

Ⅰ. Introduction
Currently, dental implants are commonly placed for the prosthetic treatment of edentulous patients. They have shown high success rates in meta-analyses.1 However, complications of implant failure have also been reported.2 They can be broadly divided into biological and mechanical complications. Biological complications include peri-implant mucositis, peri-implantitis, and marginal bone resorption, whereas mechanical complications include problems occurring in implant components and superstructures, such as screw loosening and fracturing.3 Mechanical complications appear more frequently than biological complications. The 5-year complication rates of single-tooth implant prostheses are 8.8% for screw loosening, 4.1% for prosthesis dislodgement, and 3.5% for prosthodontic material fracturing.4
Although the incidence of fractures of the abutment screw or abutment is lower than previously listed; it is also reported to be 0.5% over 5 years, with that of fractures of the abutment screw specifically being 0.3%. Internal type implants show less abutment-related complications than external type implants.5
When the abutment screw is fractured, various methods can be used to remove it.6,7,8,9,10 If the implant abutment screw is fractured at the upward position of the fixture, it can be removed easily by holding the fragment using a hemostat or tweezers.7 If it is fractured deep under the fixture, it can be removed using a probe, an endo file, or a scaler.8 If it is firmly connected to the fixture, a screw removal kit may be used.9,10
In some cases, screw removal using these methods is difficult. In these cases, careful grinding of the fractured screw can be attempted using a bur. However, internal threads of the implant may be damaged unexpectedly. Here, we introduce a method to restore an upper prosthesis using a cast post in an implant with damaged internal threads.
Ⅱ. Case Report
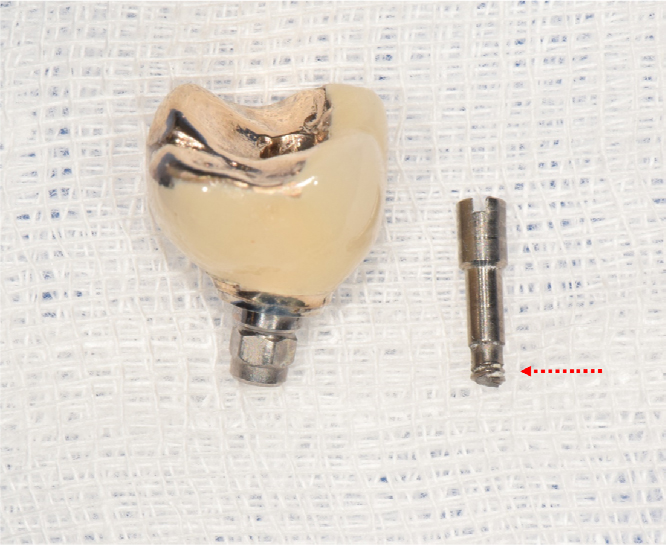
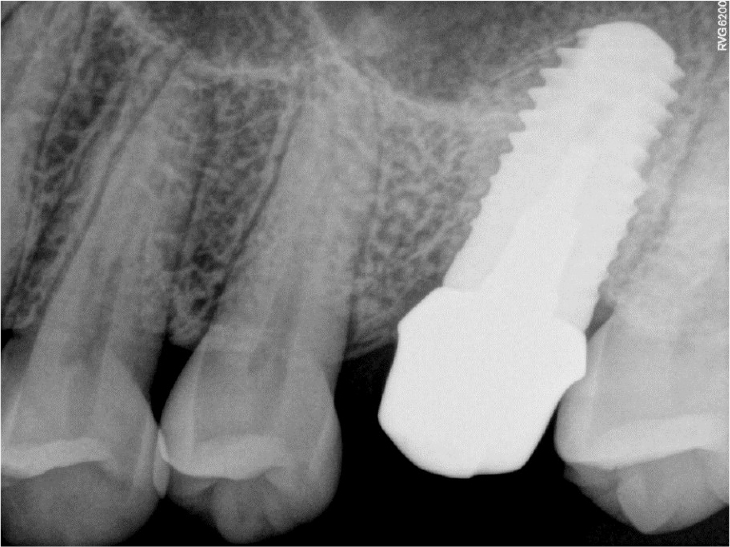
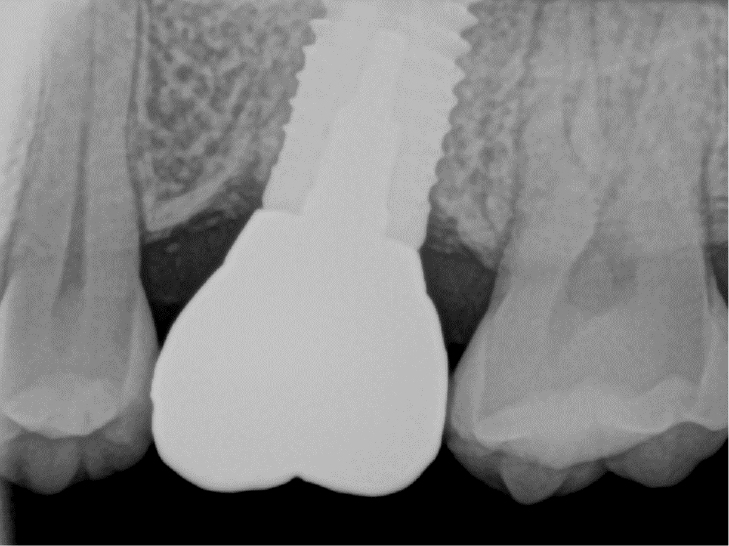
A 42-year-old female patient visited our dental clinic because of mobility of an implant prosthesis at the left maxillary first molar. According to the dental history, the implant (Xive® 5.5 × 11 mm; Dentsply Sirona, Charlotte, NC, USA) had been placed 10 years before at another dental clinic. A screw-retained porcelain-fused gold (PFG) prosthesis was connected to the patient. After retrieving the implant prosthesis, an abutment screw fracture was observed (Fig. 1).
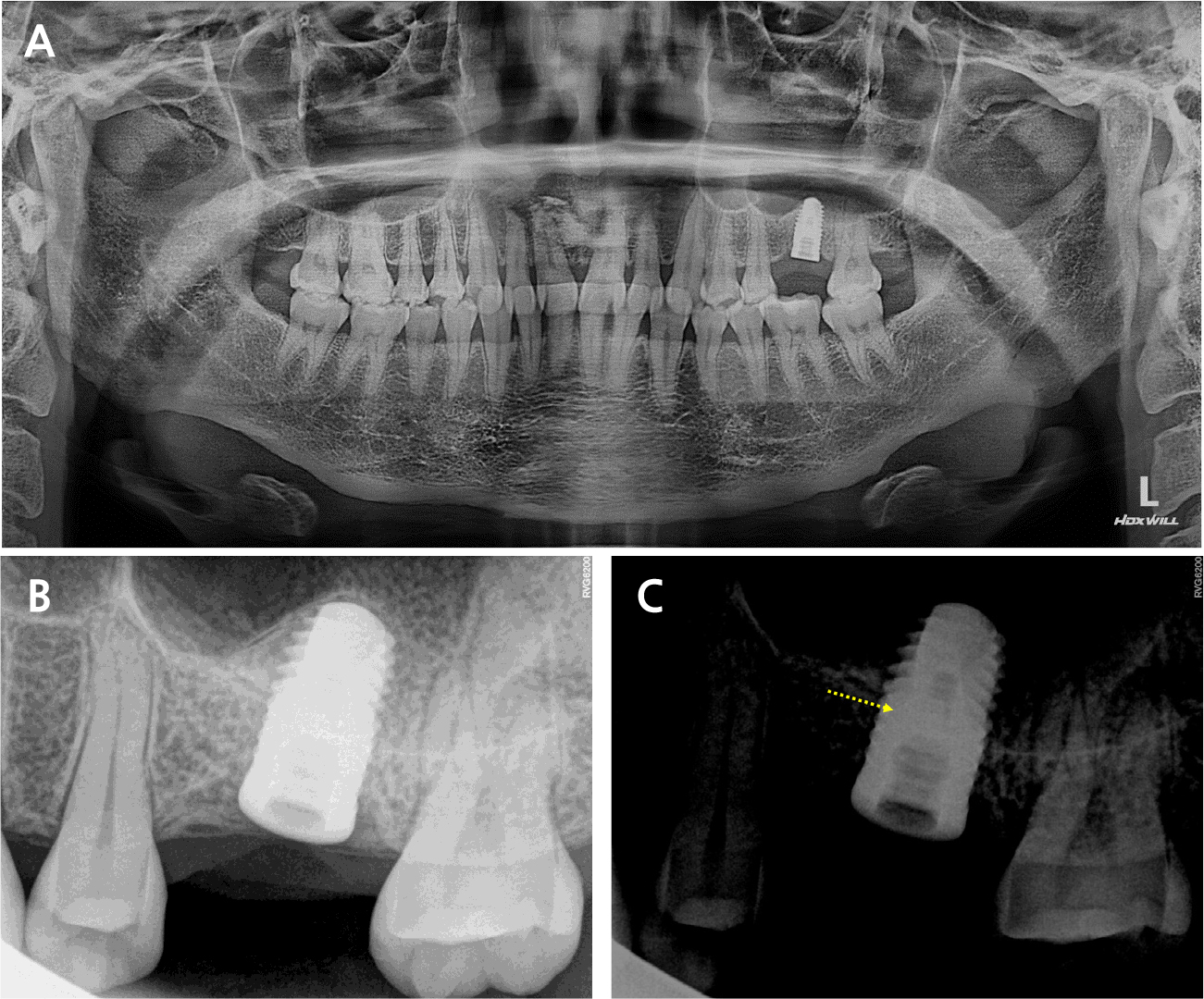
The radiograph revealed < 1 mm of marginal bone loss around the implant without inflammatory signs or peri-implantitis. The fractured screw left inside the implant was observed in the panoramic and periapical views (Fig. 2) and was located 7 mm deep from the soft tissue. An explorer, an ultrasonic scaler, and a removal kit (Neo SR Kit-II; Neobiotech, Seoul, Korea) were used for screw removal. However, the removal was difficult because the fracture was located at the first screw thread, and the remaining screw had been preloaded with torque. Sequentially, a high-speed handpiece with a 1/2 round bur was used to carefully remove the screw fragments remaining inside the implant fixture. The screw fragments inside the fixture were successfully removed, but the internal thread was damaged, and the healing abutment was not completely connected.
