

Ⅰ. Introduction
Ⅱ. Materials and Methods
1. Patients and data collection
2. Criteria for evaluating the success rates of implant overdentures
3. Statistical Analysis
Ⅲ. Results
1. Survival rates
2. Success rates
Ⅳ. Discussion
Ⅴ. Conclusion
Ⅰ. Introduction
The treatment of edentulism is critical for individuals in terms of functional and psychological aspects, as it improves their nutritional status and overall health, and has a significant impact on their quality of life and self-esteem. Edentulism can be treated using removable prostheses, fixed prostheses, or implant overdentures.1 A thorough intra- and extraoral examination is necessary to determine the prosthetic method to use.
Fixed prostheses have the best masticatory power and are convenient to use; however,they are expensive and require more maintenance. In contrast, implant overdentures are more cost-effective and offer advantages in terms of retention, support, stability, masticatory power, and psychological stability. They also maintain the alveolar bone and enhance proprioception compared to removable dentures. However, implant overdentures increase the treatment cost and duration, and require more maintenance than conventional dentures. Most patients prefer implant-supported fixed prostheses to removable prostheses; however, sufficient bone quality and quantity are necessary.2, 3
A study found that implant overdenture treatment had 4–10 times more complications than that using fixed prostheses. The number and placement of implants are critical because augmentation and technical procedures for dentures can increase the patient’s financial and physical burden. Minimally invasive treatments are necessary, particularly for elderly patients. For implant overdentures, at least four implants are required in the maxilla and two in the mandible.4, 5, 6, 6, 8, 9 Many patients prefer implant placement in the posterior region rather than the anterior region; however, bone resorption can limit this.
This study examines whether the number and placement of implants affect the survival and success rate of implants used for implant overdentures. Additionally, the relationship between patient information such as sex and age and the survival and success rates of implants is also analyzed.
Ⅱ. Materials and Methods
1. Patients and data collection
This study included patients who underwent implant surgery for overdenture treatment from 2005 to 2020 by a single surgeon at the Oral and Maxillofacial Surgery Department at Seoul Asan Medical Center. A total of 47 patients with 146 implants were included in the study. Data were collected from patient files and divided into the following categories: 1) patient factors: age and sex; 2) implant factors: implant placement location (maxilla/mandible, anterior/posterior) and the number of implants. This study was approved by institutional review board (IRB) of Asan Medical Center (No. S2018-0257-0001).
2. Criteria for evaluating the success rates of implant overdentures
1) Survival rates of implants: All cases except the following were classified as implant survival.
- Loss of implants
- Implants that should be explanted due to pain, severe mobility, and exudation
2) Success rates of implants:10 Cases that met all of the following criteria were classified as implant successess.
- Implant survival
- No pain or tenderness upon function
- Absence of mobility of the implant
- Approximately < 2 mm radiographic bone loss from the initial surgery
- No history of uncontrolled exudate
3) Exclusion criteria
- Fracture of denture framework
- Fracture of implant prosthesis
- Inability to adapt to overdentures due to pain or discomfort
- Uncontrolled systemic diseases
3. Statistical Analysis
Kaplan-Meier analysis was used to estimate the survival and success of implant overdentures. Pearson’s chi-squared test was used to determine the relationship between categorical data and the implant’s survival and success rates.
Ⅲ. Rsults
A total of 146 implants were placed in 47 patients for implant overdentures (Fig. 1). The average follow-up period was 5.03 ± 3.89 years. The mean age of the patients was 69.2 ± 9.9 years (median age: 71 years). Among the patients, 19 were men and 28 were women. Of the 146 implants, 103 (70.5%) were placed in the mandibular anterior region, eight (5.5%) in the mandibular posterior region, 26 (17.8%) in the maxillary anterior region, and nine (6.2%) in the maxillary posterior region. Among the 51 implant-supported overdentures, those with two implants were the most common, with 24 (47%) dentures, followed by those with four implants in 18 (35%). There were six dentures with three implants (12%), two dentures with one implant (4%), and one denture with six implants (2%). The total survival and success rates of the implants were 98.6% and 95.9%, respectively.
