

Ⅰ. Introduction
Adequate alveolar bone volume and quality are essential when placing dental implants. However, horizontal ridge deficiencies commonly arise following tooth loss due to physiological remodeling.1To overcome this insufficiency, clinicians consider augmentation procedures such as guided bone regeneration (GBR), block bone grafting, and alveolar ridge splitting.
Among these solutions, modified alveolar ridge splitting offers several advantages, including reduced overall treatment time, simultaneous implant placement, and simplified bone grafting due to the creation of a contained defect.
In 1986, Tatum introduced the core concept of ridge splitting as a method to widen a narrow alveolar ridge.2 Since then, this technique has been widely adopted by clinicians. The technique leverages the elastic nature of the alveolar bone to displace the buccal plate, thereby expanding the width of the atrophic ridge. This displacement creates adequate space for implant placement. This concept is based on a controlled greenstick fracture without complete detachment, which preserves vascularity and maintains periosteal attachment.
Despite its benefits, the ridge-splitting technique requires careful case selection and precise surgical execution to minimize complications such as buccal plate fracture. Consequently, some practitioners remain reluctant to utilize this approach.
To mitigate the risk of buccal plate fracture, the present case series describes an adapted splitting technique in which the buccal plate is stabilized using metal fixation miniplates and miniscrews. The procedure begins with the creation of complete vertical and sagittal osteotomies, followed by an intermittent horizontal osteotomy that does not fully separate the cortical bone. Piezoelectric surgical inserts are subsequently used to prepare the sites for miniplate and miniscrew placement (Fig. 1). The fixation devices are then secured to permit gradual, controlled expansion of the alveolar ridge, thereby further reducing the risk of buccal cortical plate fracture (Fig. 2).
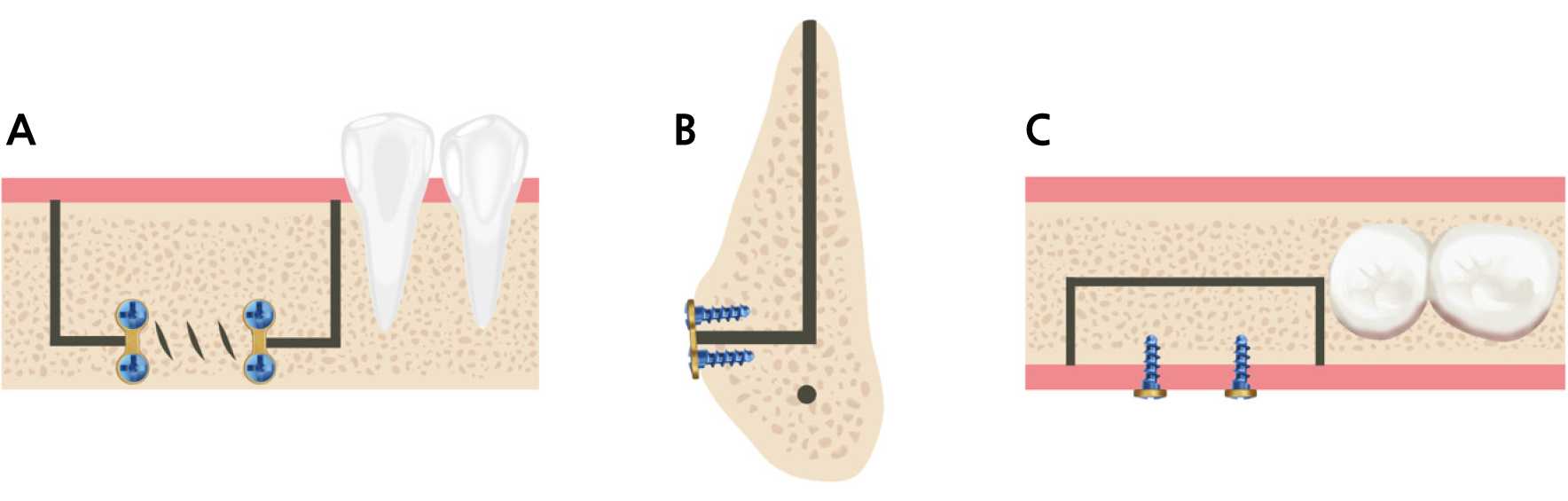
Fig. 1.
Diagram illustrating the modified alveolar ridge-splitting technique. (A) Complete vertical and sagittal osteotomies, followed by an intermittent horizontal osteotomy without complete cortical separation, (B) Coronal view of the osteotomies and miniplate and miniscrew placement, (C) Occlusal view.
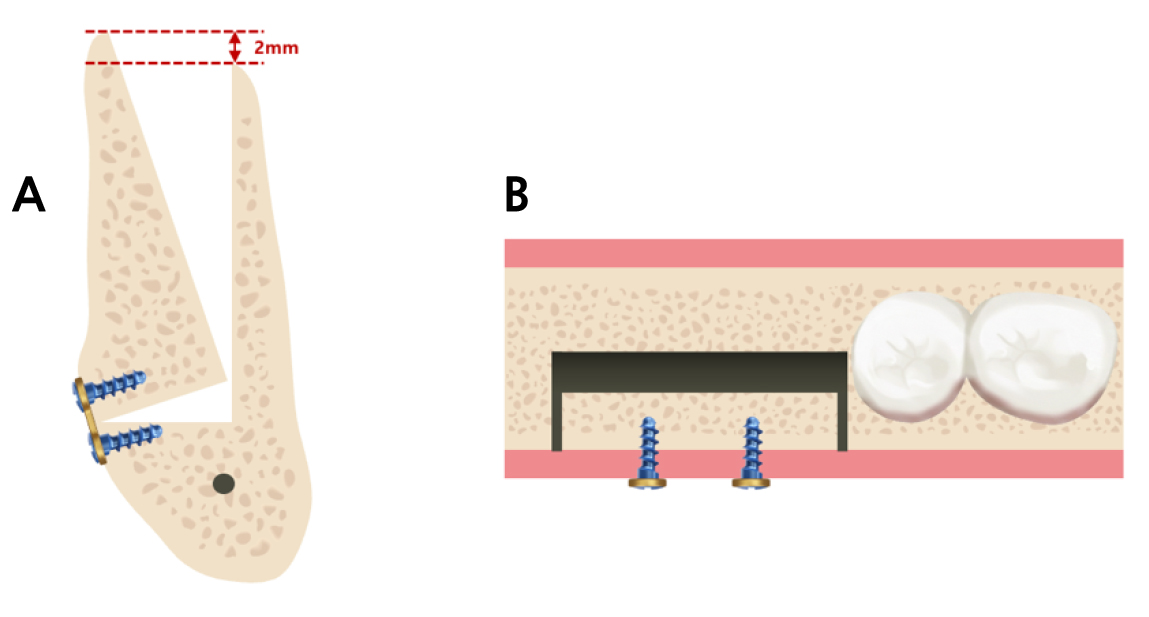
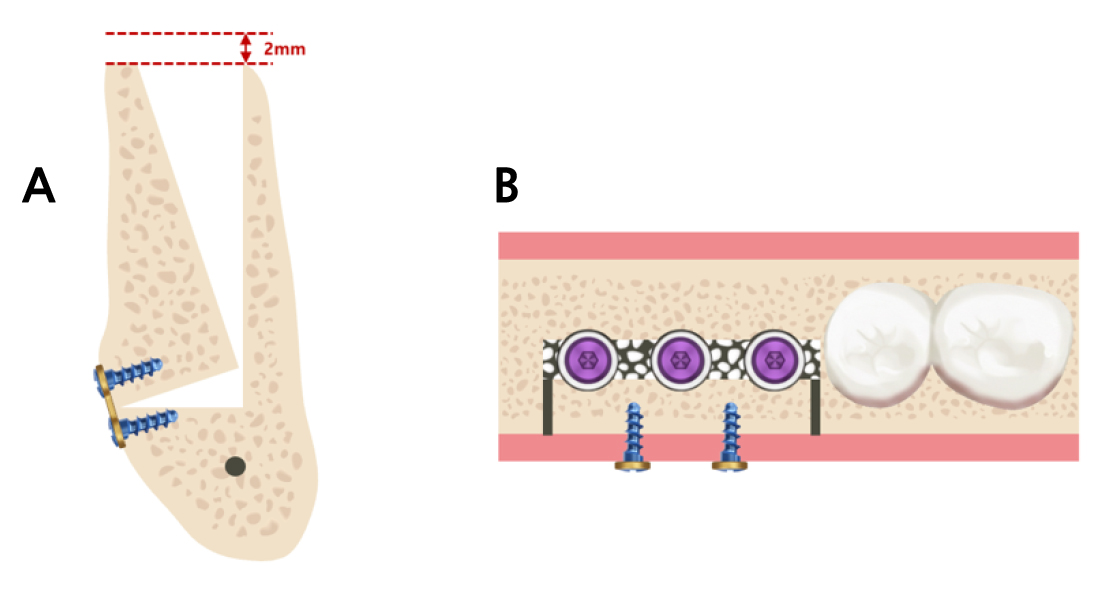
Following expansion with a chisel, the buccal cortical plate typically becomes approximately 2 mm higher than the lingual aspect of the alveolar ridge. This excess bony segment can subsequently be trimmed using a bone rongeur, and the harvested autogenous bone utilized as grafting material for GBR (Fig. 3).