Therefore, removal of the implant and replacement with a new implant were inevitable. However, the patient had experienced a panic disorder, and so she refused to be covered with the sterile drapes and was anxious and apprehensive about the dental treatment. The procedure to remove the implant adjacent to the maxillary sinus was predicted to be a burden to the patient. Therefore, treatment options without removing the fixture were considered. The non-surgical restorative method of submerging the pre-existing implant and fabricating the three-unit fixed bridge was considered first.
However, since the adjacent teeth and implants were in a sound alveolar bone condition, we planned to fabricate a cast post restoration using the pre-existing implant. Before taking the cast post impression, the overgrown gingival tissue around the fixture was excised under local anesthesia, and a better field of view was secured.
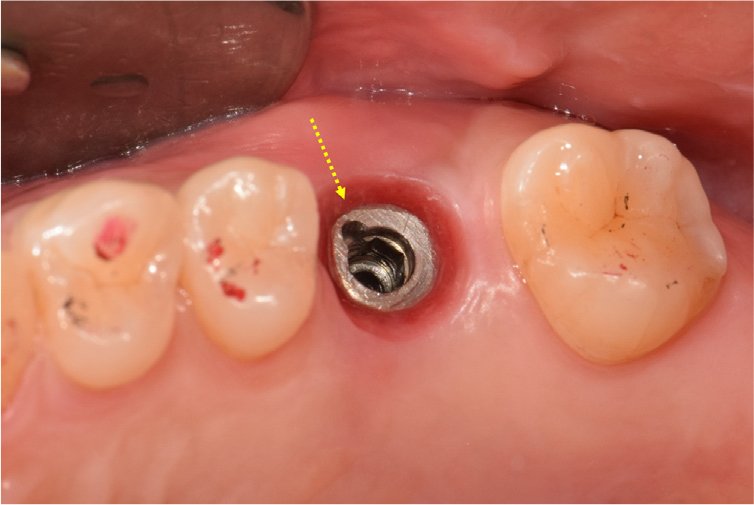
Subsequently, to prepare a space for the post, the inner surface of the fixture was prepared using a metal cutting bur (FG H34-012; Komet Dental, Lemgo, Germany) and a fine-grit round end taper diamond bur (TR 26F, 1.8 mm; Mani, Tochigi, Japan) in a high-speed handpiece (320,000 rpm) under water-cooling. In addition, a groove was formed on the fixture platform using a diamond bur to prevent horizontal rotation when connecting the post (Fig. 3).
