

Ⅰ. Introduction
Implant restoration in fully edentulous patients presents a significant clinical challenge in dental treatment. Prosthetic rehabilitation using dental implants in such cases involves a complex treatment process due to anatomical structures, loss of residual dentition, esthetic demands, and the need for occlusal reestablishment. While traditional diagnostic methods and treatment principles have long been the foundation of care, recent advancements in digital technology have integrated with these conventional concepts, compensating for their limitations and enabling clinicians to achieve more efficient, precise, and predictable outcomes.
Conventional approaches often struggle to connect each phase (diagnosis, surgery, and prosthetics), thereby limiting the accuracy and efficiency of the treatment. However, the development of digital technology now simplifies the process—from guided implant surgery to facial scanning, digital facebow transfer, and jaw motion tracking—based on digital diagnostic wax-ups. These technologies enable the fabrication of the final prosthesis in a virtual articulator, resulting in a functionally and esthetically satisfying outcome for the patient.1,2 Additionally, the T-Scan Novus system (Tekscan Inc., Boston, MA, USA) allows qualitative occlusal data to be converted into quantitative data and visualized digitally, providing an accurate assessment of occlusal contact timing and force distribution.3 This enables clinicians to reproduce the desired occlusal state after the final prosthesis delivery.
In this case report, prosthetic restoration using implants was performed in a patient who required the extraction of all teeth except teeth 17 and 47 (Fédération Dentaire Internationale notation) due to periodontal disease. Following evaluation, the existing vertical dimension was preserved, and the implants were placed using a surgical guide fabricated with consideration of the planned position of the final prosthesis. Intraoral and facial scanning, along with jaw motion tracking, were performed, and a monolithic zirconia prosthesis was delivered. Occlusions were analyzed and adjusted using the T-Scan system. As a result, functionally and esthetically satisfactory clinical outcomes were achieved using an efficient treatment approach.
Ⅱ. Case Report
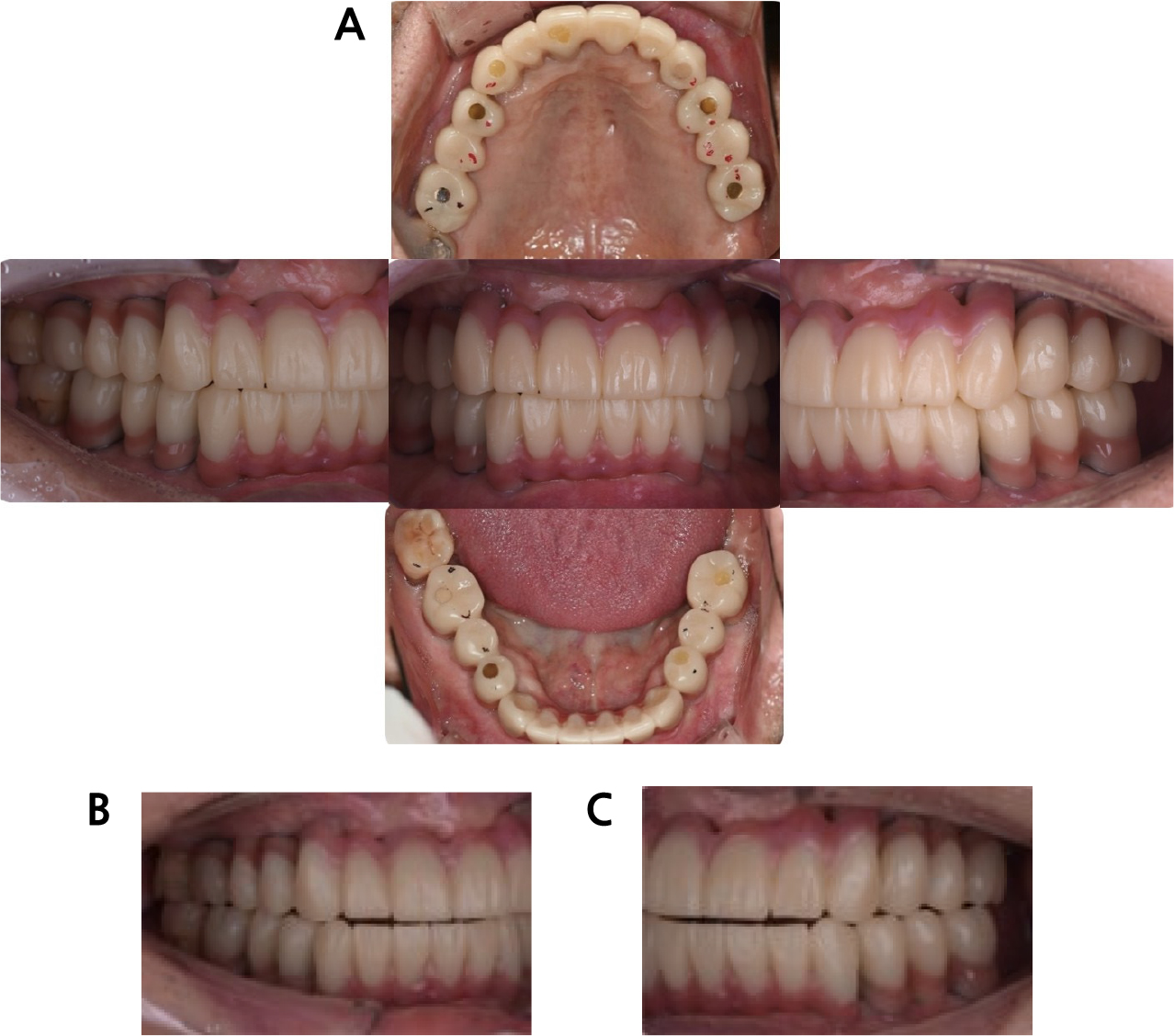
An 80-year-old male patient presented with difficulty eating due to generalized tooth mobility. His medical history included diabetes and a previous colectomy, but he was not taking any medications. Clinical and radiographic examinations revealed alveolar bone loss and Grade III mobility in all maxillary teeth except tooth 17. In the mandible, teeth 31, 32, 41, and 42 were in a hopeless condition with severe mobility, whereas teeth 34, 35, 36, 37, 44, 45, and 46 exhibited Grade II mobility, and tooth 47 showed Grade I mobility (Fig. 1). No specific abnormalities were observed in the temporomandibular joint upon radiographic evaluation.