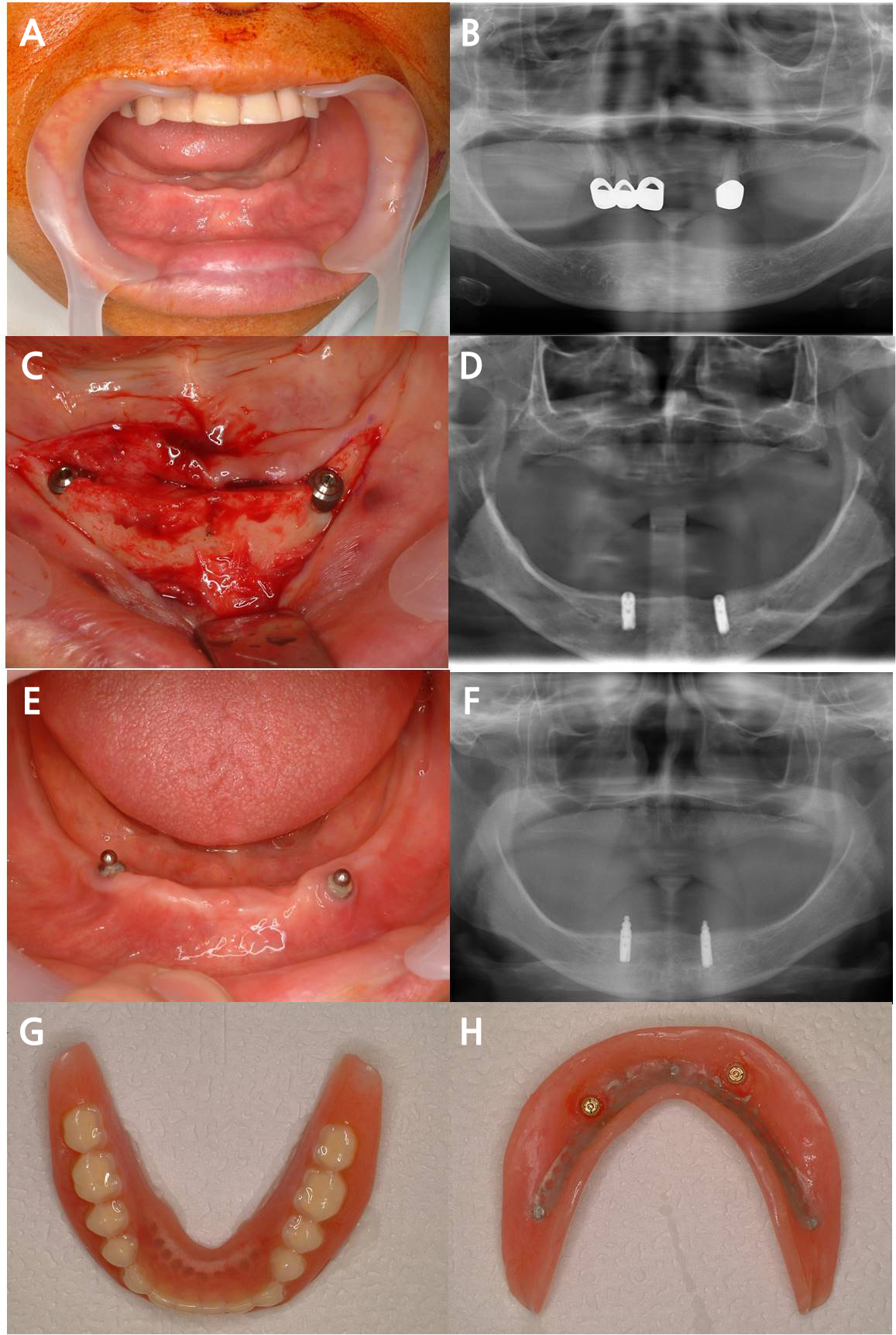
Fig. 1.