The impression was taken with the indirect method of using a plastic impression post (Parapost® Green No. 7, 1.75 mm; Coltene/Whaledent, Altstatten, Switzerland) (Fig. 4) and polyvinylsiloxane (PVS) materials. The diameter of the impression post was similar to that of the bur used to prepare the inner surface of the fixture. In addition, an adhesive (V.P.S. tray adhesive; Kerr dental, Brea, CA, USA) was applied around the impression post to increase adhesion with the impression material.

The double mixing method using a metal tray was selected, with heavy- and light-viscosity impression materials (Imprint II Garant; 3M ESPE, Maplewood, MN, USA). After taking impressions, the inside of the fixture was temporarily restored with a temporary restoration material (Selection S-temp flow; Shinhung, Seoul, Korea) to the upper gingival margin. A temporary filling material was used instead of a healing abutment to prevent soft tissue overgrowth around the implant platform.
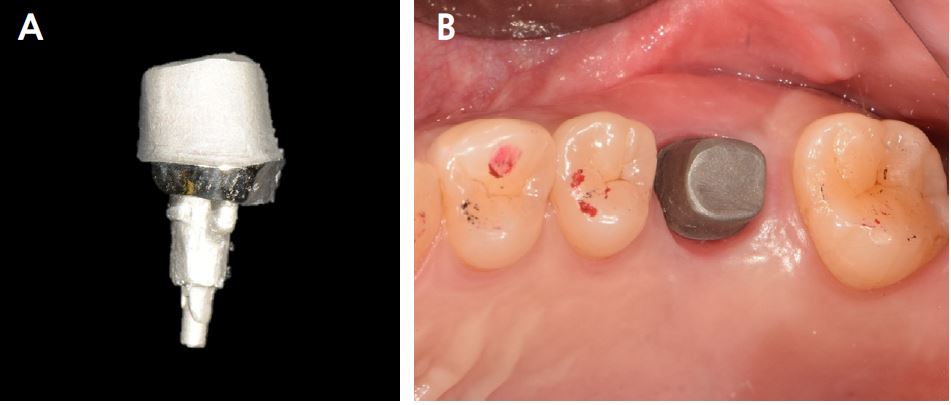
The acquired impression was poured with type IV gypsum, and a master cast was fabricated. The wax pattern of the cast post was designed and invested. Subsequently, it was burned out and cast with a nickel–chromium alloy (New Crown Metal; Ruby Dental, Osaka, Japan) (Fig. 5A).
At the next visit, the cast post was tried in (Fig. 5B), and the internal and marginal fits were checked clinically and radiologically (Fig. 6). The cast post was passively fit into the fixture, and the margin was set with an equigingival finish line. The upper prosthesis was made of a monolithic zirconia using the computer-aided design/computer-aided manufacturing (CAD-CAM) technique. The master cast was scanned with a model scanner (T500; Medit, Seoul, Korea), and the monolithic restorations were designed digitally, with narrow occlusal table width and minimal cusp inclination to minimize the offset load.
The zirconia prosthesis was tried in, and oral evaluation and adjustment were performed sequentially. Occlusion adjustment was performed according to the general concept of implant-supported prostheses. The occlusion was meticulously evaluated on a continuous basis to avoid the non-axial force vector that could lead to implant failure. At centric occlusion, the degree of the implant occlusal force was similar to that of the adjacent natural teeth.
