

Ⅰ. Introduction
Several studies have investigated the factors related to peri-implant health. Among these, the role of peri-implant keratinized mucosa (PIKM) has recently been highlighted. Despite the heterogeneity among the studies,1 recent study tended to advocate the necessity of PIKM. These studies showed that a lack of PIKM was associated with a high plaque index, mucosal inflammation, mucosal recession, brushing discomfort, inflammatory biomarkers, and marginal bone loss.2,3,4,5
Various surgical modalities can be used to establish the PIKM.6 Among them, autogenous tissue transplantation, that is, free gingival graft (FGG), is considered a standard-of-care modality.6 The effect of FGG on peri-implant health has been verified in several retrospective observational studies. Even in serial randomized clinical trials, less marginal bone loss and reduced mucosal recession were demonstrated in FGG-treated implant sites compared to those lacking PIKM.7,8
One of the clinical interest in FGG is the shrinkage that occurs after augmentation. Depending on the shrinkage rate, the clinician may determine the amount of graft required to achieve a minimum optimal PIKM (e.g., 2 mm) for peri-implant health. However, most studies were limited to short-term follow-up (≤1 year),9 with up to 62% of shrinkage rate in such a period.10,11,12,13,14 Only a few studies included long-term data (≥5 years). In a study by Schmitt et al. (2016), the shrinkage of the augmented PIKM was 41% in the anterior mandible at 5 years post-FGG.15 Recently, Chen et al. (2023) reported a 30% shrinkage rate in the posterior areas at 13 years, although the follow-up loss was significant.16
Another interesting finding is the site-specific outcomes after FGG. The distal mandibular area often poses anatomical challenges such as shallow vestibular depth, proximity to the external oblique ridge, and the attachment of the buccinator muscle. In one clinical study, these factors were suspected to contribute to less PIKM zone formation in the mandibular second molar area than in the first molar area.17 Moreover, the recreated PIKM in an area with anatomical limitations may not be as stable as that without (in other words, prone to shrinking) in the long term.
This case study aimed to report the long-term changes (≥20 years) of FGG in the posterior mandible.
Ⅱ. Case Report
Three patients received implant treatment (three consecutive implants for each patient; the distal one: Id, the center one: Ic, the mesial one: Im) in the first and second mandibular molar areas ≥20 years ago. These patients received three external-type implants in two mandibular molar-missing areas that lacked keratinized tissue. The decision regarding the number of implants followed the concept of implant treatment that had been previously used.18,19 Bone augmentation was not performed in any of the patients. After the insertion of the final prosthesis, all patients were asked to visit the clinic regularly; however, appointments were not strictly maintained. The demographic information and details of the implants are provided in Table 1.
Table 1.
Demographic and implant-related information of three patients
1. Case 1
A 38-year-old non-smoking male patient required dental implant treatment to restore the edentulous posterior mandibular area on the right side. Three smooth-surface, external-type implants (3i implant; Biomet 3i, Palm Beach Gardens, United States) were placed (Id: Ø4.0 × 11.5 mm, Ic: Ø4.0 × 11.5 mm, Im: Ø4.0 × 11.5 mm). Due to the lack of keratinized mucosa and vestibule, FGG was performed before inserting the final prosthesis. Following local anesthesia, a partial-thickness flap was prepared on the buccal side of the implants to form a periosteal bed. Then, a free epithelialized gingival graft with a 1.0–1.5 mm thickness was harvested from the ipsilateral palate and secured onto the periosteal bed with sutures. Antibiotics and analgesics were prescribed for 7 days. The final prostheses were delivered 2 months later.
In the early follow-up period, bone remodeling was more pronounced in the Ic. During the follow-up period, peri-implant mucositis developed in the Id and Ic, and peri-implantitis in the Im. These peri-implant diseases are treated surgically. At 20 years, implant fracture occurred in the Im, and it was replaced with another implant (Superline Ø4.8 × 10 mm; Dentium, Seoul, Korea).
During follow-up, the PIKM height was measured using a periodontal probe along the mid-buccal area of each implant crown. The measurements were rounded to the nearest millimeter. The measurement method was the same for all patients in this case study. The height of the PIKM in Im and Ic increased slightly between 1 and 17 years of follow-up, indicating creeping attachment. However, the height of the PIKM in the Ic group markedly decreased between the ages of 17 years (8 mm) and 27 years (2 mm). In the Id, the PIKM continuously decreased over the follow-up period and reached zero at 27 years (‒3 mm) (Fig. 1 and Table 2).