Ⅱ. Case Series
1. Case 1
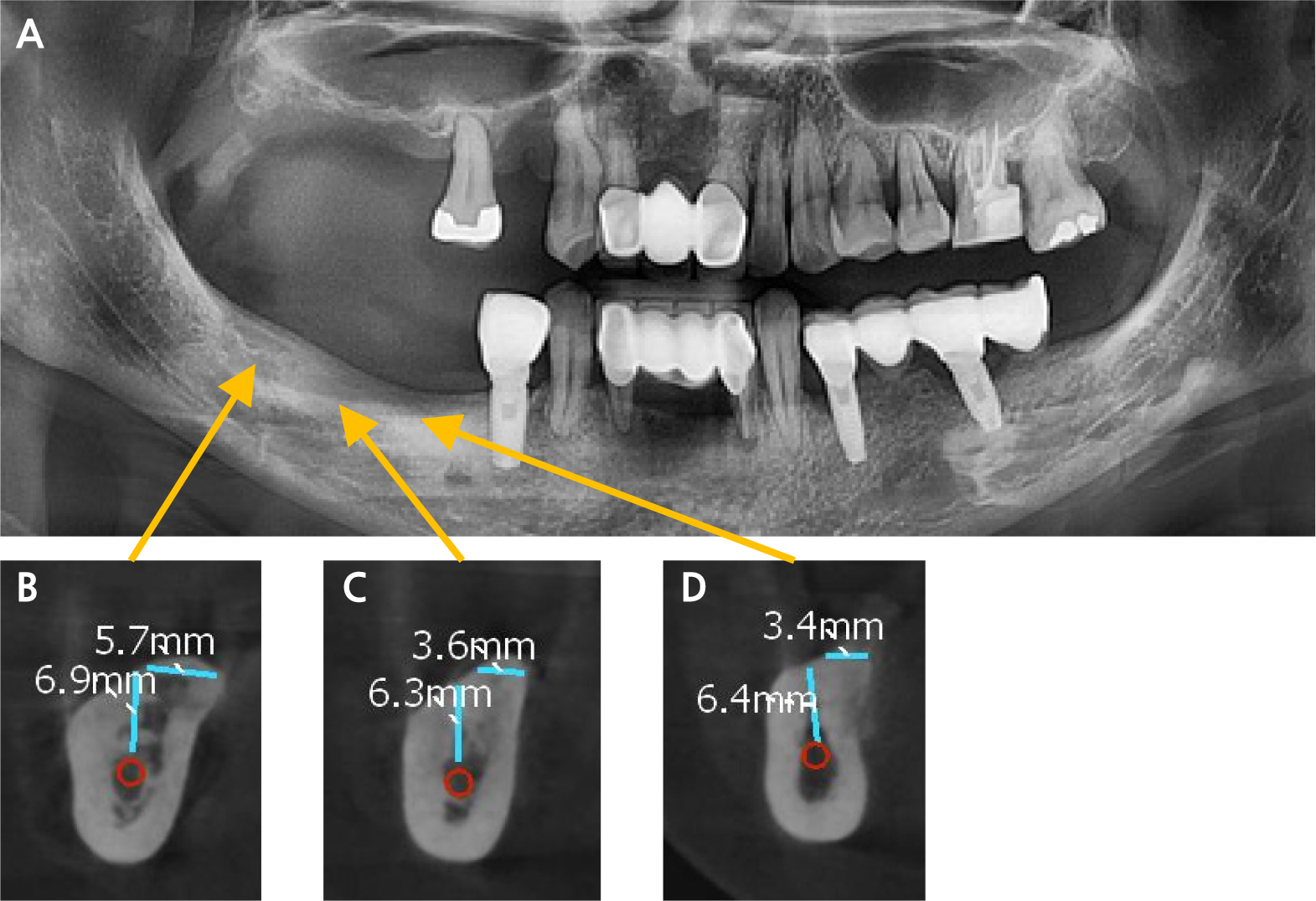
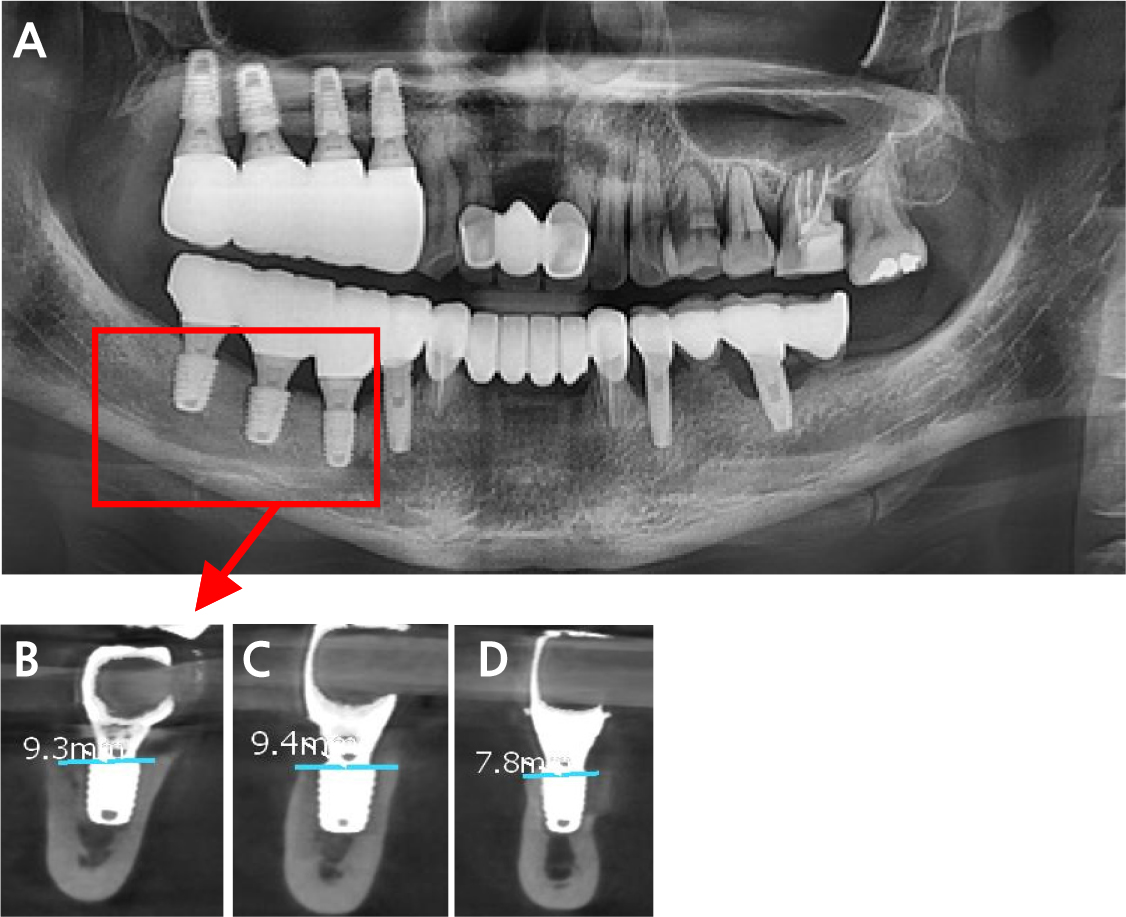
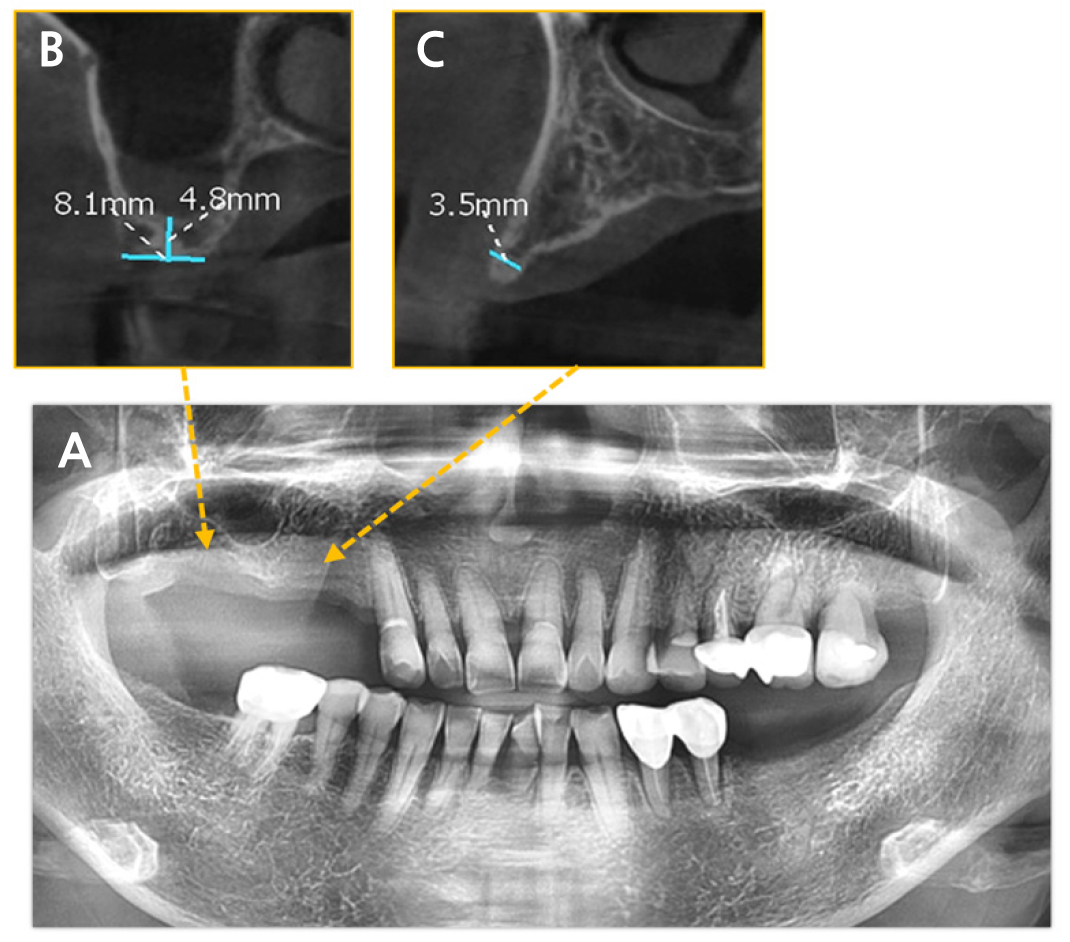
A 53-year-old patient with a noncontributory medical history presented with failed implants in the right maxillary and mandibular posterior regions. Clinical and radiographic examinations revealed alveolar bone resorption associated with the implant failure, resulting in a markedly narrow residual ridge. Cone-beam computed tomography (CBCT) and panoramic radiography (Fig. 4A) demonstrated pronounced alveolar ridge deficiency in the right mandibular posterior region, with ridge widths measuring 5.7 mm at site #47 (Fig. 4B), 3.6 mm at site #46 (Fig. 4C), and 3.4 mm at site #45 (Fig. 4D). Furthermore, inadequate vertical bone height and unfavorable ridge angulation were observed. To address these anatomical limitations, a modified alveolar ridge-splitting technique was employed to facilitate simultaneous horizontal and vertical ridge augmentation in conjunction with implant placement.
