant soft tissue.
Ⅲ. Discussion
This case report introduces a novel biologically driven approach for ARP via intrasocket granulation tissue repositioning. Unlike conventional ARP protocols that prioritize complete debridement of the reactive tissue, the intrasocket granulation tissue repositioning technique leverages the regenerative potential of preserved intrasocket granulation tissue to biologically seal the grafted socket. This is facilitated by a unique BK incision that allows tension-free flap advancement while preserving the mucogingival junction. The originality of this approach lies in its dual emphasis on conserving viable reactive tissue and minimizing surgical trauma, which results in favorable soft tissue healing and ridge maintenance without the use of membranes or additional soft tissue grafts. To the best of our knowledge, this is one of the first clinical reports to systematically combine intrasocket granulation tissue with a minimally invasive extrasocket access flap design, including a BK incision, potentially setting the stage for a new paradigm in biologically guided ARP.
Intrasocket granulation tissue has traditionally been viewed as a pathological remnant of chronic inflammation that should be completely removed during socket debridement.14,15 This perspective was reinforced by early histological studies showing infiltration of inflammatory cells and delayed bone formation within such tissues.14 However, growing evidence challenges this assumption. Recent histological and molecular investigations have demonstrated that intrasocket granulation tissue may harbor stem-like cells and osteogenic precursors that participate in socket healing, particularly in the early stages.9,10 Several case-based studies have also supported this biologically permissive view. Mardinger et al.11 first demonstrated that preserved intrasocket granulation tissue can be used to achieve soft tissue closure in severely compromised extraction sites. Hur et al.12 and Moreno-Rodríguez et al.13 further validated the potential of intrasocket granulation tissue as a natural socket-sealing material, emphasizing its utility in reducing surgical complexity and enhancing wound stability.
In this case, the intrasocket granulation tissue repositioning protocol was successfully applied to a compromised anterior site with advanced labial bone loss. Clinical outcomes demonstrated favorable healing, soft tissue integration, and dimensional stability. Notably, when compared with conventional ARP using a collagen membrane as a socket-sealing material in a similar clinical context (Fig. 6), the site treated via the intrasocket granulation tissue repositioning technique showed enhanced soft tissue closure and reduced flap tension within 2 weeks. These findings suggest that the combined use of intrasocket granulation tissue and a BK incision may optimize both the biological and mechanical aspects of socket healing.
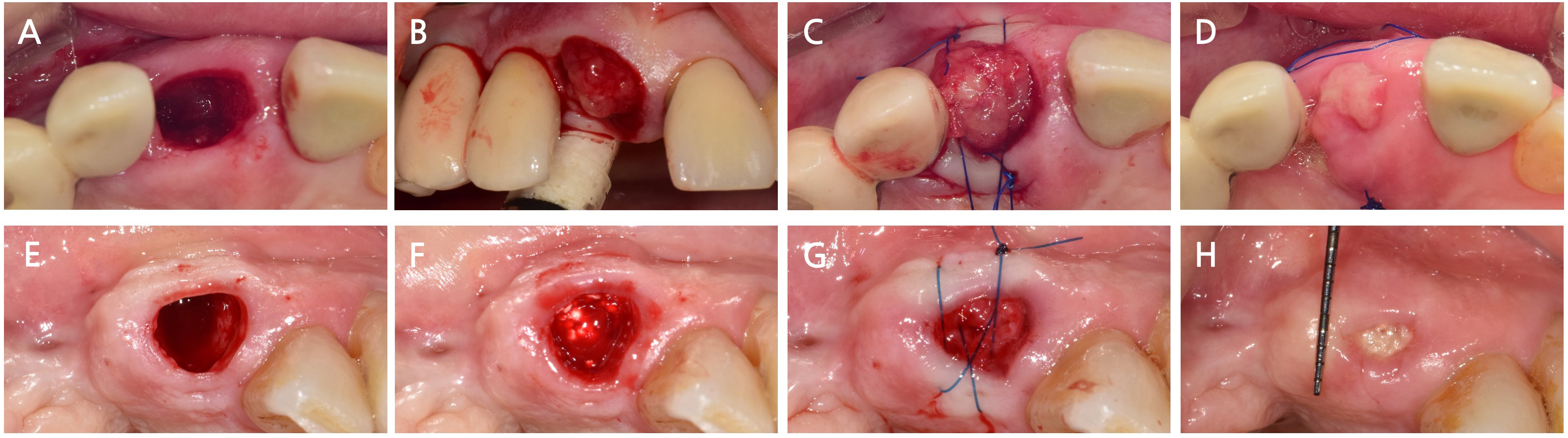
Fig. 6
Comparison of healing processes following alveolar ridge preservation (ARP) using intrasocket granulation tissue repositioning (A–D) and conventional ARP using a collagen membrane (E–H). (A) Occlusal view prior to surgery in the intrasocket granulation tissue repositioning case, (B) Bone graft placement after gentle socket debridement, (C) Socket sealed by coronally repositioned granulation tissue without membrane application, (D) Clinical healing at 2 weeks showing favorable soft tissue coverage and flap stability, (E) Occlusal view prior to surgery in the conventional ARP case, (F) Bone graft placement with complete granulation tissue removal, (G) Socket sealed using a resorbable collagen membrane, (H) Clinical healing at 2 weeks showing partial membrane exposure and delayed soft tissue adaptation.