After adjustment, the inner side of the fixture was rinsed with chlorohexidine and normal saline and dried using absorbent paper points (ProTaper Gold Absorbent Point; Dentsply Sirona). The cast post was bonded to the fixture with a resin-based cement (PANAVIA™ F 2.0; Kuraray Noritake Dental, Tokyo, Japan). Cement was applied to the post, and the post was seated in the post space with finger pressure. Excess cement was removed, and periapical radiographs were taken to check whether the cement had remained or not. The zirconia prosthesis was cemented with a resin-modified glass ionomer cement (FujiCEM® 2; GC Corporation, Tokyo, Japan) (Fig. 7).

Precautions after implant prosthesis delivery, such as avoiding hard and chewy foods, were explained to the patient. Periodic occlusion check was performed. At the 2-year follow-up, no implant complications, including detachment of the abutment or prosthesis, were observed (Fig. 8).
Ⅲ. Discussion
Mechanical complications of implant prostheses occur incidentally, and screw loosening and resulting screw fracturing are a main cause.11,12,13 To prevent complications related to the fractures of implant components, a series of processes, from diagnosis to restorations, should be accurately performed. In addition, even after the definitive prosthesis is set, an appropriate occlusion check should be performed through a regular recall check. Patient education is also important; since most implant screw failures precede screw loosening, when an implant mobility is detected, the patient should know to visit the dental clinic immediately to prevent screw fracturing.
In the present case, the patient did not undergo regular check-ups after implant treatment, and the loosened screw was left unattended for a long time, leading to a screw fracture. The maxillary and mandibular occlusal relationships showed a deep bite, and the causes of abutment screw fracture were assumed to be excessive functional and lateral forces and continuous repeated loads, leading to screw loosening. In such deep-bite cases, stable bilateral occlusion with an appropriate occlusal form that can protect the weak teeth is important.14 Left-side canine guidance was formed to minimize the lateral force applied to the implant.
Various methods have been reported to restore implant prostheses with a fractured abutment screw.6,7,8,9,10 When the abutment screw is fractured and removed without damaging the inner surface of the implant fixture, restoring the upper prosthesis is relatively easy by replacing it with a new abutment.
However, if the internal thread is inevitably damaged during removal, the abutment screw cannot be simply replaced. It is known in principle to remove the fixture when the internal thread is damaged. But the process of removal and placement of a new implant requires time and cost. Moreover, additional alveolar bone reduction might be inevitable to remove the fixture. The survival rate of these replanted implants is shorter than that of the initial implant.15
In this case, we fabricated a customized cast post and cemented a prosthesis for an internally damaged implant without removing the implant. This alternative method has been introduced in previous studies, within a 1-year follow-up.16,17,18,19
To prepare a space for the post, the inner surface of the fixture was prepared using a fine-grit round end taper diamond bur. The diameter of the prepared space was set similar to that of the existing abutment screw. It was measured on a periapical radiograph. The part corresponding to the head of the screw was widened using a metal cutting bur.
To prevent horizontal rotation of the cast post, an anti-rotation groove was formed on the fixture platform. This groove can be formed in the internal type implant with a platform or at the shoulder of the external type implant. These anti-rotational grooves are often used in cast posts on the natural tooth on a rational basis but rarely used in implants. Further studies are required to improve the level of evidence.
The cast post impression technique can be divided into two ways: direct method and indirect method. In previous studies,16,17,18,19 either the direct or indirect method was selectively used according to the clinician’s preference. In the present case, the impression was obtained with the indirect method using a plastic impression post. The diameter of the impression post was similar to that of a bur used to prepare the inner fixture.
Cast post cementation was performed using a self-cure resin-based cement, which contains methacryloyloxydecyl dihydrogen phosphate (MDP) to improve its bond strength with titanium.20 This cement was selected on the basis of previous case reports.16,17,18,19 The pumping action before complete seating of the post in the post space ensured the release of air bubbles entrapped and coronal displacement of excess cement.
This alternative method has the advantage of short treatment period, lack of surgery risk to the patient, and low cost. Therefore, this technique can be considered as an alternative method when the implant-surrounding bone and adjacent tooth are sufficiently healthy. At the 2-year follow-up, no mechanical or biological complications of the implant were observed. Further clinical studies and long-term follow-ups are required to prevent further complications, such as loosening or fracturing of the custom cast posts.