Prior to surgery, the adjacent dentition underwent thorough supragingival scaling and polishing, and the patient rinsed with 0.12% chlorhexidine digluconate (Hexamedine; Osstem, Seoul, South Korea). Local anesthesia was administered via an inferior alveolar nerve block (Scandonest 3% without epinephrine; Huons, Shiheung, South Korea) combined with buccal infiltration using articaine with epinephrine (1:100,000; Huons).
A full-thickness flap was raised using a mid-crestal incision combined with a single vertical releasing incision on the mesial aspect to expose the alveolar ridge. Modified ridge splitting was performed utilizing a piezoelectric device (Surgystar X; dmetec, Bucheon, South Korea). First, a sagittal osteotomy was created along the ridge crest (Fig. 5A), followed by vertical osteotomies on the mesial and distal aspects (Fig. 5B). An intermittent horizontal osteotomy was subsequently performed at the base of the buccal bone plate. The buccal plate was secured with miniplates (Jaeilmedical, Seoul, South Korea) and miniscrews (MCTBIO, Yongin, South Korea) and subsequently expanded buccally using a chisel (Fig. 5C). This pre-expansion stabilization permitted controlled expansion of the buccal segment while minimizing the risk of cortical fracture.
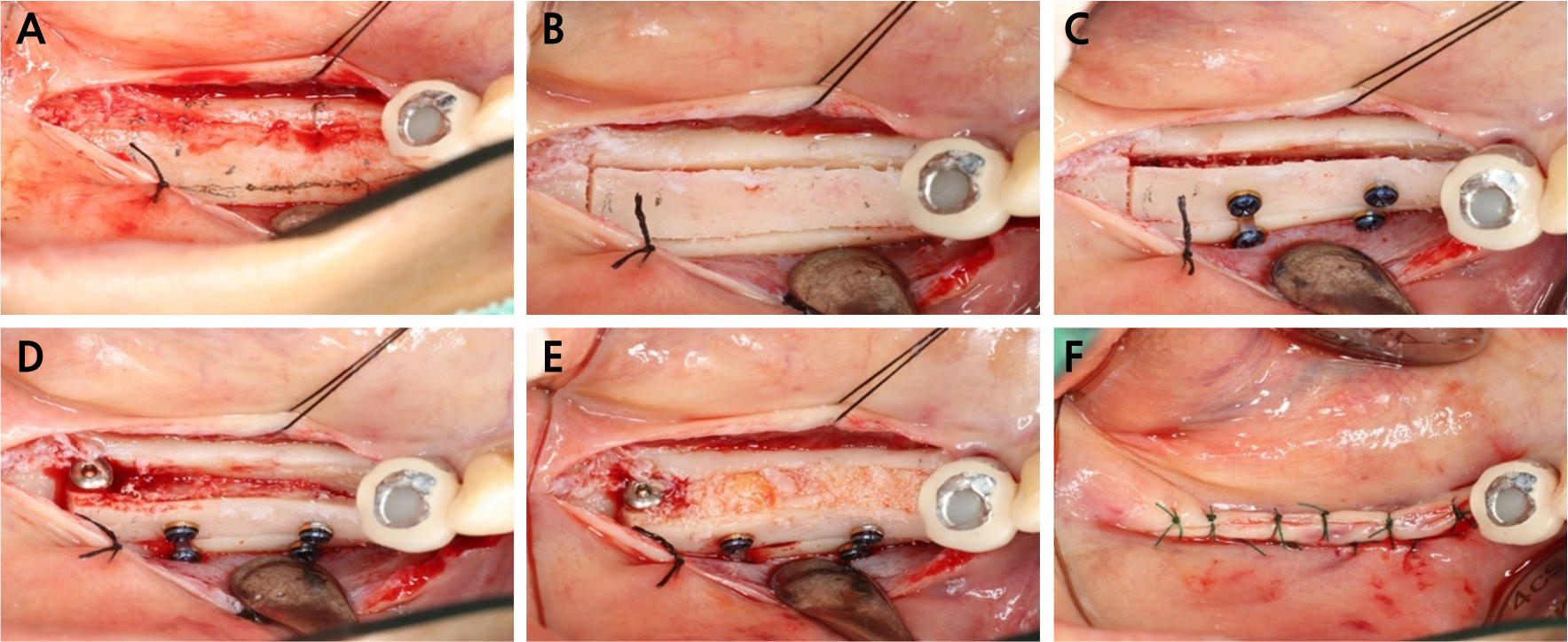
Fig. 5.
(A) Preoperative planning for osteotomies, (B) Sagittal, vertical, and horizontal osteotomies performed, (C) Two miniplates and miniscrews in place, (D) Bone spreader implant utilized to expand the buccal plate, (E) GBR performed at the expanded site, (F) Flap closure using a combination of horizontal mattress and simple interrupted sutures.
A bone spreader implant (Point Implant, Seoul, South Korea) was then placed to achieve additional ridge expansion, maintain the expanded ridge dimensions, and preserve regenerative space during the healing phase (Fig. 5D). GBR was then performed using a porcine-derived bone graft material (The Graft; Purgo, South Korea) (Fig. 5E). Primary wound closure and stable soft tissue adaptation were achieved using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0; B.Braun Surgical, S.A. Rubi, Spain) (Fig. 5F). Importantly, this expansion successfully corrected the previously unfavorable alveolar ridge angulation. An 8-week healing period was observed prior to the subsequent treatment stage.
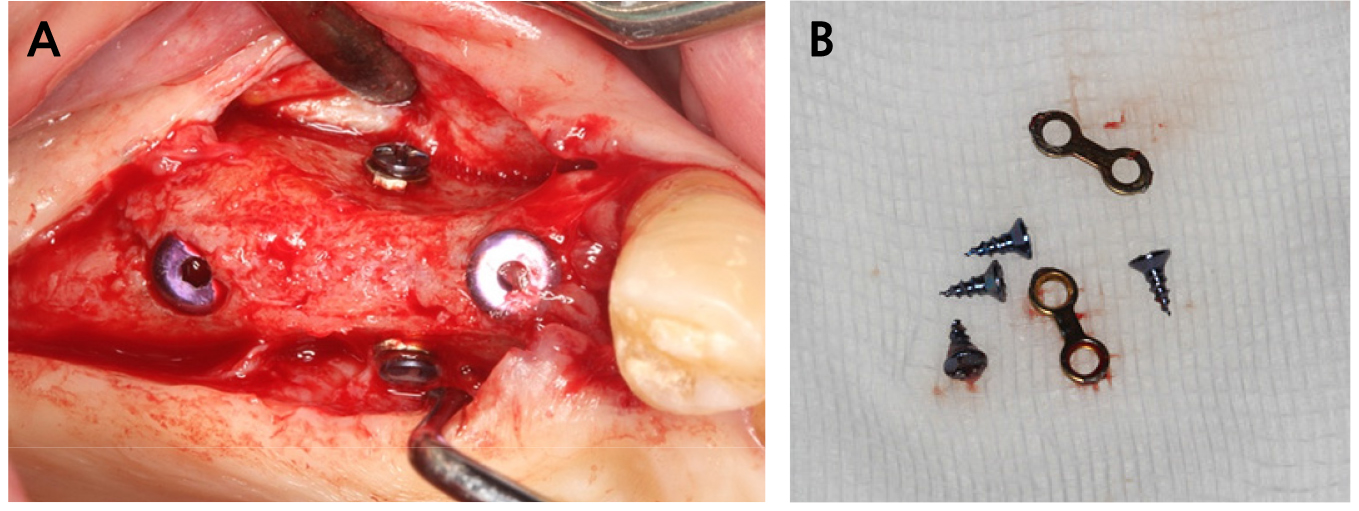
Following the 8-week healing period, implants were inserted at positions #45 (4.0 × 7.0 mm, 70 Ncm), #46 (5.0 × 7.0 mm, 70 Ncm), and #47 (5.0 × 7.0 mm, 70 Ncm) (Point Implant) (Figs. 6A to 6C). All previously placed miniplates and miniscrews were removed (Fig. 6D). Subsequently, 2-mm cover screws were placed (Fig. 6E), and concentrated growth factor (CGF) was applied prior to flap closure. The flap was sutured using horizontal mattress and simple interrupted techniques (Dafilon 3-0) (Fig. 6F). The patient received postoperative instructions along with a 3-day course of analgesics (dexibuprofen 0.4 g/tablet ) and an antacid (almagate 0.5 g/tablet) (Fig. 7).
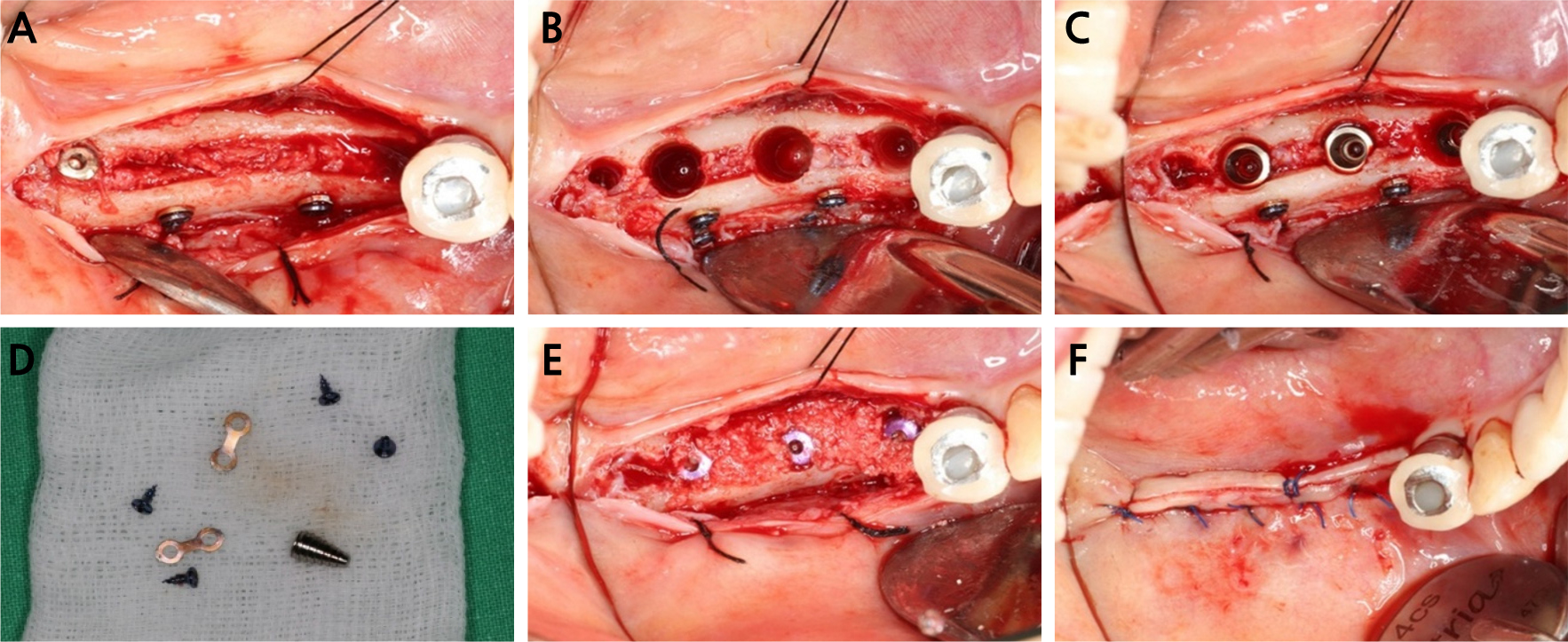
Fig. 6.