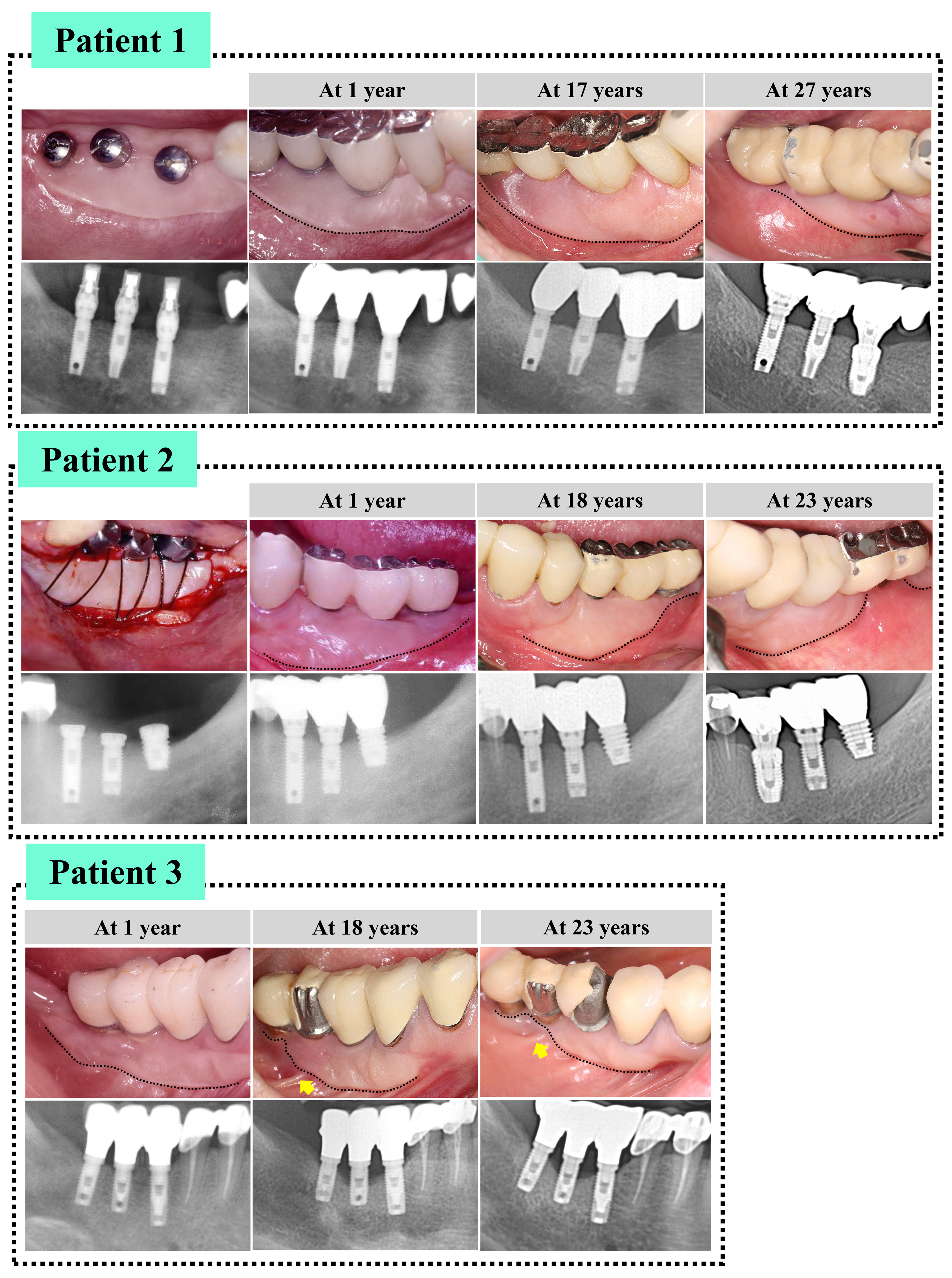
Table 2.
Apico-coronal height of peri-implant keratinized tissue, measured at mid-buccal area (in mm)
| Patient 1 | |||
| Im | Ic | Id | |
| 1 year | 4 | 7 | 3 |
| 17 years | 6 | 8 | 1 |
| 27 years | 5 | 2 | 0 |
| Patient 2 | |||
| 1 year | 10 | 6 | 4 |
| 18 years | 10 | 6 | 1 |
| 23 years | 9 | 5 | 0 |
| Patient 3 | |||
| 1 year | 6 | 5 | 4 |
| 16 years | 6 | 5 | 0 |
| 20 years | 4 | 0 | 0 |
Three implants were placed in the first and second molars. Implants in the distal area: Id; center: Ic; mesial area: Im
2. Case 2
A 50-year-old male with a smoking habit sought dental implant treatment in the left posterior mandibular area. Three smooth-surface, external-type implants (3i implant, Biomet 3i) were placed (Id: Ø5.0 × 8 mm, Ic: Ø3.75 × 10 mm, Im: Ø3.75 × 13 mm). The threaded part of the Id was not fully embedded in the bone due to the unavailability of a commercial short implant and the proximity of the inferior alveolar nerve. Keratinized augmentation using the FGG was performed simultaneously with connecting the abutments.
After 18 years, signs of peri-implantitis were observed in the Id. Nonsurgical treatment was applied to the implant. At 20 years of follow-up, implant fracture was observed in the Im. The implant prosthesis was cut at the junction between the crowns of Im and Ic, followed by the placement of the new implant in a larger diameter (Superline Ø4.8 × 10 mm, Dentium). The cut surfaces of the remaining implant prostheses were polished. After 3 months, the implant crown was delivered to the newly placed Im.