Overdenture case 1. A case of overdenture using two implants in the mandibular anterior region, which is most frequently used in this study. (A, B) Clinical photograph and panoramic radiograph before implant placement, (C) Photograph during implant surgery, (D) Panoramic radiographs after implant placement, (E, F) Ball attachment connection, (G, H) Definitive complete denture with attachment housing and retentive element.
1. Survival rates
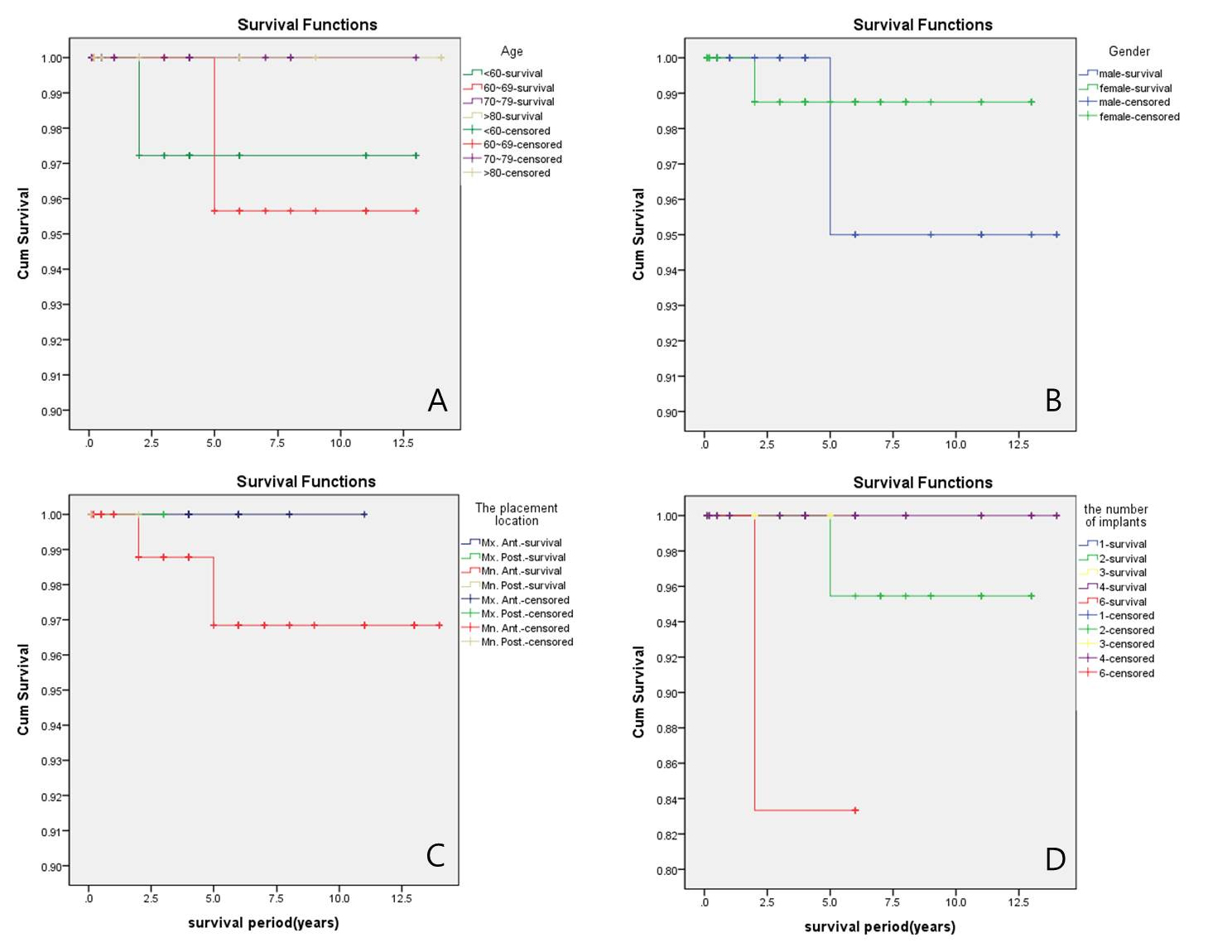
The overall survival rate was 98.6% (Fig. 2). There were two cases of implant failure, one in the mandibular molar area of a patient who underwent a fibular free flap (Figs. 3 and 4) and the other in the mandibular anterior area (Fig. 5). The Pearson chi-squared test revealed a p-value of 0.019 between the number and survival rate of implants. When six implants were placed, only 83.3% (5/6) of the implants survived. In contrast, when two implants were placed, the survival rate was 97.9% (47/48), while it was 100% when one, three, or four implants were placed. However, since no clear tendency was observed for the survival rate of implants to decrease as the number of implants increased, and there was only one case with six implants, it was unreasonable to assume a correlation between the number and survival rate of implants based solely on the p-value of 0.019 from the chi-squared test. All other categorical data and implant survival rates were not correlated, as the p-value was greater than 0.05 (Table1 and Fig. 6).
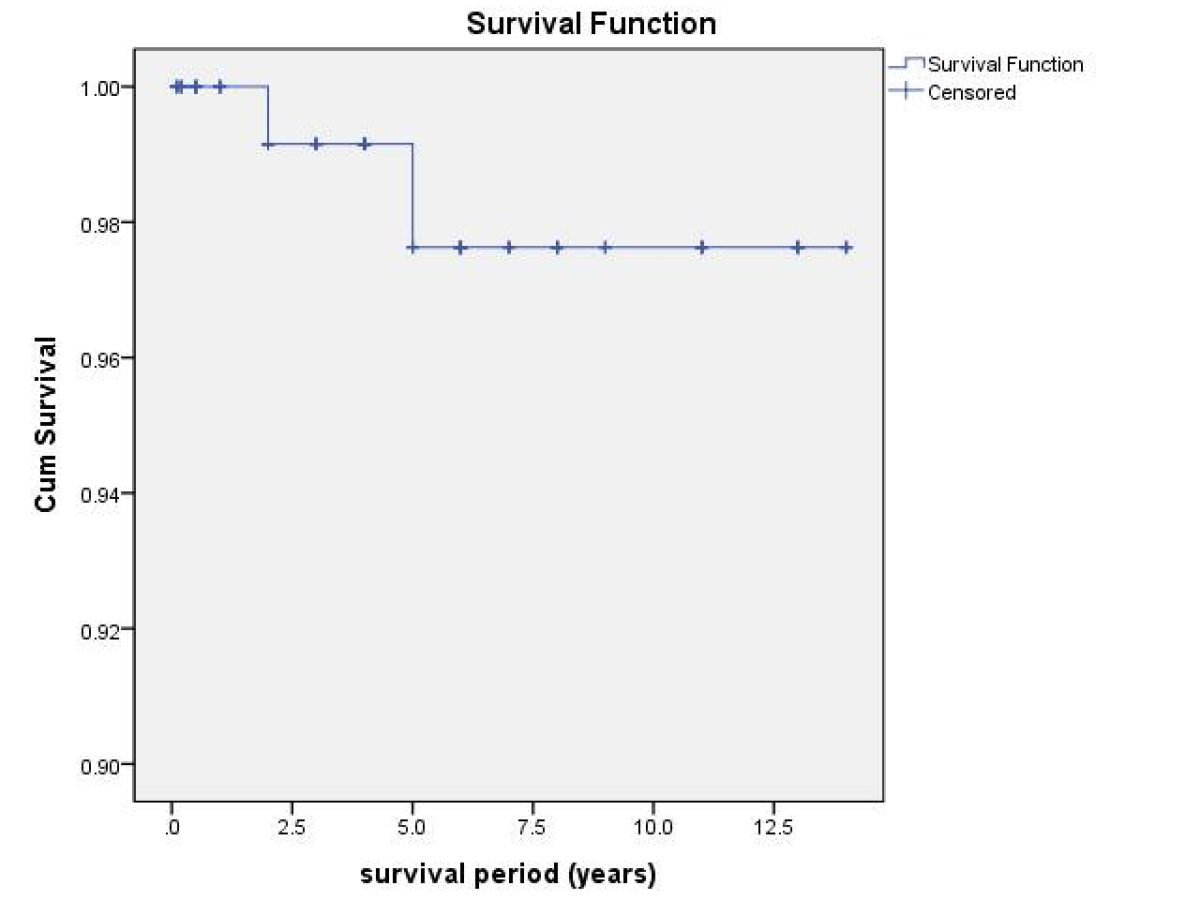
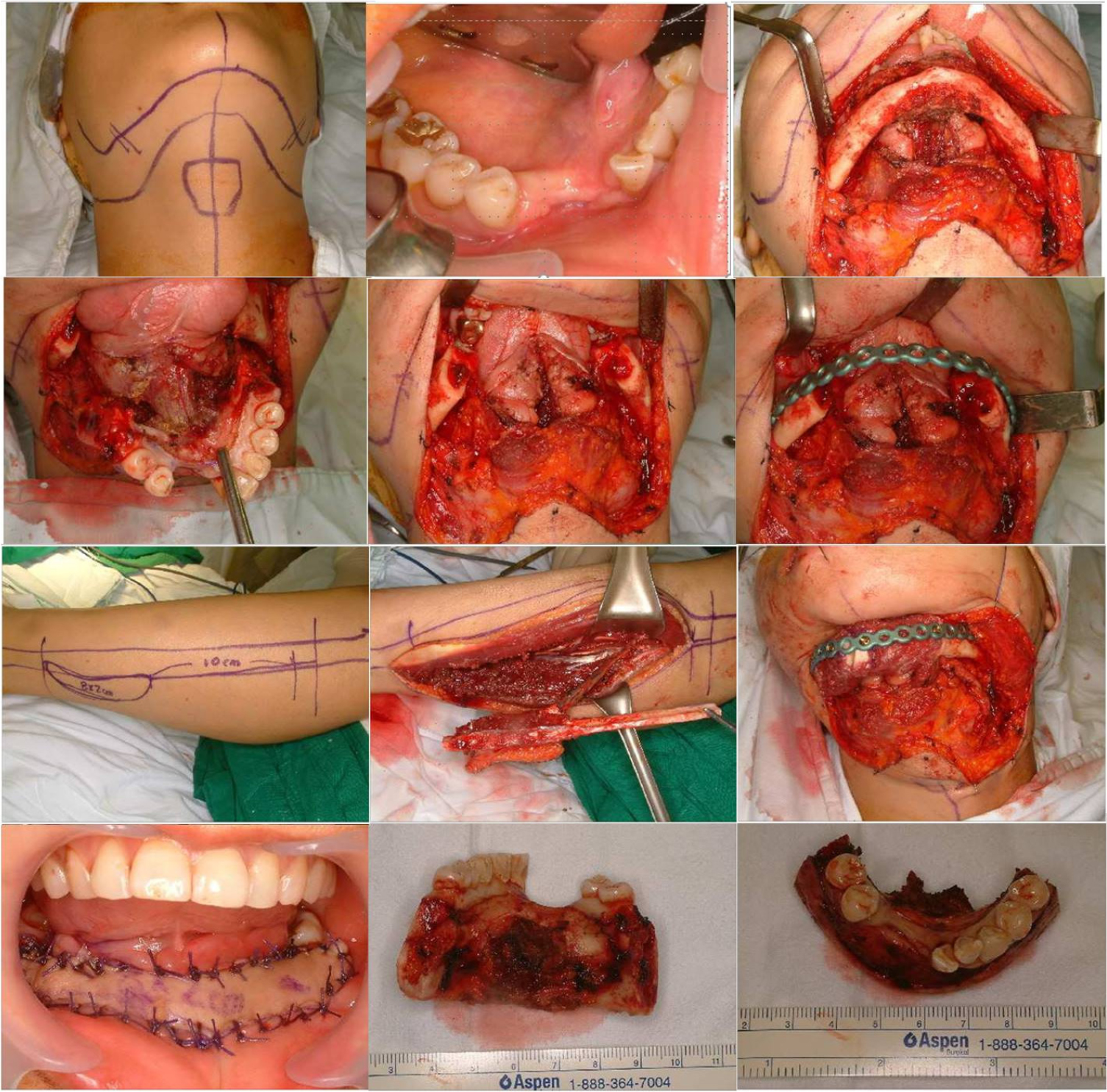
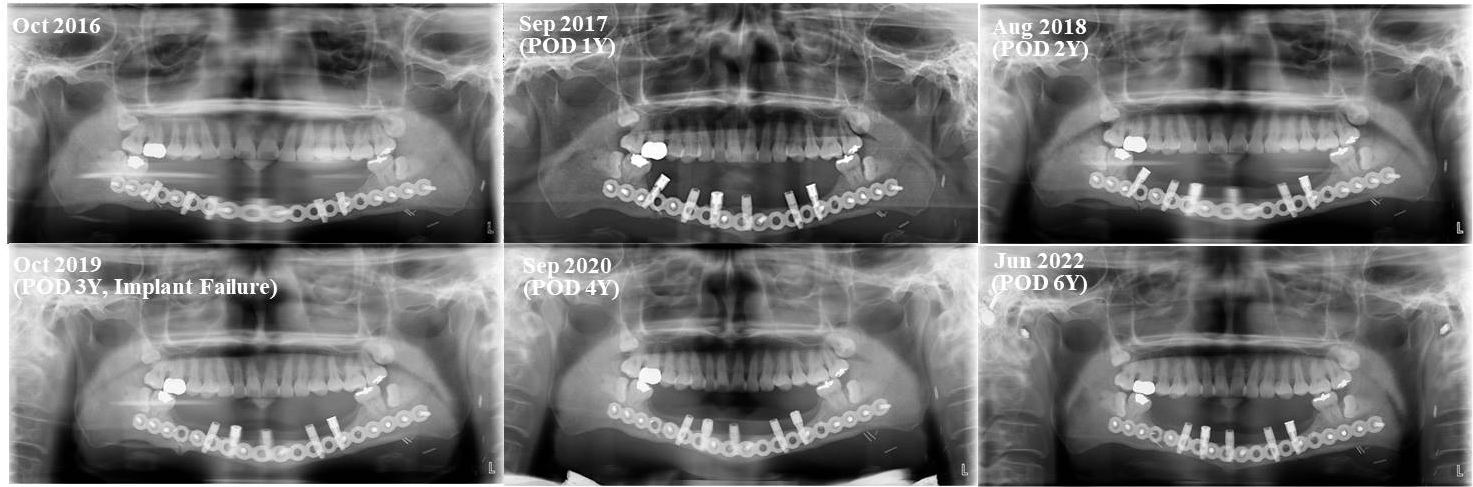
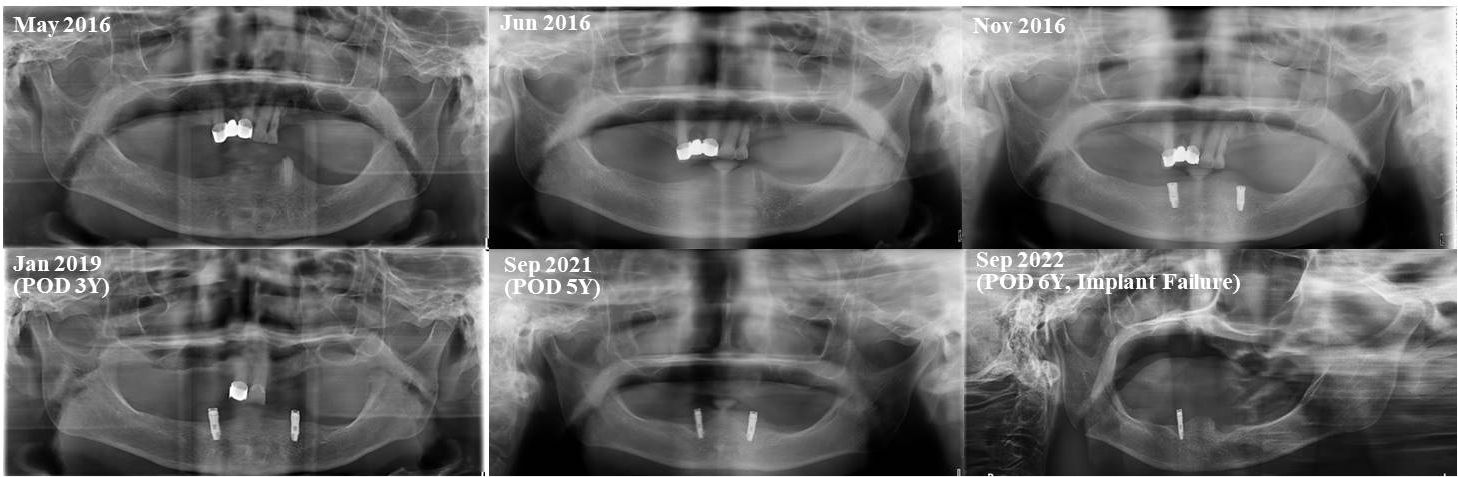
Table 1.
Pearson’s chi-squared test for categorical data and survival rate. The correlation between categorical data and survival rate is verified through Pearson’s chi-squared test. There is a correlation between the number of implants and implant survival rate; however, all other variables are not significant