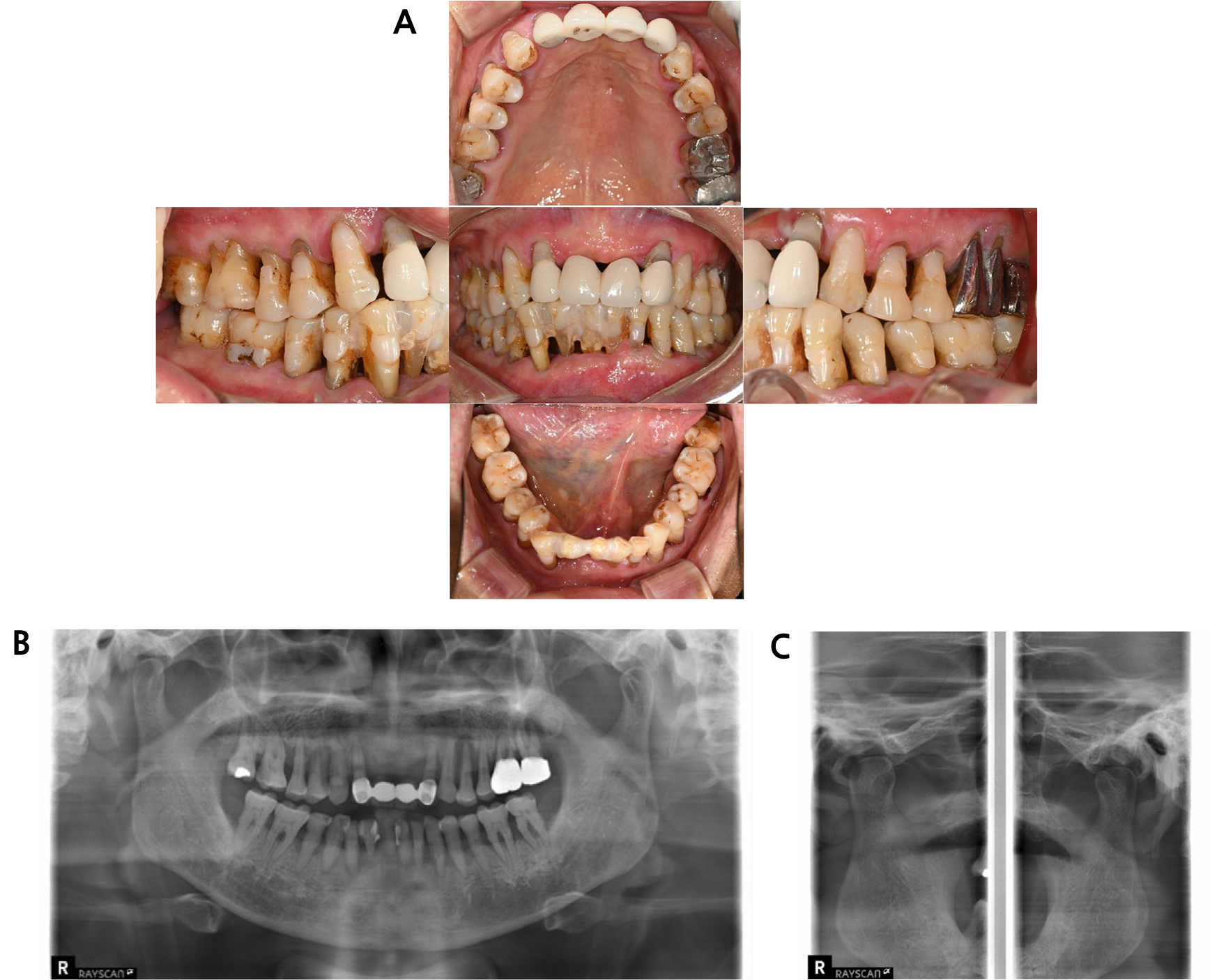
Extraoral facial analysis using the Willis method showed that the middle and lower thirds of the face measured approximately 72 mm, indicating balanced proportions. The difference between the occlusal vertical and rest vertical dimensions was 3.5 mm, which is within the normal range. Although age-related tooth wear was observed, no evidence of pathological wear was found. Therefore, we planned to maintain the existing vertical dimension.4
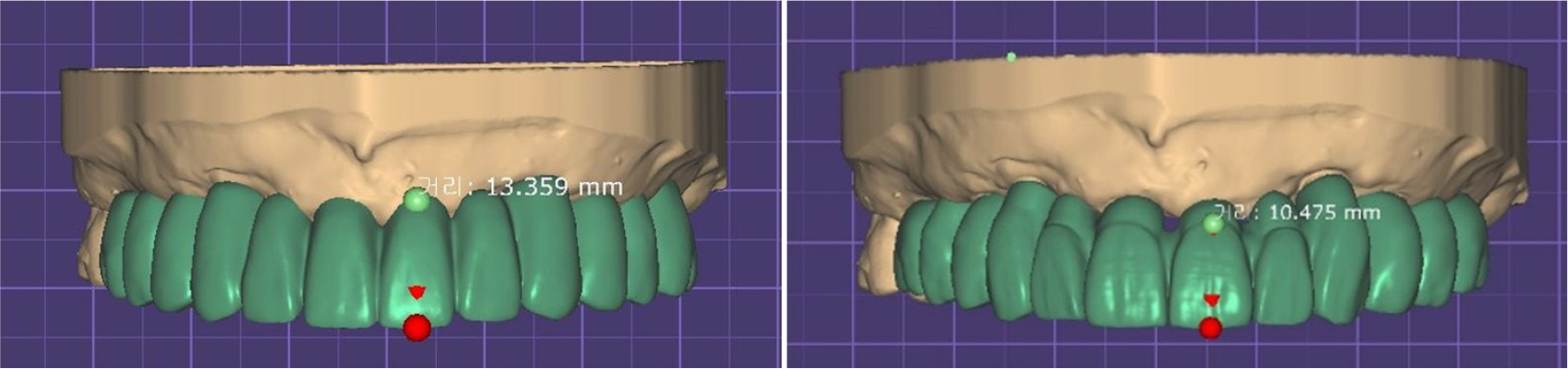
Preliminary impressions were obtained, and diagnostic models were mounted on an articulator (Artex-CR articulator system; Amann Girrbach, Mäder, Austria). A digital diagnostic wax-up was then performed. During the wax-up process, the anticipated length of the anterior and canine regions was approximately 14–15 mm. Considering the average natural tooth length reported in the literature for adult males (maxillary central incisor: 10.19 mm, canine: 10.21 mm), a relatively long crown form was expected. Therefore, a fixed prosthesis–type 3 (FP-3) was planned (Fig. 2).5,6
