

Ⅰ. Introduction
The success of the use of single implant to restore mandibular second molar has been a topic of debate. When the second molar is missing, the cantilever and removable partial denture is not generally preferred because of the biomechanics. To prevent eruption of the opposing tooth and ensure a balanced occlusion, single implant would be a favorable treatment to replace the mandibular second molar.1 With respect to its function, 90% of the masticatory efficiency occurs in the mesial half of the mandibular first molar, and the second molar is not significantly used for mastication. Moreover, it is not a suitable condition for implant. As per reports, the occlusal force per root surface was greatest on the posterior region, especially the occlusal force of the mandibular second molar area was 10% greater than that of the mandibular first molar.2 Also, when the mandibular second molar area is associated with lateral movement, it is close to condyle fulcrum and receives a large lateral force.3,4 Implants could be vulnerable to lateral force, thereby rendering osseointegration difficult to achieve.5 Therefore, there is debate over the use of single implant treatment in mandibular second molar restoration.
To evaluate implant survival, it is necessary to understand the cause of the implants’ failure. Sakka et al. classified implant failure into four categories.6 The first is biological failure, which means the failure of osseointegration. The second is mechanical failure, which means the fracture of implant-related structures. The third is iatrogenic failure, which means that osseointegration is achieved, but the implant must be removed due to the surgical-anatomical failure. The fourth is adequate failure, which means that implant should be removed