

Ⅰ. Introduction
When placing implants in the posterior maxilla, maxillary sinus floor elevation via the crestal or lateral window is a well-documented surgical method to manage limited alveolar bone height.1 Sinus augmentation is the most predictable regenerative surgery among the guided bone regeneration methods, with a reportedly high implant survival rate.2 To determine the appropriate surgical approach, dentists generally perform cone-beam computed tomography (CBCT) before sinus augmentation surgery to evaluate the alveolar bone height and detect pathologies of the maxillary sinus. Checking the normal anatomy and physiology of the maxillary sinus is essential before implant placement in the posterior maxillary region. Notably, sinus pathologies observed on CBCT in dental patients are quite common, with an incidence >50%, and their presence increases the difficulty in performing sinus augmentation surgery.3,4
Unlike panoramic radiographs, where the anatomic structures overlap in the two-dimensional image, CBCT provides a direct view of the sinus mucosal membrane and ostium in a detailed three-dimensional scan. Increased use of CBCT by dentists and maxillofacial surgeons helps analyze the prevalence of incidental pathological findings of the maxillary sinus. Moreover, studies have attempted to identify and eliminate the possible risk factors before sinus floor elevation.5 As taking CBCT is recommended before sinus elevation surgery to detect anatomic variations and pathologic findings, the role of dentists in identifying maxillary sinus diseases and making necessary referrals to otolaryngologists has become important.6,7
When treating maxillary sinus diseases, otolaryngologists first consider conservative treatment, such as prescribing antibiotics, anti-inflammatory drugs, or nasal decongestants. Surgical treatment is considered when medication therapy is ineffective or excision of the lesions is necessary. The Caldwell–Luc procedure is a conventional surgical approach for complete resection of the lesions and underlying sinus mucosal lining. However, it has several limitations, including impaired sinus physiology as the mucociliary lining is replaced by non-functional mucosa postoperatively.8 Additionally, intraoperative and postoperative complications, including bleeding and infraorbital nerve damage often occur. Currently, endoscopic sinus surgery (ESS), a less invasive approach, is the standard surgical treatment. The physiologic function of the sinus membrane is restored via ESS by curetting and opening the stenosed osteomeatal complex using an endoscopic microdebrider.9
Sinus neoplasms are rare in the broad spectrum of maxillary sinus diseases;10 however, their management may be challenging if they become malignant. Inverted papilloma is the most common neoplasm of the sinus cavity. Although benign, it has the potential to become malignant, and an association between inverted papilloma and squamous cell carcinoma has been reported.11 The current standard treatment is ESS; however, the Caldwell–Luc procedure can be adopted alone or with ESS, depending on the tumor extent and its characteristics.12
This case report describes implant placement with sinus floor elevation after endoscopic removal of an inverted papilloma, a sinus neoplasm, in the otolaryngology department.
Ⅱ. Case Report
A 52-year-old woman requiring implant placement in the right maxillary posterior edentulous area visited Seoul National University Dental Hospital in November 2020. The maxillary second premolar and first and second molars were missing. As atrophy of the alveolar bone was anticipated and pneumatization of the maxillary sinus was observed on panoramic radiography, CBCT was taken to determine the surgical approach for sinus floor elevation.
The CBCT scans revealed radiolucency indicative of a tumor near the sinus ostium, impeding normal sinus drainage, with irregular thickening of the Schneiderian membrane (Fig. 1). Dome-shaped and cyst-like opacity of the antral pseudocyst is a frequent finding in the maxillary sinus, and it is not a contraindication for sinus augmentation.13 However, the irregular contour observed on the CBCT appeared different from that of an antral pseudocyst. Although there was no facial discomfort or nasal congestion, the patient was referred to an otolaryngologist before sinus augmentation.