Although bone loss was observed around teeth 17 and 47, tooth 17 showed no mobility, and tooth 47 exhibited Grade I mobility. These teeth were preserved according to the patient’s preference. Implant placement was planned in the sites of teeth 11, 13, 14, 16, 23, 24, 26, 33, 34, 36, 43, 44, and 46. Considering the occlusal scheme, a bilateral group function occlusion was planned to accommodate the vulnerability of the implants to lateral forces, with centric contacts concentrated on point-centric occlusion.7 For anterior guidance, a mutually protected occlusion was designed to ensure that the posterior teeth would be protected during protrusive movement.
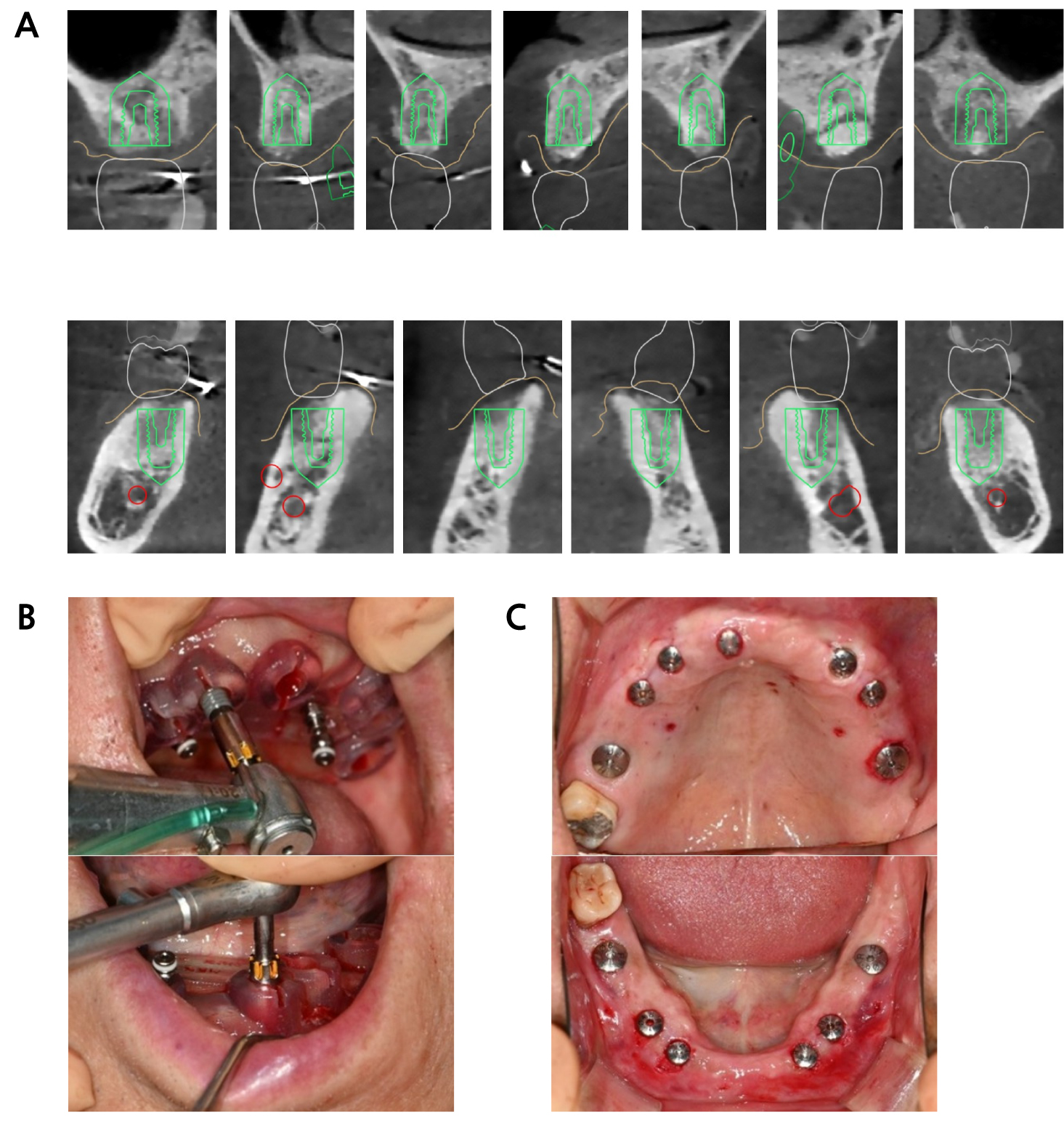
A provisional denture was fabricated while maintaining the original vertical dimension after tooth extraction. Following an adequate healing period, the existing provisional denture was stabilized using a fit-checker for cone beam computed tomography (CBCT) imaging, which is required for guided surgery. Resin balls were attached to the denture as radiopaque markers (Fig. 3). Intraoral scanning was performed, including the intaglio and cameo surfaces of the provisional denture, as well as occlusal registration. A CBCT scan was then performed with the provisional denture in place, and the data were merged. Using implant planning software (3Shape Implant Studio; 3Shape A/S, Copenhagen, Denmark), the implant positions were determined, and a corresponding surgical guide was fabricated (Fig. 4A).
In the maxilla, internal hex connection implants (TSIII SA; Osstem, Seoul, Korea), were placed at the sites of teeth 11, 13, and 23 (diameter 4.0 mm, length 10 mm), teeth 14 and 24 (diameter 4.5 mm, length 10 mm), tooth 16 (diameter 5.0 mm, length 8.5 mm), and tooth 26 (diameter 5.0 mm, length 10 mm). In the mandible, implants were placed at teeth 33 and 43 (diameter 4.0 mm, length 8.5 mm), teeth 34 and 44 (diameter 4.5 mm, length 8.5 mm), and teeth 36 and 46 (diameter 5.0 mm, length 10 mm) (Fig. 4B). Sufficient primary stability was achieved in both arches, allowing for the connection of the healing abutments using a one-stage surgical approach (Fig. 4C).