| Categorical data | Conditions | Survival | Failure | Total | p-value |
|
Age (year) | < 60 | 38 | 1 | 39 | > .576* |
| 60 ~ 69 | 34 | 1 | 35 | ||
| 70 ~ 79 | 55 | 0 | 55 | ||
| > 80 | 17 | 0 | 17 | ||
| Gender | Male | 52 | 1 | 53 | .685 |
| Female | 92 | 1 | 93 | ||
| Placement location | Mn. Ant. | 105 | 2 | 107 | .864 |
| Mn. Post. | 4 | 0 | 4 | ||
| Mx. Ant. | 30 | 0 | 30 | ||
| Mx. Post. | 5 | 0 | 5 | ||
| Number of implants | 1 | 2 | 0 | 2 | .019** |
| 2 | 47 | 1 | 48 | ||
| 3 | 18 | 0 | 18 | ||
| 4 | 72 | 0 | 27 | ||
| 6 | 5 | 1 | 6 | ||
| Total | 144 | 2 | 146 |
2. Success rates
The overall success rate was 95.9%. Among the 146 implants placed for implant overdentures, six had more than 2 mm radiographic bone loss from the initial surgery. Among the patients with more than 2 mm bone loss, two experienced pain during function, one had exudate leakage, and one required removal of the implant owing to severe
There was no statistically significant correlation between success rate and age (p = .651), sex (p = .877), implant placement location (p = .380), or the number of implants (p = .098). None of these variables showed a significant correlation with the success rate, as the p-value was greater than 0.05 for all variables (Table 2).
Table 2.