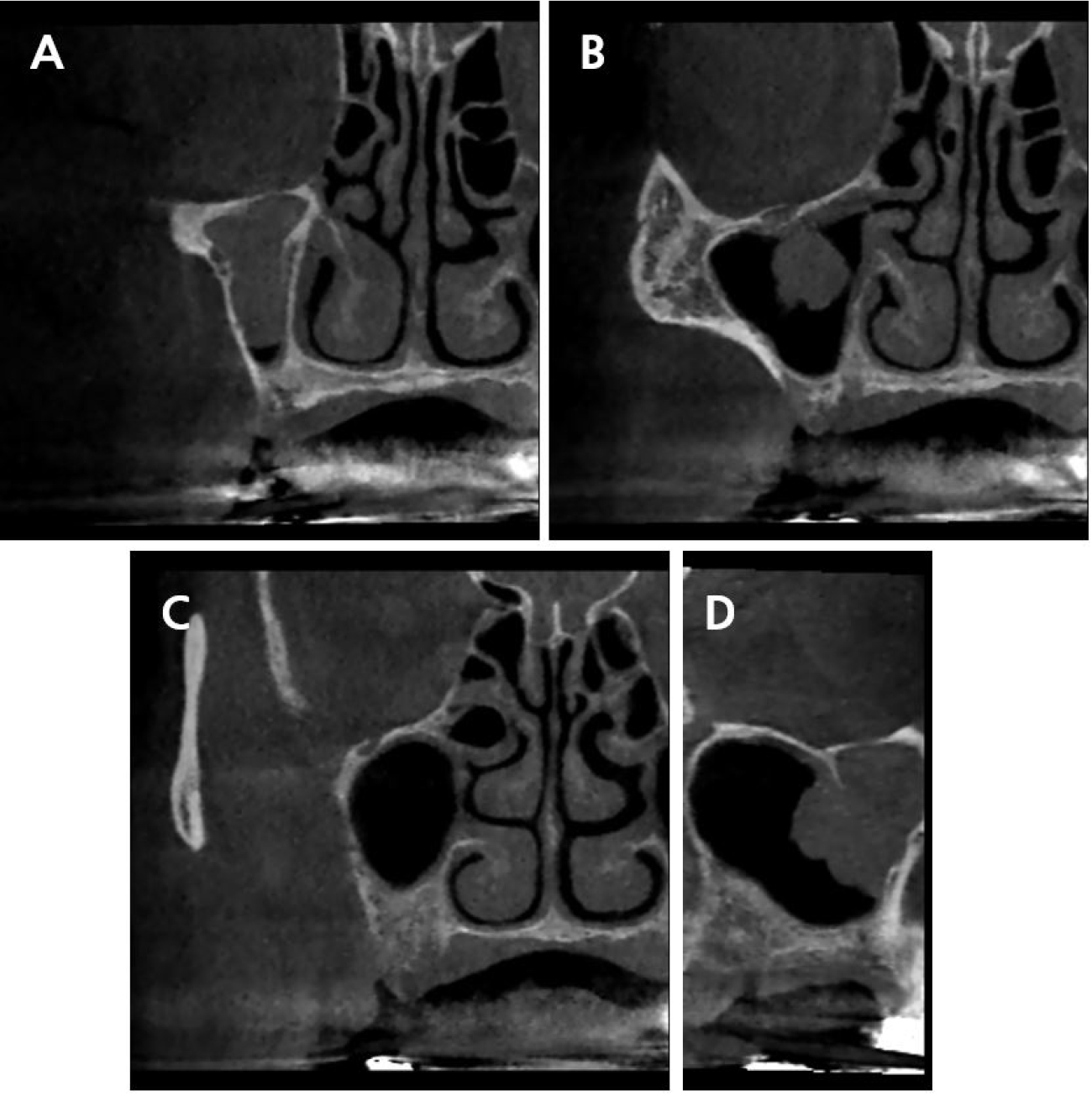
Fig. 1.
Cone-beam computed tomographic images of the pathologic findings of the right maxillary sinus suggestive of inverted papilloma. (A) Cross-sectional view of the maxillary second premolar region, (B) Cross-sectional view of the maxillary first molar region, (C) Cross-sectional view of the maxillary second molar region, (D) Sagittal view.
The patient had initially visited a local otolaryngologist. However, she was referred again to the otolaryngology department at our hospital for excisional biopsy. The biopsy results indicated an inverted papilloma, which is a precancerous lesion; hence, surgical removal under general anesthesia was scheduled at the otolaryngology department in February 2021. ESS was performed to remove the sinus lesion.