(A) Healed site observed after 8 weeks, (B) Removal of the bone spreader implant and osteotomy preparation at the planned sites, (C) Placement of the implant fixtures, (D) Removal of the miniplates and miniscrews, (E) 2-mm cover screws in place, (F) Flap closure using a combination of horizontal mattress and simple interrupted sutures.

The second-stage procedure was performed 4 months later. Local anesthesia was achieved through buccal and lingual infiltration with lidocaine containing epinephrine (Lignospan Standard, 1:100,000; Huons). The surgical site had healed without complications (Fig. 8). The cover screws were replaced with healing abutments, and simple interrupted sutures were placed (Dafilon 3-0).
Following complete soft tissue healing, the definitive prosthesis was delivered (Fig. 6B). The patient reported high satisfaction with both the aesthetic outcome and functional restoration (Fig. 9).
2. Case 2
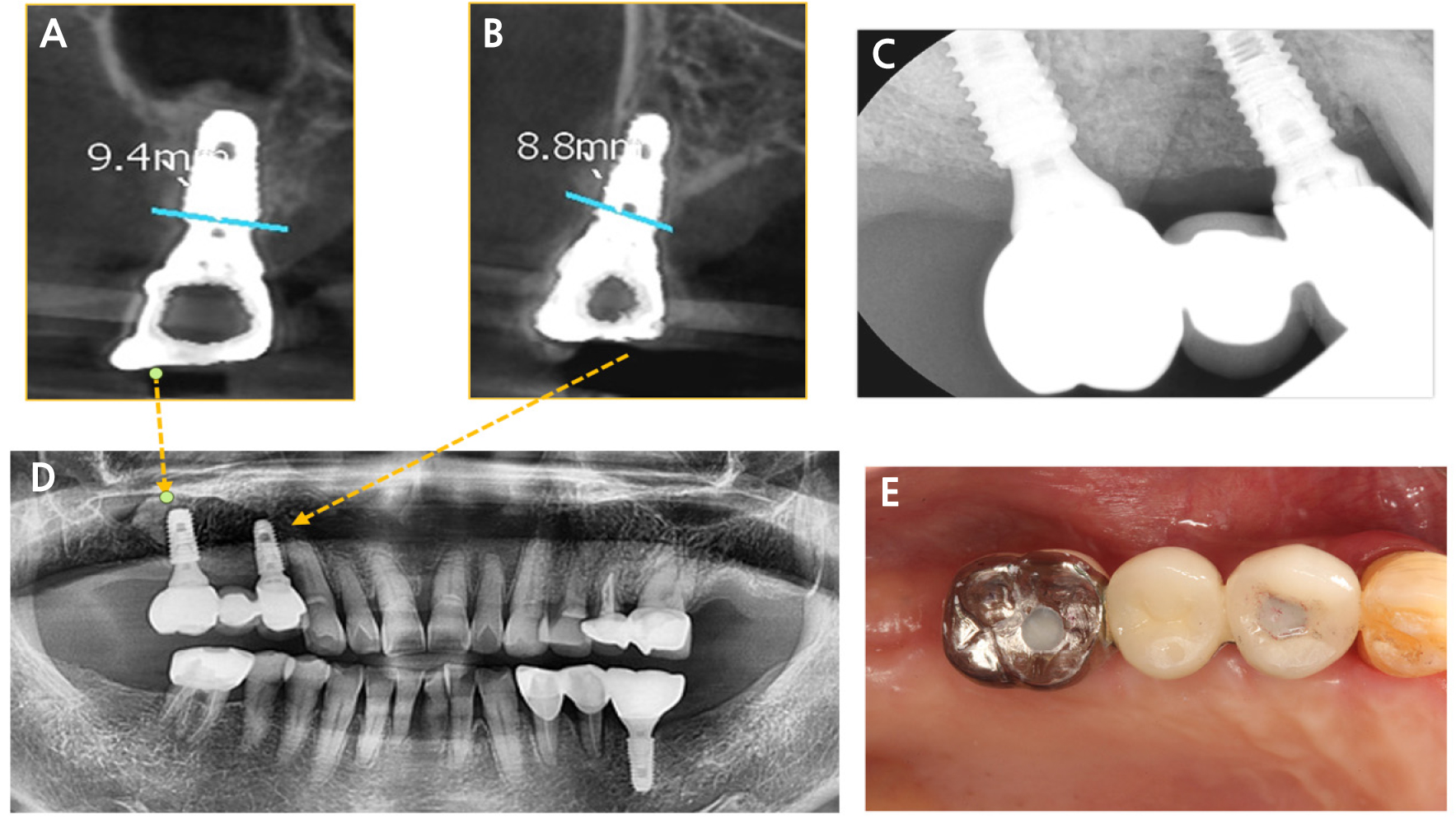
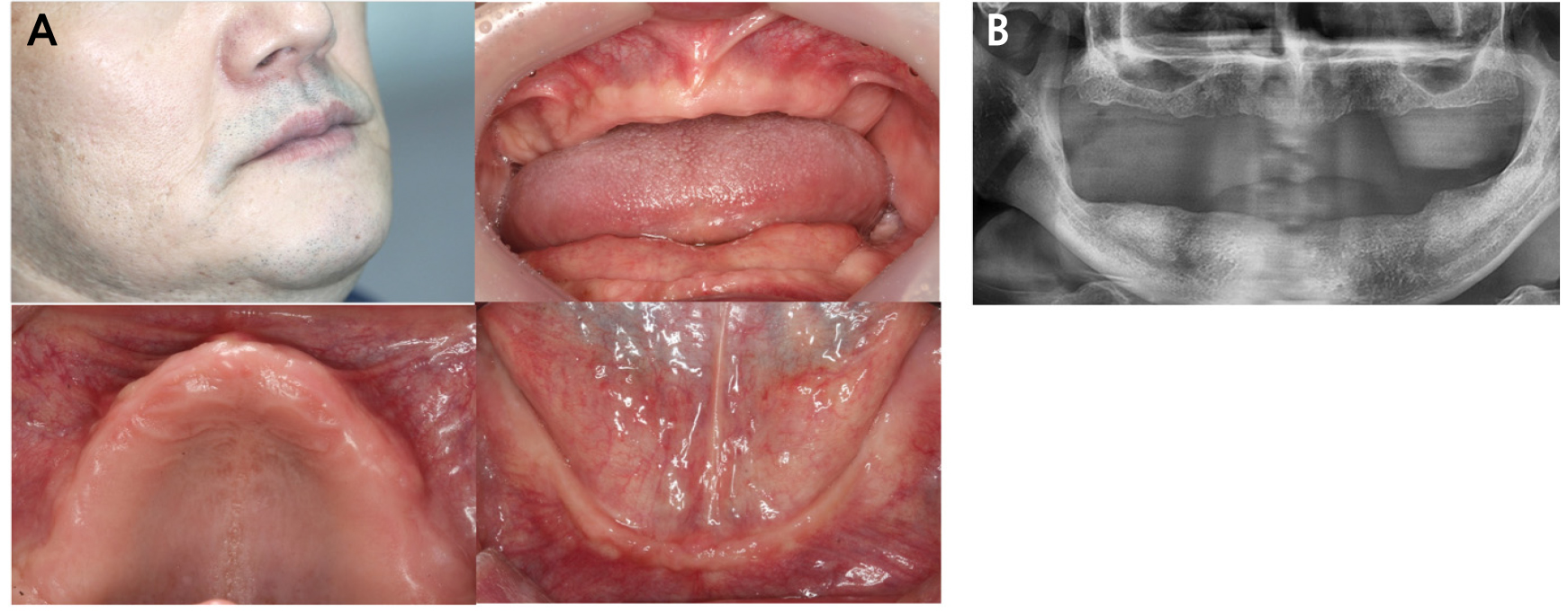
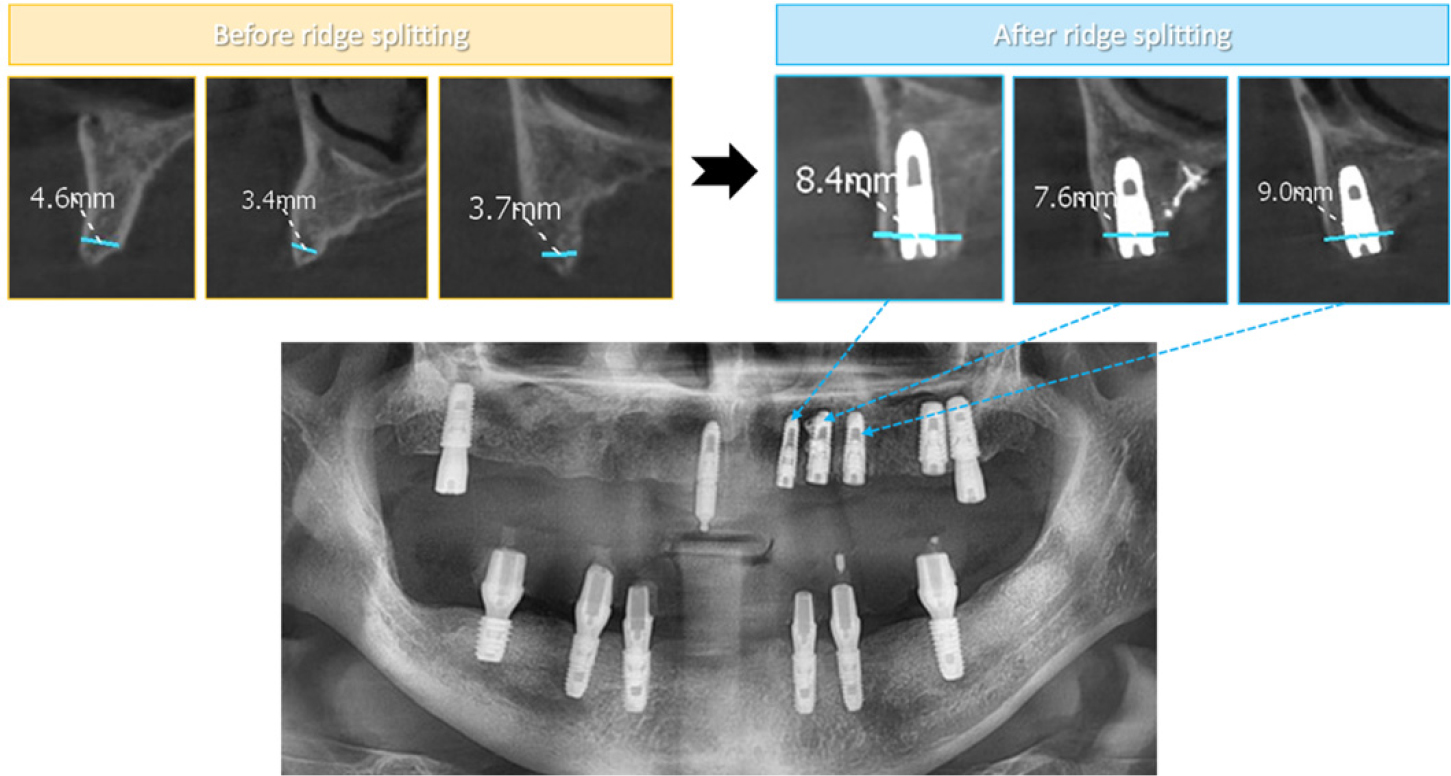
A 76-year-old patient with a noncontributory medical history presented with reduced masticatory efficiency associated with tooth loss in the right maxillary posterior region. CBCT and panoramic radiography revealed a narrow alveolar ridge with low bone density at site #14. Furthermore, insufficient vertical alveolar bone height was observed at site #16 (Fig. 10).