In this technique, granulation tissue is not left in situ within the socket base, but is carefully elevated and repositioned coronally to function as a biological seal, thereby allowing uninterrupted bone regeneration in the apical and middle portions of the socket. Extraction of the infected tooth typically removes the primary source of inflammation, and in immunocompetent individuals, the remaining reactive tissue is subject to host-mediated immune remodeling. Preservation is performed only when the granulation tissue exhibits favorable macroscopic characteristics, such as firm texture, reddish coloration, active bleeding upon probing, and the absence of necrotic or purulent components. In cases where residual inflammation is suspected, a short course of preoperative antibiotics may be administered to improve tissue quality and minimize the risk of postoperative complications.
Although the technique was demonstrated in an anterior maxillary site, which offers favorable access for flap design and tissue repositioning, it also has high esthetic sensitivity. Complications, such as wound dehiscence, soft tissue contraction, or scarring, could adversely affect the final esthetic outcome. Therefore, this approach should be reserved for cases in which precise surgical control and primary closure can be predictably achieved. An extra-socket incision design (BK incision) may assist in minimizing tension, however, careful patient selection and atraumatic handling are essential, particularly in the esthetic zone.
Nevertheless, intrasocket granulation tissue is not a uniform biological entity and its preservation should not be universally applied without critical evaluation. The cellular composition, inflammatory profile, and regenerative potential of these tissues may vary significantly between sites and patients. As emphasized by Shehabeldin et al., selective preservation based on intraoperative tissue assessment represents a prudent clinical strategy.
This report is limited by its single-case nature and the absence of histological or biological validation, such as biopsy analysis. No quantitative comparisons were made regarding the changes in soft tissue volume or radiographic bone level, and digital overlays were not applied. Although the current case showed successful healing, possible complications, such as persistent inflammation or soft tissue instability, should be considered, especially in high-risk cases. Furthermore, clearly defined clinical indications and contraindications remain to be established. Future controlled clinical studies are needed to validate this biologically oriented approach and determine its long-term efficacy and safety.
Ⅳ. Conclusion
Within the limitations of this case report, our study demonstrated that the intrasocket granulation tissue repositioning technique offers a biologically driven approach to ARP, which is particularly beneficial in periodontally compromised sites. By preserving the intrasocket granulation tissue and utilizing a minimally invasive flap design, this method enables primary closure without additional grafts or membranes. Its potential to enhance soft tissue healing and esthetic outcomes makes it a promising adjunct to implant therapy. Further clinical studies are needed to validate its long-term efficacy and define clear indications for intrasocket granulation tissue preservation.