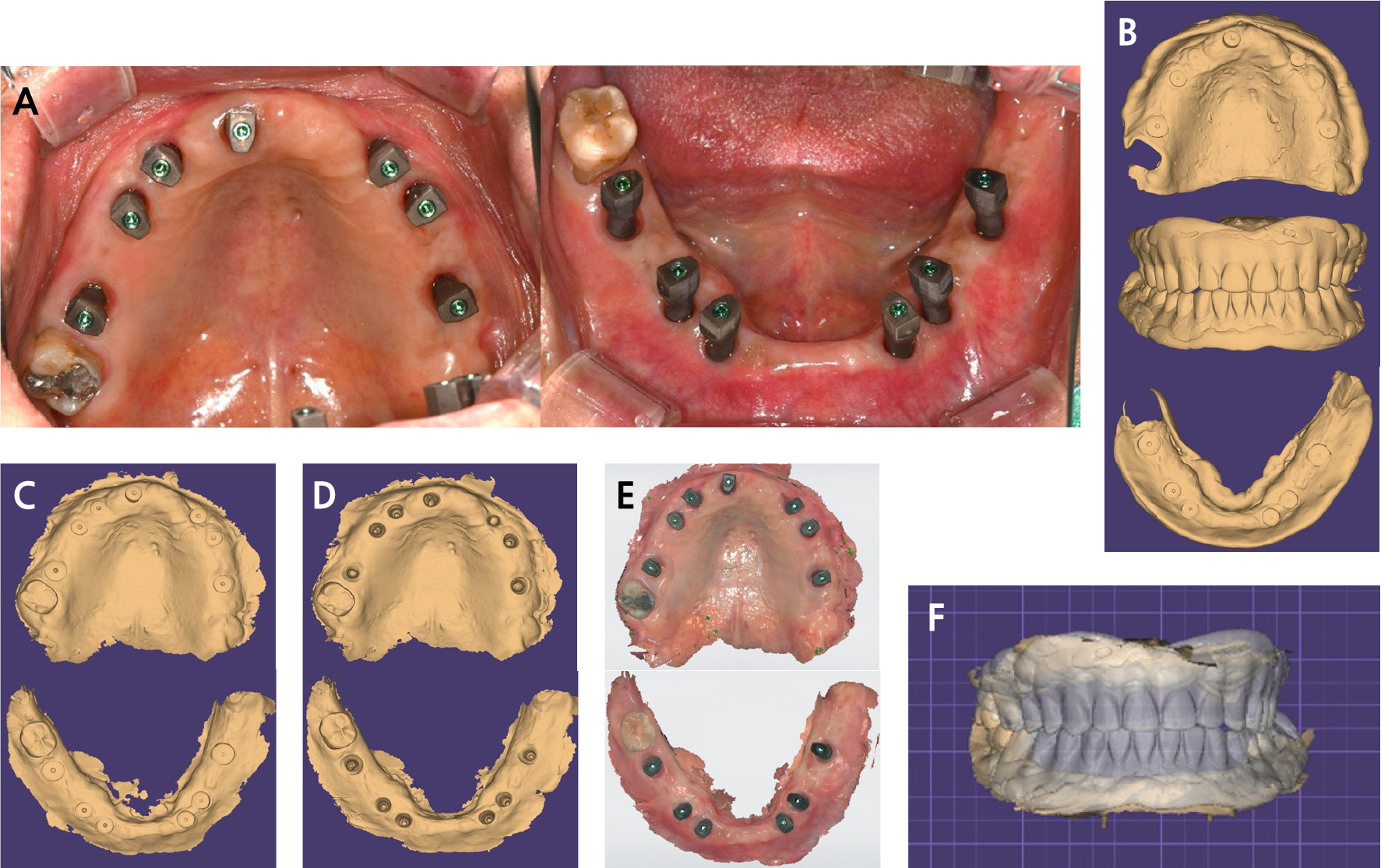
To fabricate a fixed provisional prosthesis, the implant stability quotient was measured, and after confirming sufficient stability, the scan bodies were connected. Maxillary and mandibular implant-level scans were performed using an intraoral scanner (TRIOS 5; 3Shape A/S). To ensure scanning accuracy, adjacent scan bodies were captured simultaneously within the same field of view during acquisition (Fig. 5A).
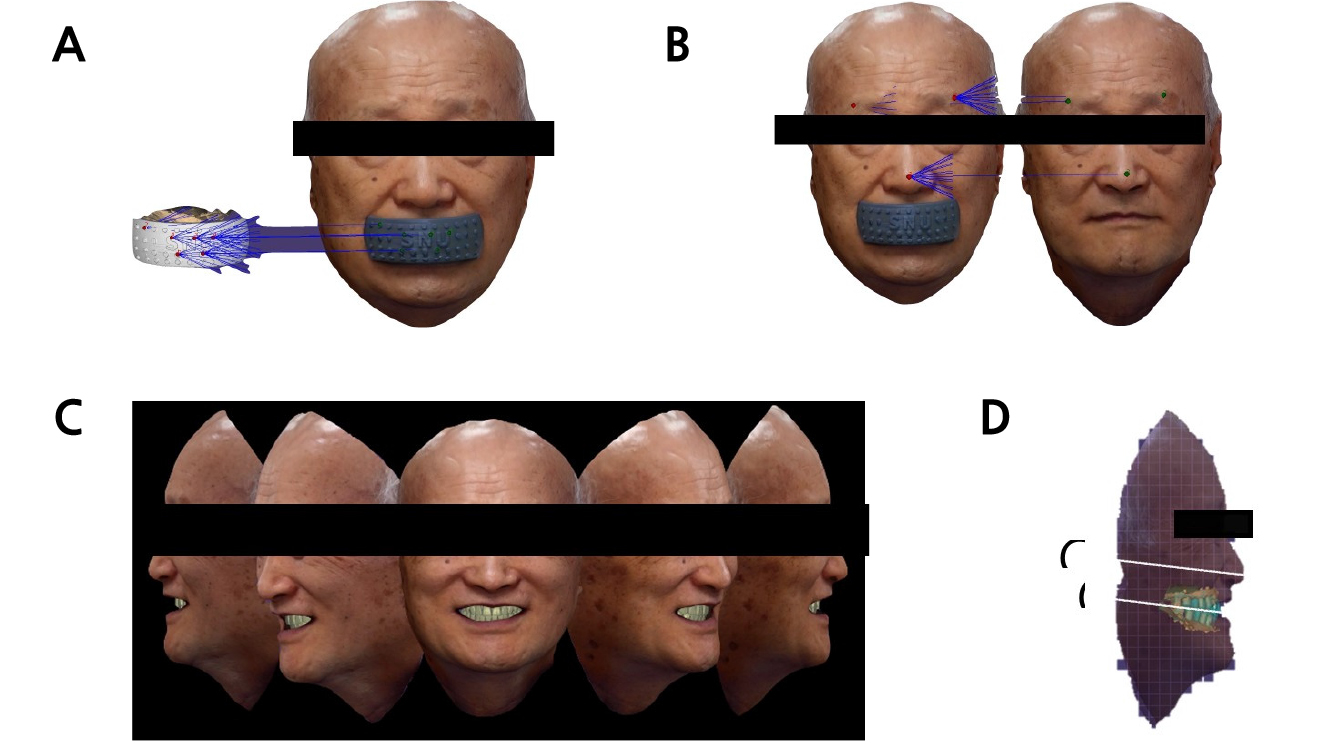
To maintain the vertical dimension of the provisional denture, the intaglio surface and bite registration were captured using a fit-checker material. A pre-preparation scan was performed using the 3Shape TRIOS 5 intraoral scanner, starting with the healing abutment state. Final impressions were obtained after connecting the scan bodies, followed by a facial scan using the Bellus3D ARC system (Bellus3D, Inc., Campbell, CA, USA). The intaglio surface of the denture was aligned with the scan data within the software to preserve the vertical dimension established by the existing provisional denture (Fig. 5B to 5F).
Using the aligned model, the alignment jig used during the facial scan was also aligned with the digital model. With the jig in place, the patient’s face was positioned, and the T-zone was used as a reference to register both relaxed and smiling facial expressions (Fig. 6A and 6B). The horizontal and midline references, as well as the occlusal plane, were verified using the facial scans. In the relaxed facial state, the lip contour was evaluated, and in the smiling view, the amount of anterior tooth display was confirmed (Fig. 6C and 6D).
Based on this information, custom titanium implant abutments and polymethyl methacrylate blocks (Huge Dental Material Co., Ltd., Shanghai, China) were milled to fabricate fixed provisional prostheses, which were divided into three segments—the anterior and bilateral posterior regions—for both the maxilla and mandible. After verifying the bilateral group function occlusion and mutually protected occlusion, the fixed provisional prostheses were delivered (Fig. 7).