The proposed treatment plan included implant placement at sites #14, #16, and #36 to restore functional occlusion and improve masticatory performance. Radiographic assessment indicated that site #16 required maxillary sinus augmentation due to inadequate vertical bone height. Furthermore, the severely reduced ridge width at site #14 necessitated a modified alveolar ridge-splitting technique involving both buccal and palatal expansion. Because buccal expansion alone was considered insufficient to achieve the desired ridge dimensions, additional palatal expansion was performed to ensure adequate implant site development.
Prior to surgery, the adjacent dentition underwent thorough supragingival scaling and polishing, and the patient rinsed with 0.12% chlorhexidine digluconate (Hexamedine; Osstem). Local anesthesia was administered via buccal infiltration and a greater palatine nerve block using articaine with epinephrine (1:100,000; Huons).
A full-thickness mucoperiosteal flap was elevated via a mid-crestal incision combined with a single vertical releasing incision on the mesial aspect to expose the alveolar ridge. Clinical examination revealed severe ridge narrowing at site #14 secondary to buccal bone resorption (Fig. 11A).
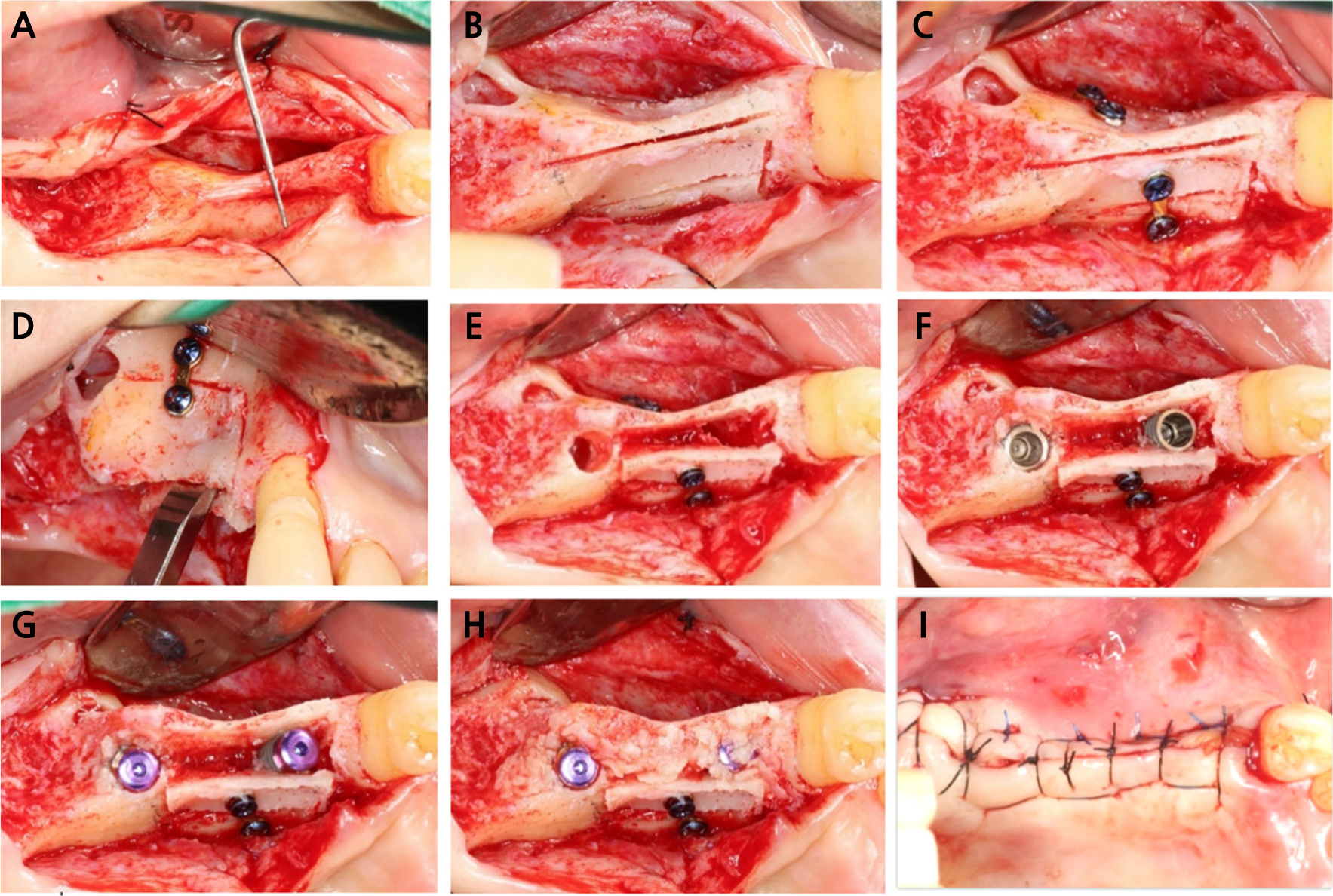
Fig. 11.
(A) Preoperative intraoral view demonstrating an extremely narrow ridge at site #14, (B) Sagittal, vertical, and horizontal osteotomies, (C) Miniplates and miniscrews stabilizing both the buccal and palatal aspects, (D) A lateral window approach performed at site #16 to facilitate maxillary sinus augmentation; a chisel is used to expand the ridge, (E) Osteotomy preparation at the planned sites, (F) Implant placement at sites #14 and #16, (G) 2-mm cover screws in place, (H) GBR performed, (I) Flap closure using a combination of horizontal mattress and simple interrupted sutures.
A lateral window approach was initially performed at site #16 to facilitate maxillary sinus augmentation. Subsequently, sagittal, vertical, and horizontal osteotomies were created utilizing a piezoelectric device (Surgystar X) (Fig. 11B). Additional vertical osteotomies were performed on the palatal aspect to enable simultaneous ridge expansion in both the buccal and palatal directions. Due to this bidirectional expansion, stabilization with miniplates and miniscrews was required on both aspects (Fig. 11C). Gradual and controlled expansion of the buccal and palatal cortical plates was achieved using a chisel (Fig. 11D). Following successful ridge expansion, sequential osteotomy preparation was performed at the planned implant sites (Fig. 11E). Implant fixtures were placed at site #14 (4.0 × 10.0 mm, 15 Ncm; Point Implant) and site #16 (5.0 × 10.0 mm, 20 Ncm; Point Implant) (Fig. 11F). Subsequently, 2-mm cover screws were placed on the implant fixtures (Fig. 11G).
GBR was then performed by applying a porcine-derived bone graft material (The Graft) to the contained defect (Fig. 11H). To achieve tension-free primary closure, a periosteal releasing incision was created to advance the buccal flap. Primary wound closure was ensured using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0) (Fig. 11I). The patient received postoperative instructions and was prescribed a 5-day course of medications, including an analgesic (loxoprofen 68.1 mg/tablet), an antibiotic (amoxicillin 500 mg; Huons, South Korea), and mosapride citrate hydrate (5.29 mg/tablet), along with a 0.12% chlorhexidine digluconate rinse (Osstem).
The second-stage procedure was performed 4 months later. Local anesthesia was achieved through buccal and palatal infiltration with lidocaine containing epinephrine (Lignospan Standard, 1:100,000; Huons). The surgical site had healed without complications (Fig. 12A). The cover screws were replaced with healing abutments (Fig. 12B), and simple interrupted sutures were placed (Dafilon 3-0).
Following complete soft tissue healing, the definitive prosthesis was delivered, successfully restoring both function and aesthetics (Fig. 13).