due to aesthetic dissatisfaction and psychological problems. In addition, biological failure can be classified into two types: early failure and late failure. There are several criteria for this division. Early failure is defined as failure before osseointegration is achieved. It means that the primary bone healing process is poor. It also occurs before the prosthesis is installed, or up to one year after implantation. Late failure is defined as failure to preserve osseointegration. It occurs after the prosthesis is installed, or more than one year after implantation. The causes of early failure include bone quality and quantity and the medical conditions of the patient. Late failure usually includes excessive loading, peri-implantitis, and inadequate prosthetic restoration.
There is only one study that detailed the cumulative success rate of single second molar implant. The study attributed a success rate of 95.1% to the procedure.7 However, it must be noted that the study was performed by multiple implantologists, and the maxilla and mandible second molar implants are mixed. So, from our knowledge, there is no study that describes the success of single implant for the restoring mandibular second molar. The purpose of this study was to evaluate the survival rate and risk factors of the mandibular second molar single implants which were performed by an experienced surgeon. The relationships between implant failure with implant length, diameter, and GBR were analyzed.
Ⅱ. Materials and Methods
This study included 137 patients (77 males and 60 females; 19~81 years old; mean age 53.6 years) who were treated with 147 single-tooth implant in the mandibular second molar region by an experienced surgeon between 2006 and 2019. This retrospective study was approved by the institutional review board (IRB) of the hospital (IRB no. S2022-2420-0001) and was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2000. The inclusion criterion for this study was that patients should have a missing single second molar with a healthy or well-controlled systemic disease. The exclusion criteria were bone targeting agents’ users, and uncontrolled systemic diseases.
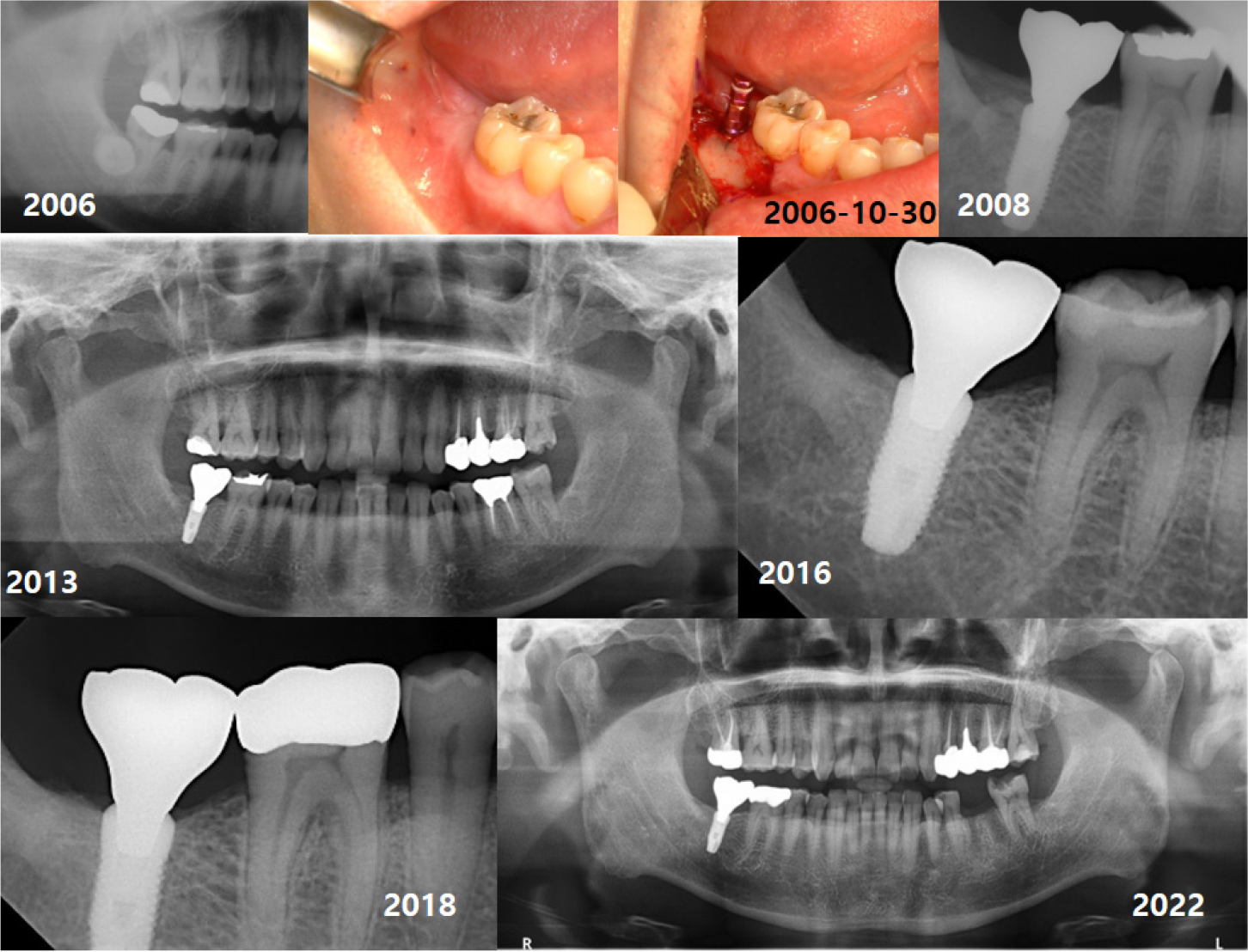
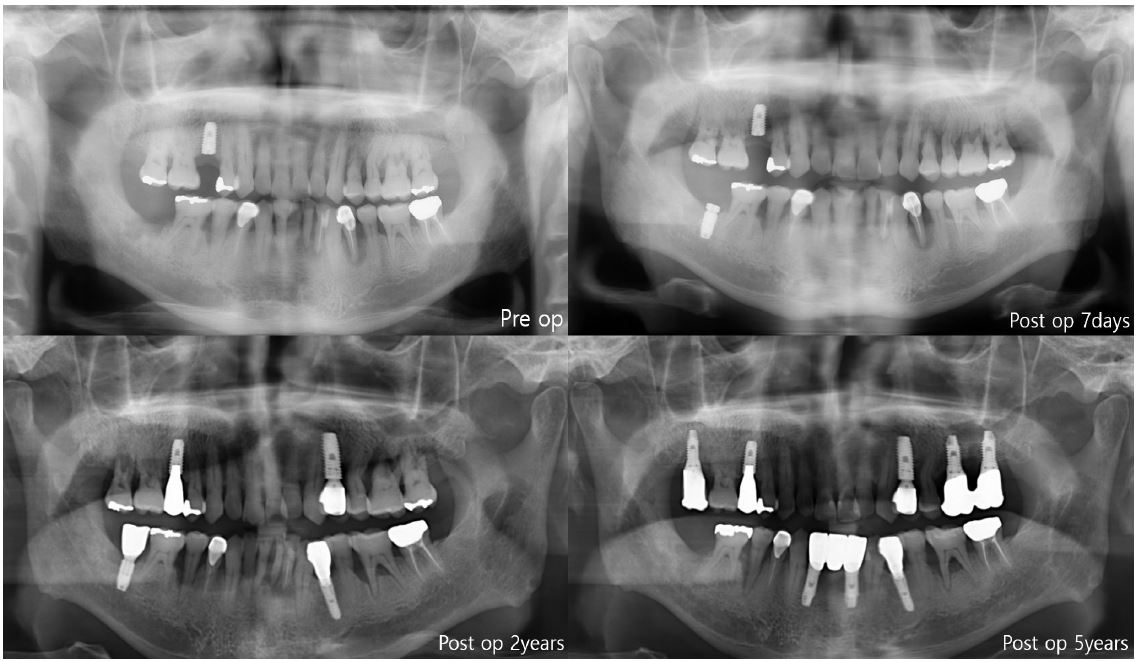
A total of 147 implants were placed in eight types (internal type: Implantium, Astra, Superline, TS III CA, Straumann, Luna, external type: Brånemark, US II), and all the implants were bone-level type. A second surgery was performed three months after first surgery in case of two-stage implants. Impression was taken two weeks after second surgery, and conventional prosthetic treatment was performed. Follow-ups were performed at three-month interval for the first year, then at six-month intervals for the next year, and then one-year intervals with panorama or periapical radiography (Fig.1). The criteria for implant survival was evaluated on the basis of four factors: absence of persistent pain, absence of mobility of implant, absence of continuous radiographic bone loss, and absence of uncontrolled exudate.8 The CSR was calculated using life-table analysis. Also, comparisons in CSRs between implant diameter and length, and GBR were performed using Log Rank test. p < .05 was considered significant.
Ⅲ. Results
Among the 147 implants, four implants failed. Thus, the five-year cumulative survival rate was 97.1% (Fig. 2). Among the eight types, Astra had the highest failure rate, accounting for three out of the four cases of failure (Table 1).
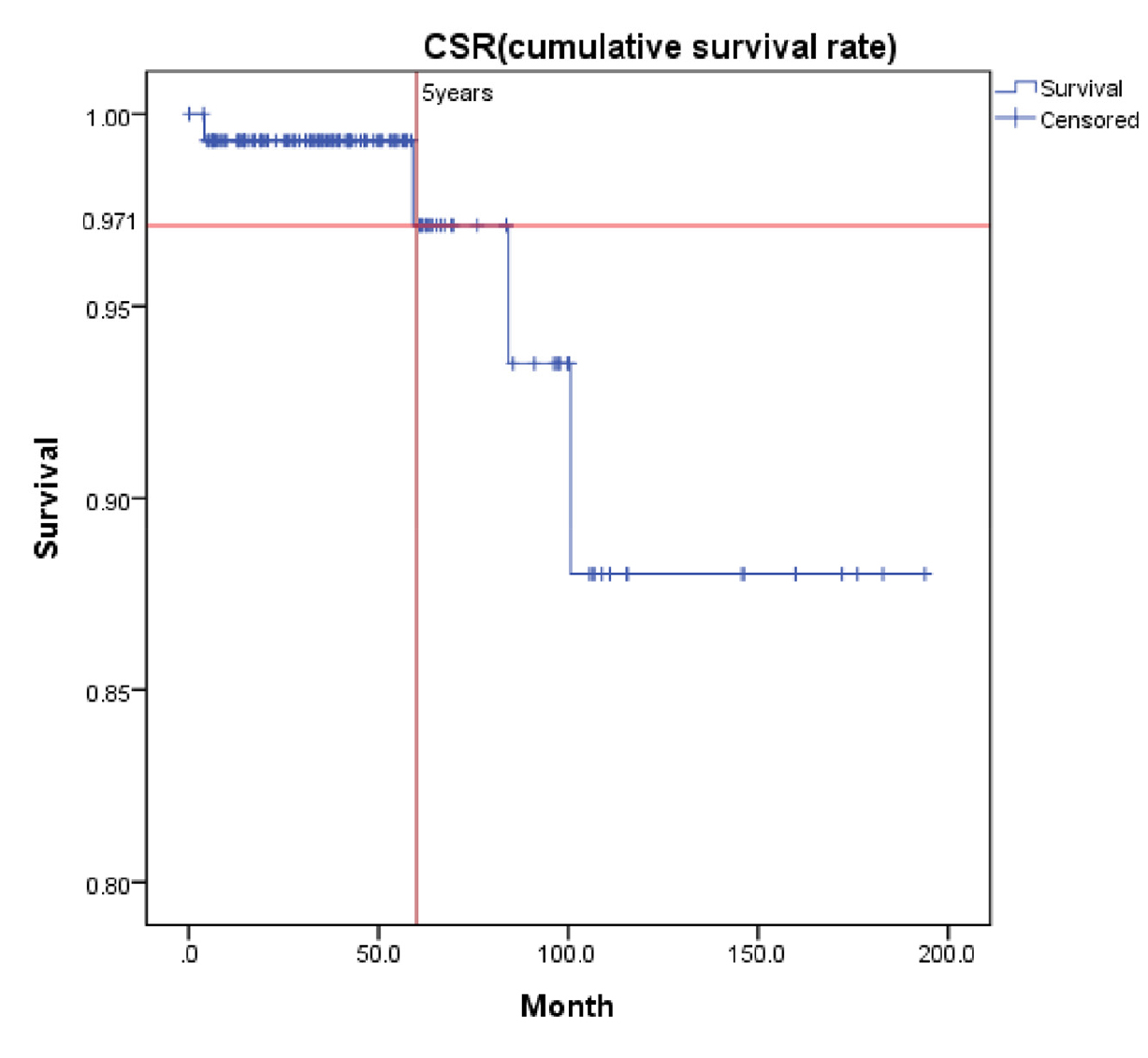
Table 1.