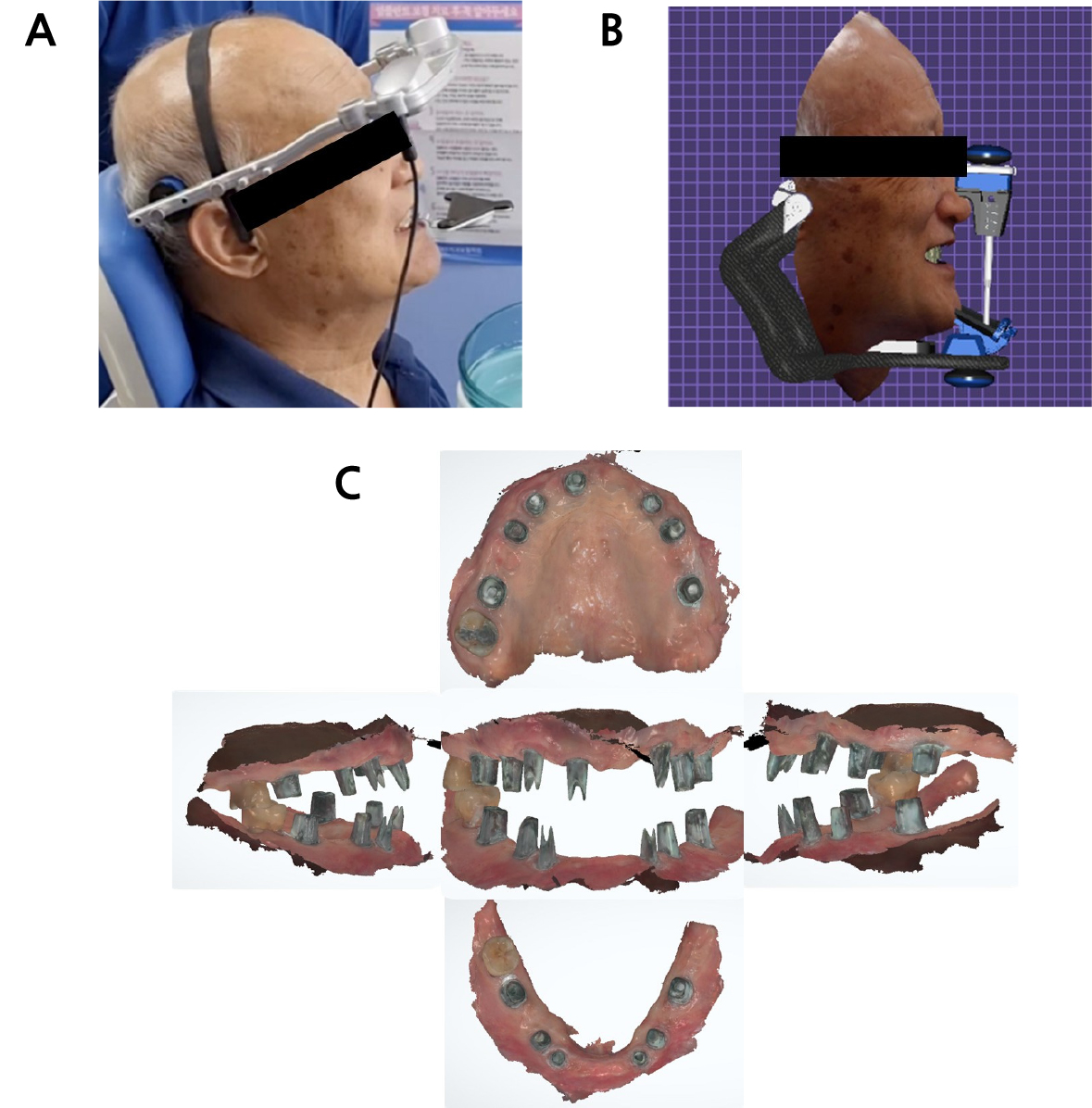
Following approximately 3 months of occlusal stabilization and esthetic evaluation with the fixed provisional prostheses, digital facebow transfer and jaw movement recordings—including opening, protrusive, and lateral movements—were performed using the Zebris jaw motion tracker (Zebris for Ceramill; Amann Girrbach) while the provisional restorations remained in place (Fig. 8A and 8B).
After removing the provisional prostheses, scan spray was applied to the custom titanium implant abutments to enhance scanning accuracy, and an abutment-level impression was taken using the 3Shape TRIOS 5 intraoral scanner (Fig. 8C). Additionally, the gingival shade was recorded to guide the application of pink porcelain.
In the ExoCAD DentalCAD software (v3.1-8200; ExoCAD GmbH Inc., Darmstadt, Germany), the final abutment scan was superimposed with the previously acquired stereolithography file of the custom abutments to verify the abutment margins. Based on the existing fixed provisional prostheses, the data obtained from the Zebris system were used to define the final prosthesis contours and occlusal scheme for the design process.
After designing in the virtual articulator, a model was 3D-printed, and the final zirconia prostheses were fabricated. These prostheses were mounted on a physical Artex articulator with the application of individualized parameters such as the Bennett angle, lateral condylar movement, condylar guidance angle, anterior guidance table angle, and inclination, corresponding to the virtual articulator settings. Functional verification showed that the same lateral and protrusive movements planned in the virtual articulator were accurately reproduced on the physical articulator.
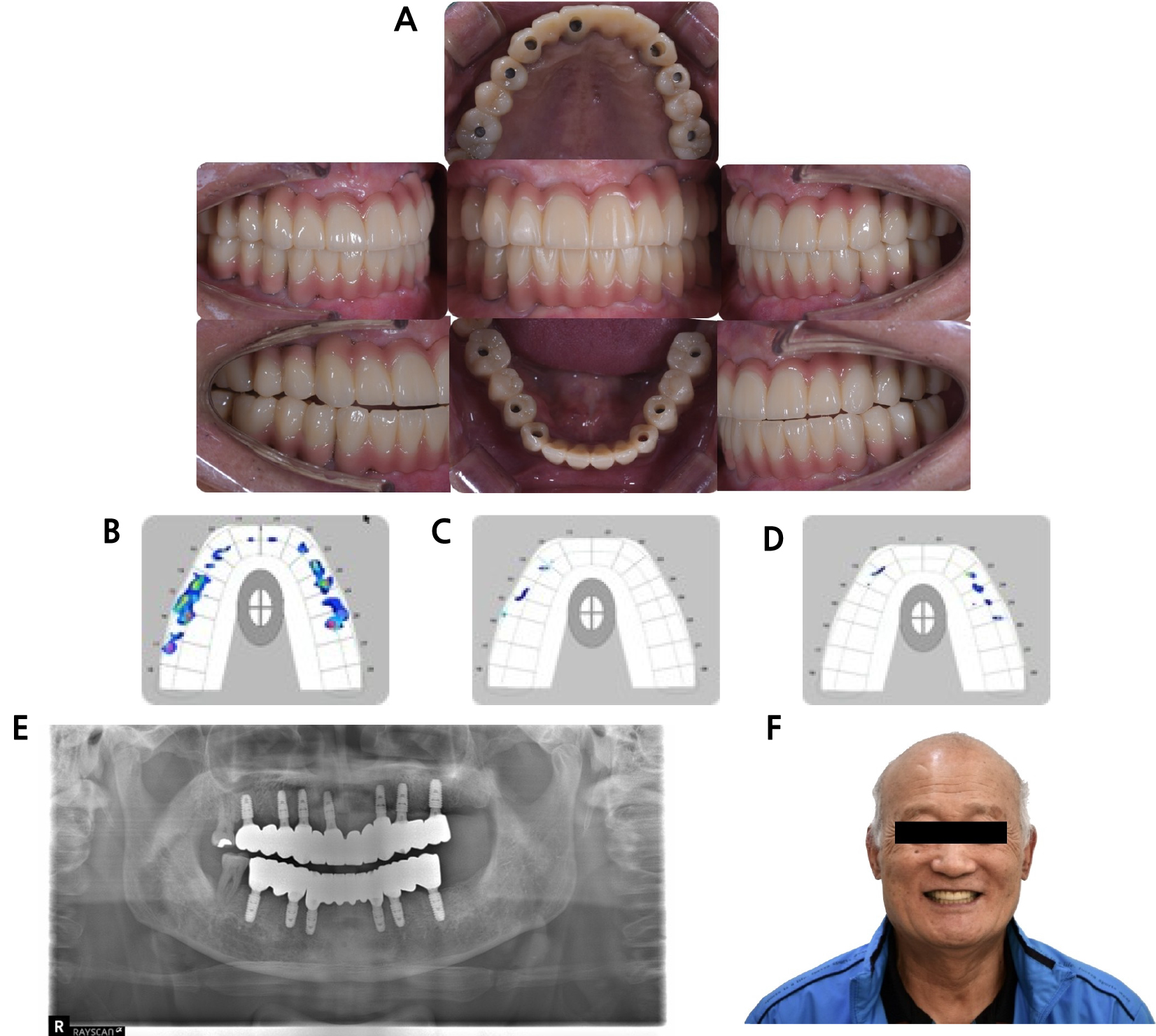
After the intraoral try-in, the intended occlusal scheme was confirmed to be successfully implemented, and the prostheses were definitively cemented. A T-Scan analysis was performed to precisely verify the occlusal contacts, confirming appropriate bilateral group function and mutually protected occlusion (Fig. 9). Following delivery of the final prosthesis, the vertical dimension was confirmed to match the pre-treatment value, and no temporomandibular joint abnormalities were detected during the 1-year follow-up.