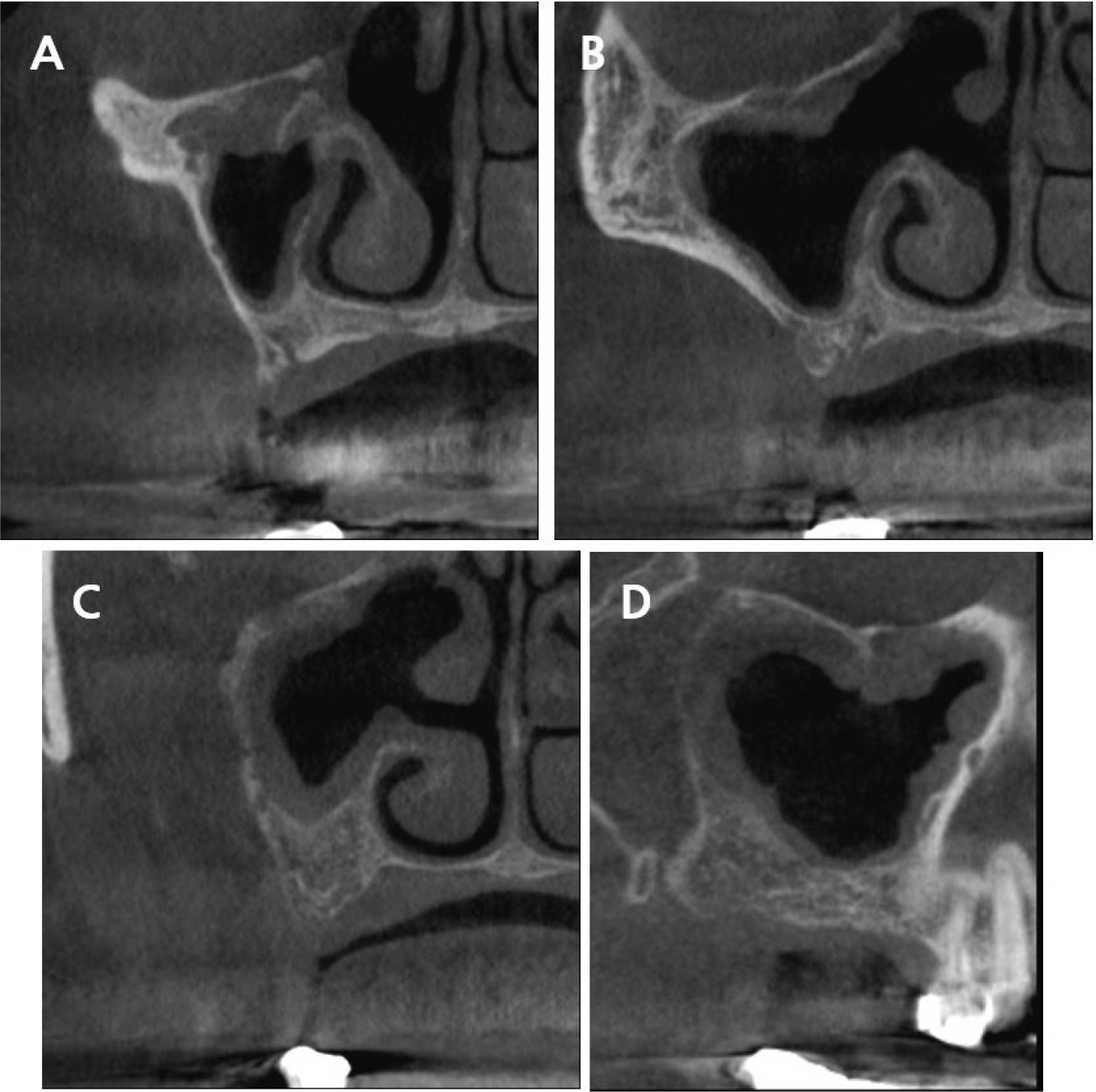
After several months of follow-up, the patient was called to place implants in the posterior maxilla in June 2021. CBCT was performed and complete tumor removal was confirmed (Fig. 2). Furthermore, dissection of part of the sinonasal structures and generalized mucosal thickening along the sinus wall were observed. Since the neoplasm was removed by ESS and not the Caldwell–Luc method, the otolaryngology department observed that dental surgery could be performed without any specific precautions. However, regular check-ups were necessary, and surgical re-entry would be required if the inverted papilloma recurred.