3. Case 3
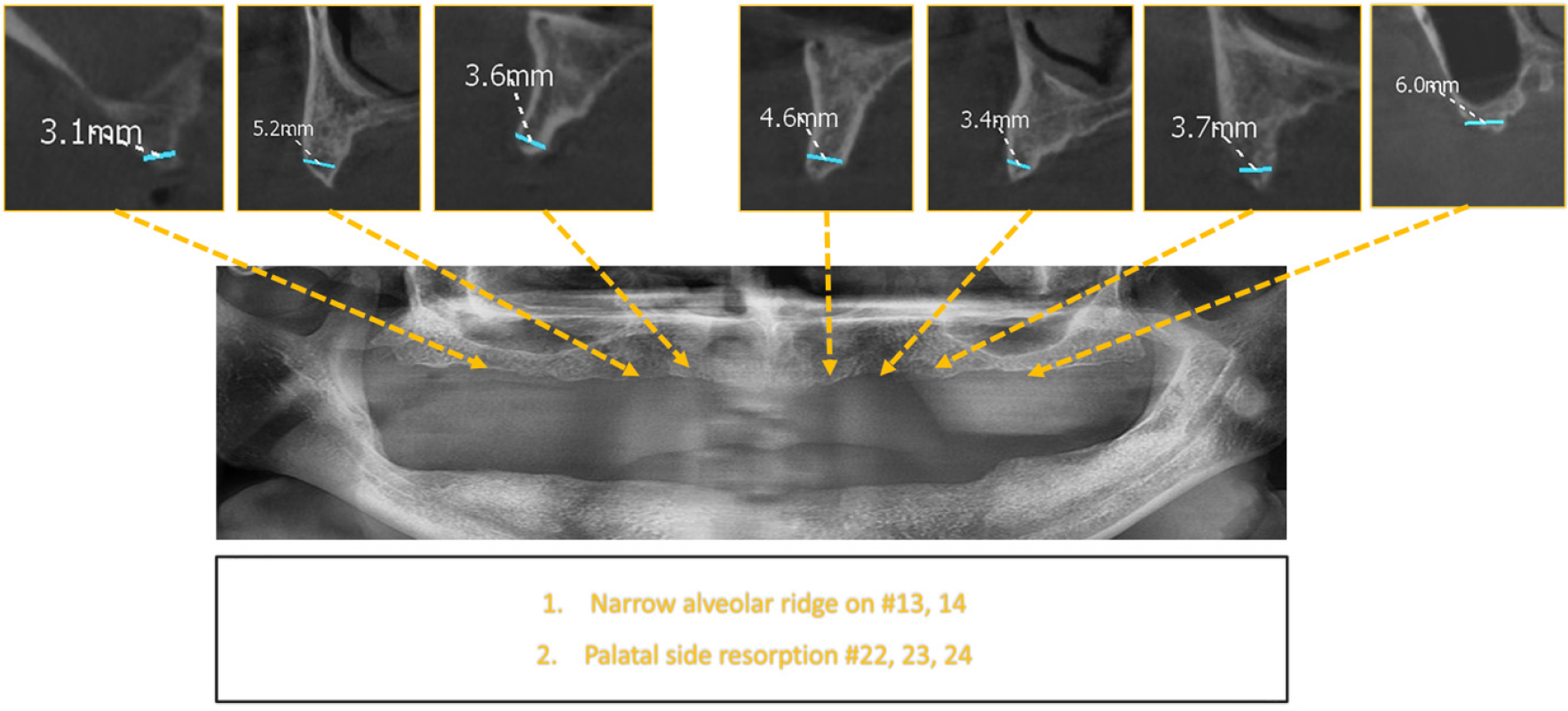
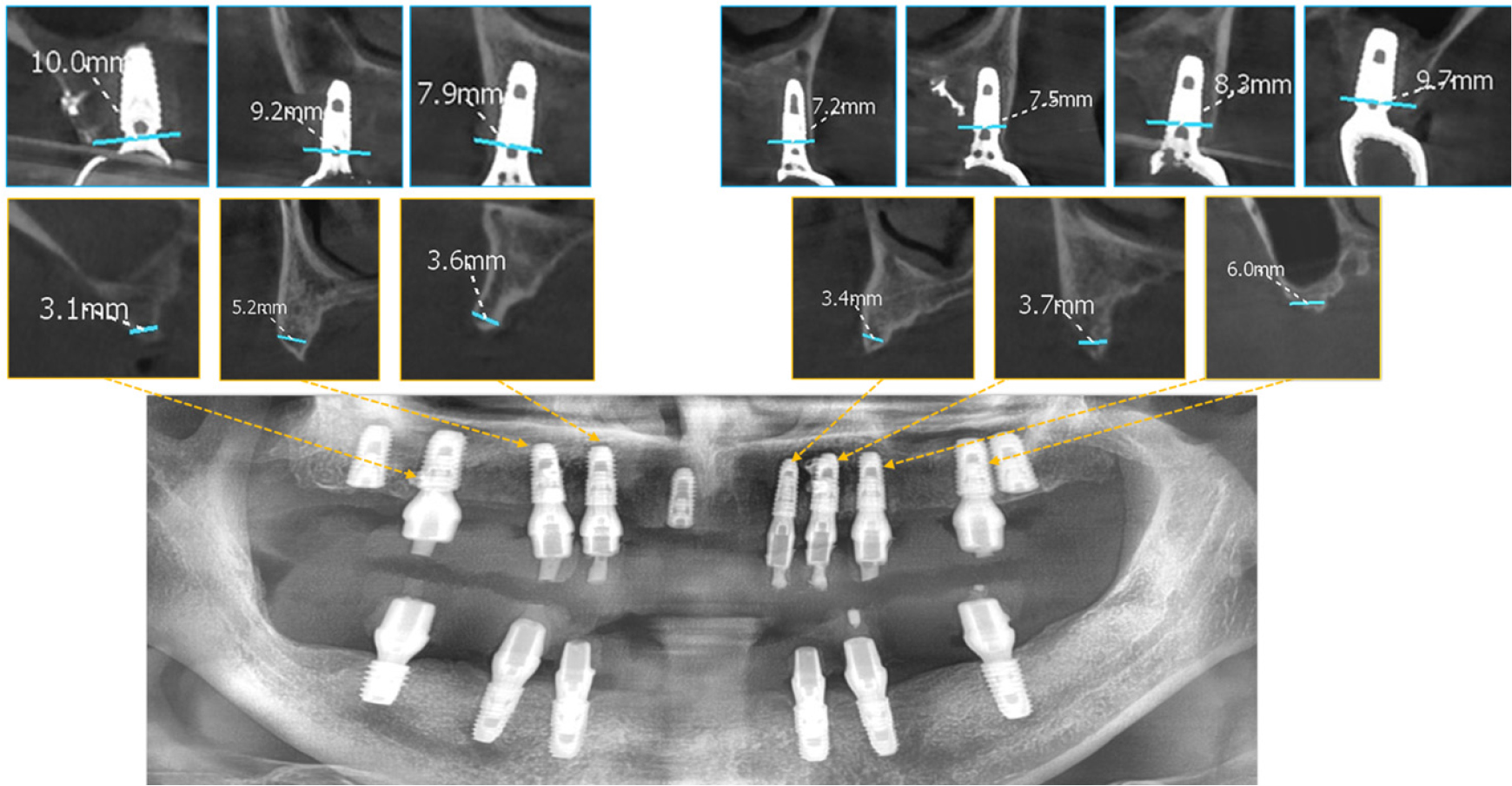
A 51-year-old male patient with well-controlled hypertension and diabetes mellitus presented for implant-supported rehabilitation following tooth loss. Clinical and CBCT evaluations revealed a narrow maxillary ridge attributed to extractions performed several years earlier (Figs. 14 and 15).
The treatment plan involved the placement of six implants in the mandible and seven implants in the maxilla, along with modified alveolar ridge splitting in the resorbed regions. In the interim, three temporary implants were inserted to support a provisional denture during the healing of the ridge-split sites.
The initial surgery involved the placement of six implants in the mandibular arch and three temporary implants in the maxilla. Although classified as temporary, these implants possessed characteristics identical to definitive implants and were used to stabilize the provisional denture throughout the healing of the ridge-split sites. Local anesthesia was achieved through buccal and palatal infiltration with articaine containing epinephrine (1:100,000; Huons). In the mandible, implants were placed at sites #33 (4.0 × 10 mm, 70 Ncm), #34 (4.0 × 10 mm, 70 Ncm), #36 (5.0 × 10 mm, 70 Ncm), #43 (4.0 × 10 mm, 70 Ncm), #44 (4.0 × 10 mm, 70 Ncm), and #46 (5.5 × 7.0 mm, 70 Ncm) (Point UV Implant); subsequently, abutments were connected to support a fixed provisional prosthesis. In the maxilla, temporary implants were positioned at sites #18 (4.5 × 10 mm, 70 Ncm), #28 (5.0 × 10 mm, 40 Ncm), and #11 (3.5 × 10 mm, 70 Ncm) (Point UV Implant), and healing abutments were placed to retain a provisional denture (Fig. 16). A lateral window sinus lift was performed at site #26, and autogenous bone collected during low-speed drilling was grafted into the site. The surgical sites were closed using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0). A healing period of approximately 4.5 months was planned prior to the subsequent stage.