Pearson’s chi-squared test for categorical data and success rate. The correlation between categorical data and success rate is verified through Pearson’s chi-squared test. There is no correlation between all variables and the success rate
| Categorical data | Conditions | Survival | Failure | Total | p-value |
|
Age (year) | < 60 | 38 | 1 | 39 | .429* |
| 60 ~ 69 | 32 | 3 | 35 | ||
| 70 ~ 79 | 53 | 2 | 55 | ||
| > 80 | 17 | 0 | 17 | ||
| Gender | Male | 51 | 2 | 53 | .877 |
| Female | 89 | 4 | 93 | ||
| Placement location | Mn. Ant. | 102 | 5 | 107 | .111 |
| Mn. Post. | 3 | 1 | 4 | ||
| Mx. Ant. | 30 | 0 | 30 | ||
| Mx. Post. | 5 | 0 | 5 | ||
| Number of implants | 1 | 2 | 0 | 2 | .098 |
| 2 | 44 | 4 | 48 | ||
| 3 | 17 | 1 | 18 | ||
| 4 | 72 | 0 | 27 | ||
| 6 | 5 | 1 | 6 | ||
| Total | 144 | 2 | 146 |
Ⅳ. Discussion
In several previous studies, the 5-year survival rates of implants have been reported to range from 96.8% to 99.1%, while the 5-year success rates were reported as 95% to 97%.11, 12, 13, 14, 15 The 5-year survival and success rates of implants for overdentures were reported as 93% to 97%.16, 17, 18, 19, 20 Therefore, it has been found that the survival and success rates of implants for fixed prostheses and overdentures are similar, and the rates observed in the present study are consistent with those reported in previous studies.
In one patient, six implants were placed in the fibula for mandibular reconstruction, and one placed in the posterior area failed, resulting in an implant survival rate of 83.3% when considering only implants placed in the fibula. This is much lower than the 99.3% (139/140) survival rates of implants for overdentures placed in the alveolar bones. However, owing to the limited sample size, it is difficult to conclude that implants placed in the fibula have a lower success rate than those placed in the alveolar bone based on the results of this study. Other studies have reported no significant difference in survival rates between implants placed in the alveolar bone and those placed in the fibula. For example, Attia et al.21 reported a 97% survival rate of implants placed in the 34 fibula flaps transplanted after surgical reconstruction, while Sozzi et al.22 reported a 98% implant survival rate in a cohort of patients who underwent fibula free flap, with no statistically significant difference found in implant success rate between maxillary and mandibular implants or between radiated and non-radiated bone.
Based on the results of this study, there seems to be a significant correlation between the number and survival rate of implants (chi-square test p = .019). The only case in which six implants were placed for the overdenture were those placed in the fibula. As aforementioned, there is no significant difference in the survival rates between implants placed in the alveolar bone and those placed in the fibula.21, 22 Therefore, while it is possible to evaluate the impact of the number of implants on the survival rate by using it as the only variable, it is unreasonable to mention statistical significance because there is only one case with six implants placed. It was observed that the implant survival rate significantly decreases when six implants are used; however, there is no clear trend in survival rate with an increase or decrease in the number of implants. Furthermore, there was no significant correlation between implant survival rate when there were four or more implants compared to when there were fewer than four implants (p = .922). In previous studies with larger sample sizes, a higher number of implants was found to have a relatively higher survival rate.6, 18 Some studies on maxillary overdentures have claimed that having four or more implants is advantageous for both implant and overdenture survival rates.6, 23 Similarly, some studies have suggested that as the number of implants increases in the mandible, the implant survival rate also increases.9, 24, 25 However, a meta-analysis study on the number of implants and implant survival rates in overdentures found no correlation between the survival rates of four and six implants for maxillary overdentures.26 Another study showed that ITI implants supporting mandibular overdentures on two implants produced outcomes comparable to three or more implants.27 Additionally, several studies have reported a high success rate for two-implant overdentures. In contrast, some studies have found no significant differences in implant survival rates based on the number of implants.28, 29, 30 In summary, a higher number of implants generally results in less burden on individual implants and tends to increase the overall survival rate. However, the difference in survival rates is not necessarily significant. Therefore, surgeons should consider various factors such as the patient’s bone quality, quantity, and density; general condition; cost; and clinical time when determining the appropriate number of implants for a given case.