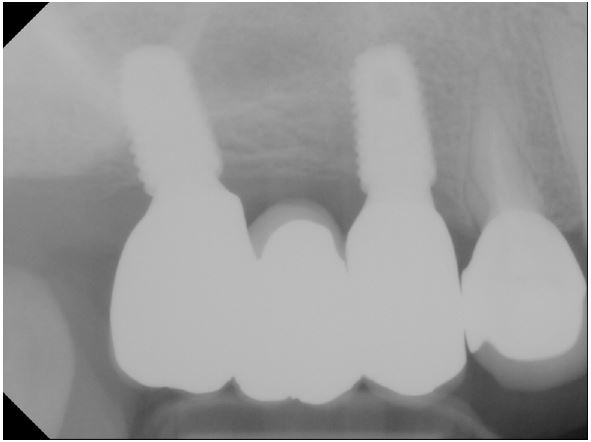
Implant placement with sinus floor elevation was conducted approximately 6 months after ESS. Because of the mucosal thickening observed after the otolaryngologic surgery and possibility of inverted papilloma recurrence, two implants instead of three were placed in the maxillary second premolar and second molar sites, respectively, to simplify and minimize the dental surgery. Implant placement in the first molar region was omitted, because the residual bone height was <4 mm and would need a lateral window technique with graft materials for sinus floor elevation. The osteotome technique without grafting materials was used, and short implants of length 8.5 mm were placed in the second premolar and second molar areas (TS III 4.5 × 8.5 mm and 5.0 × 8.5 mm; OSSTEM, Seoul, Korea). Both implants were placed with sufficient initial stability, and the patient did not report any postoperative discomfort.
The final implant prosthesis was inserted in April 2022 in the prosthodontics department (Figs. 3 and 4). The patient underwent regular check-ups in the periodontology and prosthodontics departments, and no complications were reported. The patient also visited the otolaryngology department every 6 months to check for recurrence.

Ⅲ. Discussion
Various sinus pathologies are observed on CBCT, including mucosal thickening, mucous retention cyst or antral pseudocyst, sinus polyps, and air-fluid level, as well as malignancies, which is rarely observed.14 Although there is no clear criterion regarding referring cases to otolaryngologists, some pathological findings need postponing of dental surgery and preoperative otolaryngologic treatment. Dentists should assess the eligibility of the case for sinus augmentation thoroughly, because some untreated sinus pathologies negatively affect the sinus augmentation outcomes and implant survival. Appropriate treatment of preexisting diseases is essential to reduce the risk of sinus membrane perforation and postoperative complications.15
Mucosal thickening is the most frequent finding in the maxillary sinus, followed by mucous retention cysts, which appear as dome-shaped opacities. These are not considered contraindications for sinus surgery, unless the physiology of the maxillary sinus is affected.16 However, caution is needed when the sinus ostium loses patency or when tumor-like membrane thickening is observed. Tumors or neoplasms of the maxillary sinus are often asymptomatic, making it difficult to detect them. They are usually found when patients complain of symptoms only after the adjacent structures have been destroyed.10
Although inverted papilloma of the paranasal sinus is a benign tumor, it has aggressive characteristics, such as a tendency for recurrence and potential for malignant transformation. It is important to distinguish between inverted papilloma and common inflammatory sinusitis because both present increased membrane thickness on CBCT.17 The final diagnosis is determined by histologic examination of the biopsy samples obtained via nasal endoscopy. While pharmacotherapy is the primary treatment for inflammatory sinus diseases, such as chronic or acute rhinosinusitis and odontogenic sinusitis, inverted papilloma requires surgical removal. The significant factors in the selection of the appropriate surgical method are the extent and location of the inverted papilloma. ESS is the primary treatment, unless the neoplasm is too extensive to be visualized endoscopically or shows bone destruction or malignancy.12
To our knowledge, this is the first case report in which the implants were placed with sinus floor elevation after ESS was performed for a sinus neoplasm. Implant placement was postponed during the healing and follow-up periods postoperatively.18 Despite the delayed treatment schedule, CBCT showed homogenous membrane thickening. Membrane perforation during sinus elevation is a valid concern, because the maxillary sinus membrane is not completely healthy.19 If perforation occurs, leakage of graft materials into the sinus cavity could lead to infection, especially in patients with impaired ostium patency or an unhealthy sinus membrane. Therefore, we adopted the osteotome technique without graft materials rather than the lateral approach for sinus membrane elevation. Surgical treatment was completed by placing short implants simultaneously.
Ⅳ. Conclusion
Before placing implants with sinus floor elevation in the posterior maxilla, it is essential to evaluate the anatomical and physiological status of the maxillary sinus and consult an otolaryngologist, if preoperative treatment is deemed necessary. Dentists can detect pathologic changes in the maxillary sinus in the early stages using CBCT, an advanced device that illustrates sinonasal conditions precisely.