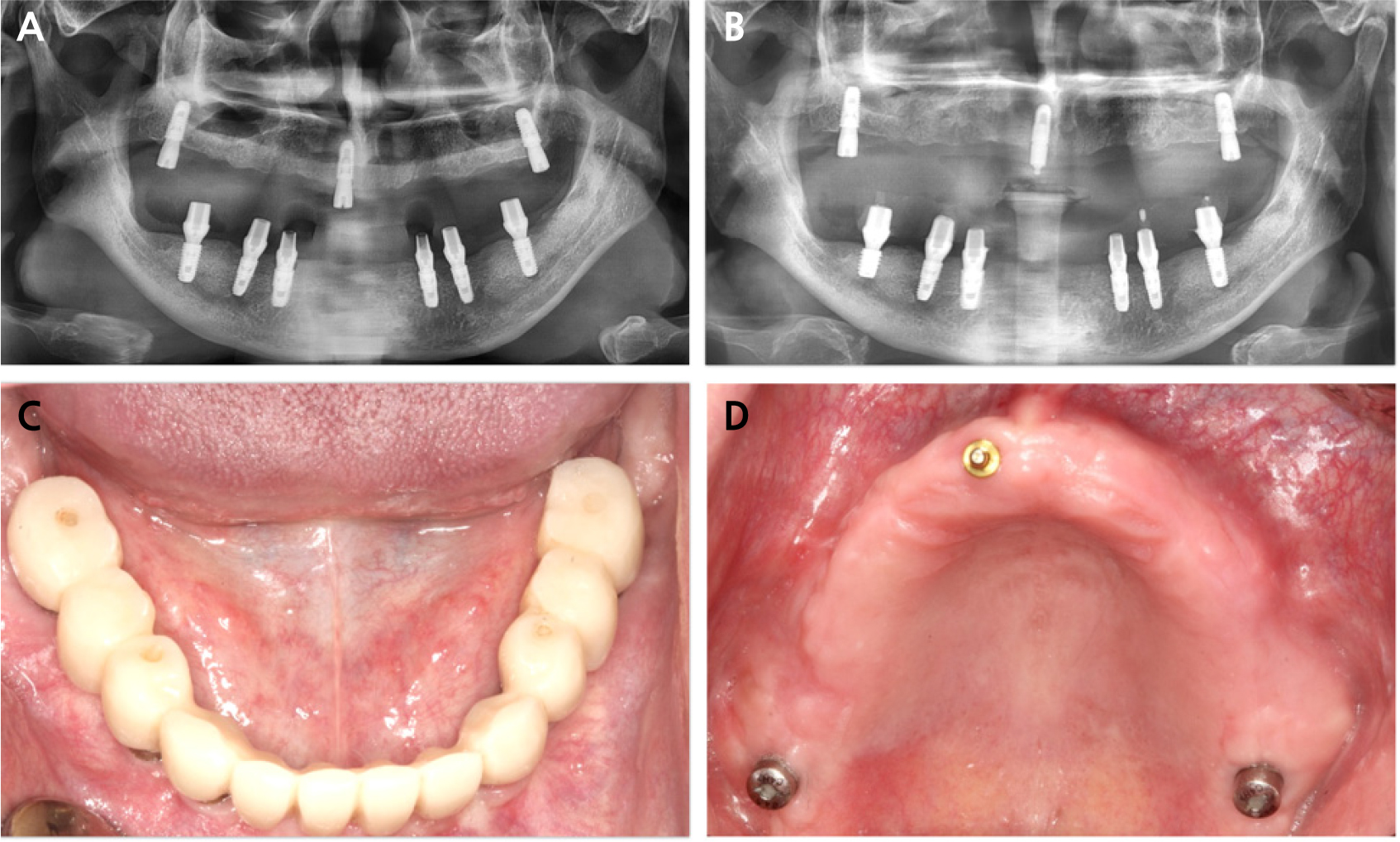
Fig. 16.
(A) Panoramic view after the placement of six implants in the mandible and three temporary implants in the maxilla, (B) Panoramic view showing a ball-type implant abutment in the maxillary anterior region, (C) Intraoral view showing temporary polymethyl methacrylate (PMMA) crowns delivered in the mandible, (D) Intraoral view demonstrating two healing abutments positioned in the posterior regions and a ball-type implant abutment placed in the anterior region.
The patient received postoperative instructions and was prescribed a 7-day course of medications, including an analgesic (loxoprofen 68.1 mg/tablet), an antibiotic (amoxicillin 500 mg; Huons), and mosapride citrate hydrate (5.29 mg/tablet), along with a 0.12% chlorhexidine digluconate rinse (Osstem).
One month later, the second-stage procedure involved a maxillary sinus lift at site #16. Local anesthesia was achieved through buccal and palatal infiltration with articaine containing epinephrine (1:100,000; Huons). A lateral window approach was utilized, and the sinus cavity was grafted with a porcine-derived bone substitute 0.25 g (The Graft). The flap was closed using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0). Postoperative care included a 5-day regimen of an analgesic (loxoprofen 68.1 mg/tablet), an antibiotic (amoxicillin 500 mg; Huons, South Korea), and mosapride citrate hydrate (5.29 mg/tablet), along with a 0.12% chlorhexidine digluconate rinse (Osstem).
Two months later, the third surgical procedure involved modified alveolar ridge splitting at sites #23 and #24. A full-thickness flap utilizing a mid-crestal incision was elevated to expose the alveolar ridge crest. Ridge splitting was performed utilizing a piezoelectric device (Surgystar X). A sagittal osteotomy was first created along the ridge crest, followed by vertical osteotomies on the mesial and distal aspects, and an intermittent horizontal osteotomy at the basal portion. The palatal bone plate was stabilized with miniplates (Jaeilmedical) and miniscrews (MCTBIO), and carefully expanded, achieving successful palatal expansion at sites #22, #23, and #24. Implants were then placed at the planned sites: #22 (3.5 × 10 mm, 30 Ncm), #23 (4.0 × 10 mm, 50 Ncm), #24 (4.0 × 10 mm, 30 Ncm), and #26 (5.0 × 10 mm, 30 Ncm) (Point UV Implant) (Fig. 17). GBR was performed using autogenous bone collected during low-speed drilling, and primary closure was achieved using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0) (Fig. 18). A healing period of 5 months was planned before the subsequent stage.
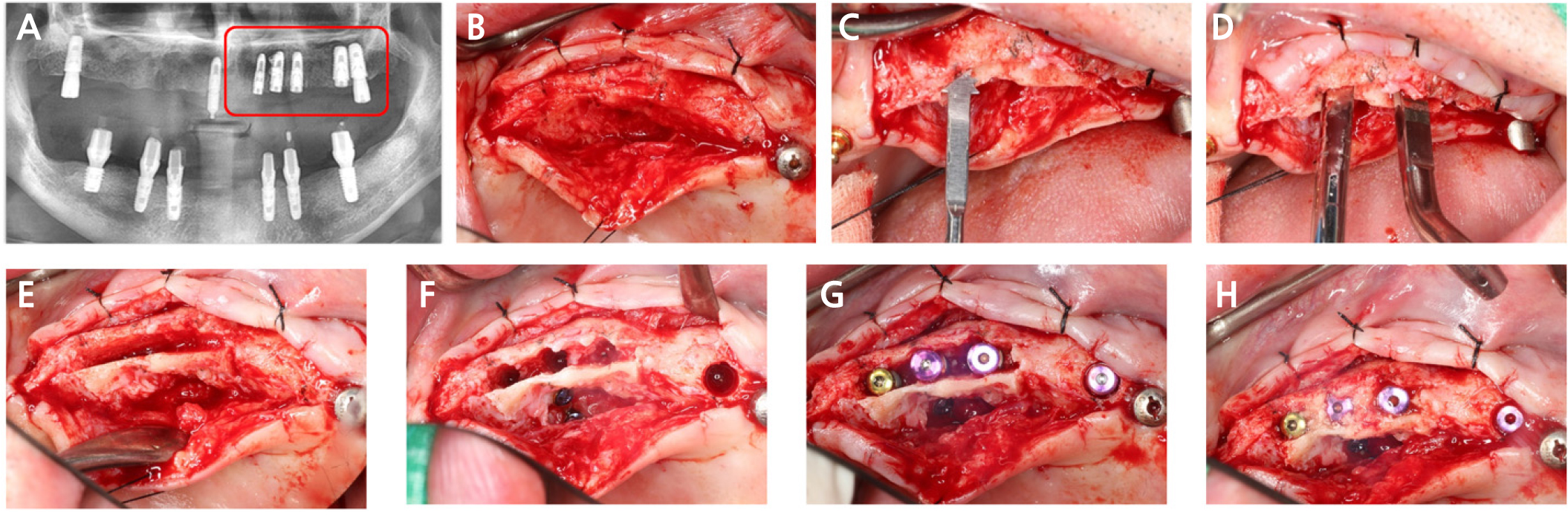
Fig. 17.
(A) Postoperative panoramic view, (B) Full-thickness flap elevation, (C) Utilization of a piezoelectric device, (D) Sagittal osteotomy, (E) Vertical and intermittent horizontal osteotomies performed, (F) Palatal bone plate stabilized with miniplates and miniscrews, (G) 2-mm cover screws in place, (H) GBR performed.
Two months later, the final surgical procedure involved modified alveolar ridge splitting at sites #13, #14, and #16. Local anesthesia was administered via buccal and palatal infiltration using articaine with epinephrine (1:100,000; Huons) (Fig. 19A). A full-thickness flap utilizing a mid-crestal incision was elevated to expose the alveolar ridge crest (Fig. 19B). Ridge splitting was performed utilizing a piezoelectric device (Surgystar X). A sagittal osteotomy was first created along the crest, followed by vertical osteotomies on the mesial and distal aspects, and an intermittent horizontal osteotomy at the basal portion (Fig. 19C).
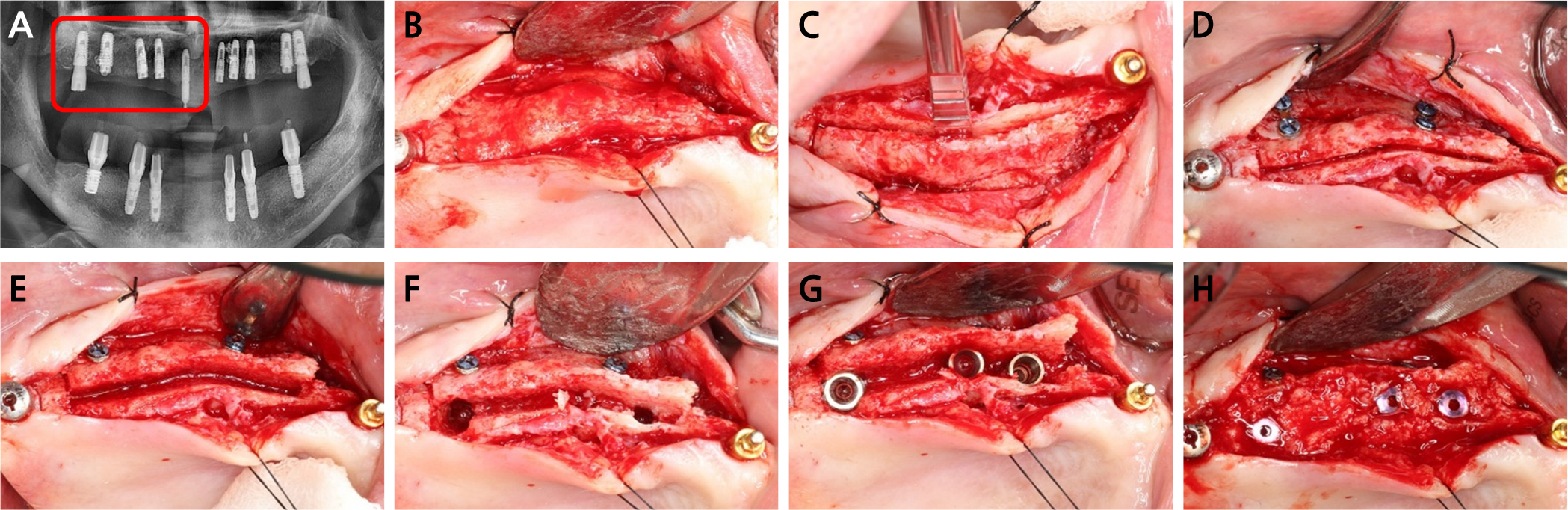
Fig. 19.