III. Discussion
In this case, full-mouth rehabilitation using implants was performed in a patient who required the extraction of all teeth except the maxillary and mandibular right second molars due to severe alveolar bone resorption. A physiologic freeway space of 3.5 mm, normal phonetics, and sufficient restorative space were confirmed, and no pathological tooth wear was observed.4 The patient, who had all teeth present before extraction, wished to receive a fixed restoration and requested to minimize the number of implants due to financial concerns. According to several studies, restoration up to the first molars provides satisfactory masticatory function.8,9,10 Therefore, using a digital diagnostic wax-up, the restoration was designed to extend to the first molars on both sides. The prosthesis was segmented to account for posterior cantilever torque and was designed as an FP-3 prosthesis, reflecting the average natural tooth length.5,6,11
The vertical dimension was determined using a provisional denture and was maintained throughout the implant prosthetic phase after an adaptation period. Recent studies have reported that full-arch implant impressions taken with intraoral scanners show no significant difference compared to conventional methods and are clinically applicable.12 Accordingly, a full-arch implant impression was taken using an intraoral scanner, and a facial scanner was used to reference the patient’s facial structure during prosthesis design. Conventional methods have several limitations, such as the risk of cast damage and difficulties in reusing previous casts. In contrast, digital impression techniques provide advantages in reproducing previous conditions. Using facial scans, the midline, occlusal plane, and horizontal alignment could be reassessed even in the dental laboratory, thereby reducing