The height of the PIKM remained stable at Im and Ic for 23 years. However, in the Id, a pronounced reduction in PIKM was observed during follow-up, and the height of the PIKM became 0 at 23 years (‒4 mm) (Fig. 1 and Table 2).
3. Case 3
A 36-year-old, non-smoking female patient requested dental implant treatment in the right posterior mandibular area. Three smooth-surface, external-type implants (Steri-Oss; Steri-Oss Inc., Yorba Linda, United States) were placed (Id: Ø3.8 × 10 mm, Ic: Ø3.8 × 10 mm, Im: Ø3.8 × 12 mm). FGG was performed before the final prosthesis delivery.
The Ic showed pronounced bone remodeling and eventually developed peri-implantitis. Peri-implant mucositis was observed in the Id. Similar to patients 1 and 2, nonsurgical treatment was performed for Ic and Id.
The PIKM height in Im was relatively stable during the follow-up period. However, the Ic and Id showed a whole loss of PIKM between 16 years and 20 years (‒5 mm) and between 1 year and 16 years (‒4 mm), respectively (Fig. 1 and Table 2).
Ⅲ. Discussion
The current cases present a different stability of the re-established PIKM at the distal part of the posterior mandible than at the mesial part. Over 20 years of follow-up, some implants underwent unfavorable bone remodeling and peri-implant diseases, which are confounding factors that contribute to the weak stability of the FGG at the distal part. However, the pattern of the reduction of the re-established PIKM was peculiar; the reduction was mostly in the coronal direction.
The site-specific stability of the re-established PIKM has been documented in a few studies. In one clinical study on FGG outcomes in the posterior mandible, the second molar area exhibited a smaller amount of re-established PIKM and greater shrinkage over 3 years of follow-up. In this study, the reduction rate was 49 ± 24% in the first molar area and 66 ± 19% in the second molar area between immediately after the PIKM augmentation and 3 years later.17 Following explanation can be made for such different behaviors of FGG: the second molar area is 1) initially related to the shallow vestibule, 2) close to the external oblique ridge, limiting the available space for the graft, 3) susceptible to buccinator muscle re-attachment, and 4) not supported by the natural tooth in the distal area. In a preclinical study, frenular attachment affected the number of re-established PIKM, which partially supports the effect of muscle attachment.20
After FGG, most of the dimensional reduction occurred within 6 months, and the re-established PIKM stabilized afterward.16 Such observations seem to be true for most sites. However, in long-term observations, a gradual and consequently significant loss of the re-established PIKM can be observed at the most distal part of the mandible for the reasons mentioned above. In the study by Fu et al., approximately a 10% reduction was reported in the second molar area between 6 months and 3 years,17 which might not be negligible. If this reduction tendency persists, the long-term result could be a total loss of the re-established PIKM, as shown in the Id of patient 1.
As implants remain in the oral cavity for a long time, the risk of peri-implant diseases may increase with age. Peri-implant inflammation can affect PIKM adherence. An increased probing depth is a common finding in peri-implant diseases. If the peri-implant probing depth is 5 mm and the PIKM is 3 mm, the PIKM can be regarded as non-adherent (or not attached). Considering the orientation of the peri-implant connective tissue (running parallel to the abutment surface),21 genuinely attached PIKM can be confirmed when the mucogingival junction is apical to the bone crest. However, peri-implantitis negatively affects bone levels; thus, PIKM previously attached (to the bone) may change to non-attached PIKM.22 The unattached PIKM plays a role in interpreting the PIKM reduction in the coronal direction. The attached PIKM probably withstood the harmful influence of the neighboring soft tissues (thick cheek tissue, buccinator muscle, and frenum). However, unattached PIKM might be vulnerable, especially in the distal part of the posterior mandible, and the PIKM zone is invaded by non-keratinized mucosa.
The same explanation can be applied to the Id of Patient 3. After 1 year, bone remodeling was evident in the implant. Considering the bone level and PIKM height, the PIKM was unlikely to be attached to the bone. Supracrestal exposure of the implant threads contributed to mucosal recession and peri-implant inflammation. However, the pattern of PIKM reduction included shrinkage in the coronal direction.
A contrasting phenomenon was observed in the Ic and Im values of patient 1. The PIKM increased coronally throughout follow-up for these implants. This phenomenon is known as “creeping attachment” and is reported sporadically. The factors that induce creeping attachment at implant sites have not yet been clarified.23,24
Ⅳ. Conclusion
The case report showed an unstable tendency to re-establish the PIKM in the distal area of the posterior mandible compared to the other parts. However, these results were based on only a small number of patients and should be interpreted cautiously, considering potential confounders such as peri-implant diseases and bone remodeling. Moreover, site specificity in terms of PIKM stability should be further verified in healthy implants.