(A) Postoperative panoramic view showing implant placement at sites #13, #14, and #16, (B) Full-thickness flap elevation, (C) Sagittal, vertical, and horizontal osteotomies performed, (D) Buccal bone plate stabilized with two miniplates and miniscrews, (E) Buccal bone plate expansion, (F) Osteotomy preparation at the planned sites, (G) Implant placement at sites #13, #14, and #16, (H) 2-mm cover screws in place and GBR performed.
The buccal bone plate was stabilized using miniplates (Jaeilmedical) and miniscrews (MCTBIO) and subsequently expanded (Fig. 19D). Implants were placed at the planned sites: #13 (4.0 × 10 mm, 40 Ncm), #14 (4.0 × 10 mm, 40 Ncm), and #16 (5.0 × 10 mm, 40 Ncm) (Point UV Implant) (Figs. 19E to 19G ).
GBR was performed using autogenous bone collected during low-speed drilling combined with a porcine-derived bone substitute (The Graft) (Fig. 19H). Primary closure was achieved using a combination of horizontal mattress and simple interrupted sutures (Dafilon 3-0). A healing period of 5 months was scheduled prior to the next stage.
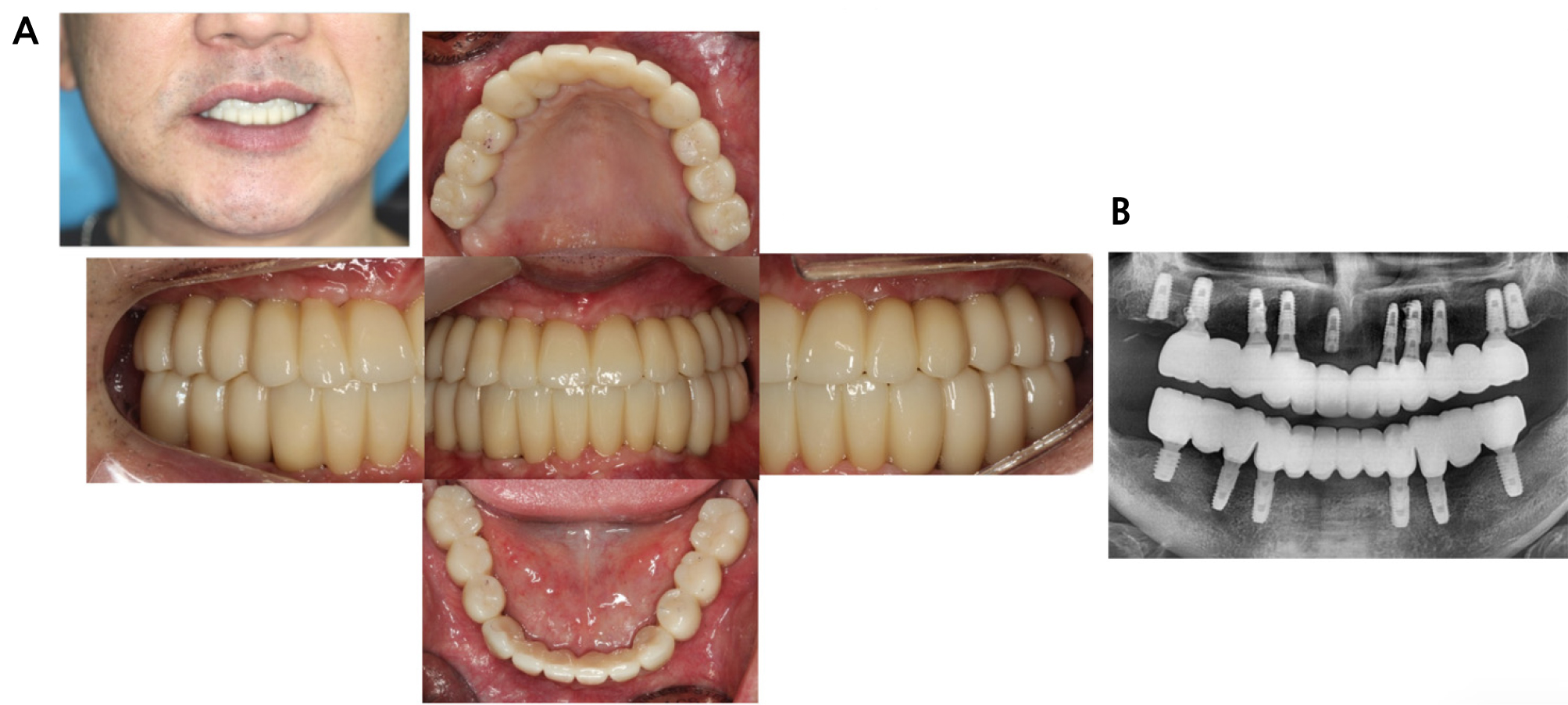
Following the final maxillary surgical procedure, a 5-month healing period was observed to ensure complete osseous integration. After thorough patient consultation, the three temporary maxillary implants previously used to support the provisional denture were submerged. All miniplates and miniscrews were removed following the completion of treatment (Fig. 20). Definitive fixed implant-supported prostheses were subsequently delivered in both the maxillary and mandibular arches. The patient reported a high level of satisfaction, noting improved comfort without removable dentures, enhanced masticatory function, and greater confidence in speech during social interactions (Fig. 21).
Ⅲ. Results
All three case patients were scheduled for follow-up evaluations at 1, 3, 6, 12, 18, and 24 months after definitive prosthesis placement to facilitate the early detection and management of any postoperative complications. Throughout the observation period, clinical examinations revealed stable peri-implant soft tissue conditions without signs of inflammation or implant mobility. Radiographic assessments further demonstrated maintained marginal bone levels, sustained osseointegration, and preservation of alveolar bone width around the implants.
Ⅳ. Discussion
The alveolar ridge-splitting technique can be selected for horizontal bone augmentation in cases presenting with insufficient ridge width but adequate vertical bone height.
In 1992, Simion et al.3 described this technique as an effective and predictable method for horizontal bone augmentation. Histological analysis revealed new bone development within the gap formed by the mobilized cortical plates. Additionally, this method facilitates simultaneous ridge augmentation and implant placement.
A primary advantage of alveolar ridge splitting is the generation of new bone within the contained defect formed by the mobilized cortical plates. An animal study by Scipioni et al.4 demonstrated that primary bone contact at the time of implant placement is not an absolute prerequisite for osseointegration. Successful integration can occur despite an initial gap between the implant surface and the surrounding bone, provided that adequate implant stability is maintained and the biological environment is conducive to healing. Under such conditions, osseointegration is achieved through de novo bone formation, leading to progressive bone deposition and subsequent direct bone-to-implant contact.
Scipioni et al.5 documented that implants placed using this technique demonstrated a 98.8% success rate over a 5-year period. Nevertheless, achieving such outcomes depends on thorough patient selection and precise surgical technique. Their findings also indicated that, following alveolar ridge splitting, the buccal bone plate should maintain a minimum thickness of 1.5 mm.
Favorable clinical results are largely influenced by careful patient selection, atraumatic and precise surgical handling, and the application of gradual, well-regulated expansion forces. Incorporating piezoelectric devices6 improves surgical safety and accuracy while reducing the risk of cortical plate damage. In the present case series, adequate bone density combined with careful surgical execution facilitated reliable ridge expansion and satisfactory primary implant stability.
In 2000, Chee7 concluded that combining alveolar ridge splitting with GBR and immediate tapered implant placement appears to be an effective strategy for expanding narrow atrophic maxillary ridges, enabling secure implant placement and reducing overall treatment time.
In the event of a buccal plate fracture during gradual expansion, bone augmentation alone may be performed, while implant insertion is delayed until the bone plate has been reinforced with a metal fixation plate.8 In all three cases included in this case series, metal fixation miniplates were applied even when the buccal plate remained intact. This approach permitted controlled expansion of the buccal plate while mitigating the risk of fracture, as the miniplates provided stabilization prior to expansion. If the alveolar ridge width is insufficient and buccal plate expansion alone is deemed inadequate, a combined buccal and palatal expansion approach with adjunctive osteotomies may be performed and stabilized using miniplates and miniscrews. This technique facilitates bidirectional ridge expansion, enabling augmentation of both the buccal and palatal aspects.
The incorporation of miniplates and miniscrews during modified alveolar ridge splitting improves stabilization of the buccal cortical segment, thereby reducing the risk of uncontrolled fractures during expansion. Nevertheless, several disadvantages and clinical limitations must be considered. The use of osteotomies in ridge-splitting procedures may be associated with increased postoperative swelling and pain. Moreover, the additional flap reflection required for hardware fixation can increase operative complexity and compromise periosteal vascularity, potentially contributing to delayed healing, cortical resorption, or wound dehiscence. Furthermore, the use of fixation devices increases treatment costs and occasionally requires a secondary surgical intervention for removal.
Appropriate patient selection remains essential for predictable outcomes. Ridge splitting with fixation is generally less favorable in severely atrophic ridges with minimal cancellous bone, as limited bone elasticity reduces expansion capacity and fixation stability. Patients with impaired healing potential, such as those with uncontrolled diabetes, individuals with a history of irradiation, or those receiving antiresorptive medication, may demonstrate a higher incidence of postoperative complications. Furthermore, thin soft-tissue biotypes and severe vertical bone deficiencies may negatively influence surgical and restorative outcomes. Consequently, this approach appears most suitable in cases presenting with moderate horizontal ridge deficiency, adequate bone quality, and favorable systemic and soft tissue conditions.
Ⅴ. Conclusion
Within the limitations of this case series, alveolar ridge splitting demonstrated predictable horizontal ridge augmentation with concurrent implant placement in narrow mandibular and maxillary ridges. In selected cases, this approach provides a shortened treatment duration and favorable outcomes, representing a clinically robust treatment option.