errors compared to setting the midline and occlusal plane using conventional methods. After a sufficient stabilization period with the provisional prosthesis, jaw motion tracking was employed in the final prosthesis phase to establish the intended occlusion.13,14 As implants lack a periodontal ligament, improper occlusion can lead to failure.15 Additionally, because implants are vulnerable to lateral forces, the occlusion was designed to prevent excessive lateral load on the posterior implants while harmonizing with the patient’s mandibular movements.7
Ultimately, the final prostheses were fabricated as monolithic zirconia screw- and cement-retained prosthesis restorations, allowing for retrievability.16,17 Digital workflows encompassing diagnostic wax-up, implant position planning, and occlusal design enabled the achievement of excellent esthetics and function with minimal adjustment of the final prosthesis. The advantages of the digital approach have evolved from conventional methods, and incorporating traditional reference points provides a means to simplify the process. Integrating the two approaches enhances overall harmony and ultimately leads to improved outcomes.
IV. Conclusion
A comprehensive diagnosis and treatment plan were established using a digital wax-up, followed by the fabrication of a surgical guide for implant placement through a top-down approach. The vertical dimension was accurately preserved using digital technology, and complete implant impressions were obtained with an intraoral scanner. Facial scanning was conducted to determine the horizontal reference, midline, anterior tooth display, and occlusal planes. Furthermore, jaw motion tracking was applied to incorporate the patient’s mandibular movements into the final occlusal scheme. This integrated approach enabled precise determination of esthetic parameters and occlusal planes, as well as the establishment of a planned group function and mutually protected occlusion. The combination of digital technologies yielded functionally stable and esthetically satisfactory clinical outcomes.