Comparison of implant survival rates according to implant type. In three out of the four failure cases, the implant type was Astra. In the other failure case, the implant type was Implantium
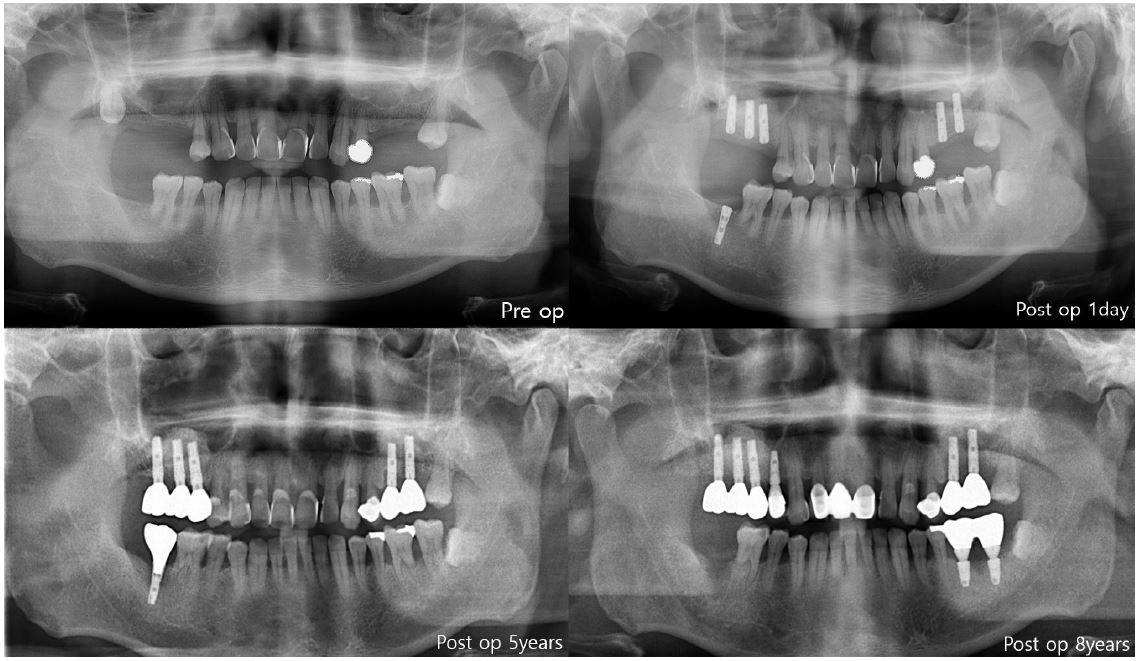
In the first case of failure, the patient had no specific medical history. The implant was removed at 6 years and 11 months (Fig. 3). In the second case, the patient had diabetes mellitus, and a smoking history. Also, GBR was performed with Xenograft and Bio-Oss. The implant was removed at 8 years and 3 months (Fig. 4). In the third case, the patient had radiotherapy history for tonsil cancer. The implant was removed at 4 years and 10 months (Fig. 5). In the fourth case, the patient had diabetes mellitus. The implant was removed, and another implant was immediately placed at four months (Fig. 6).
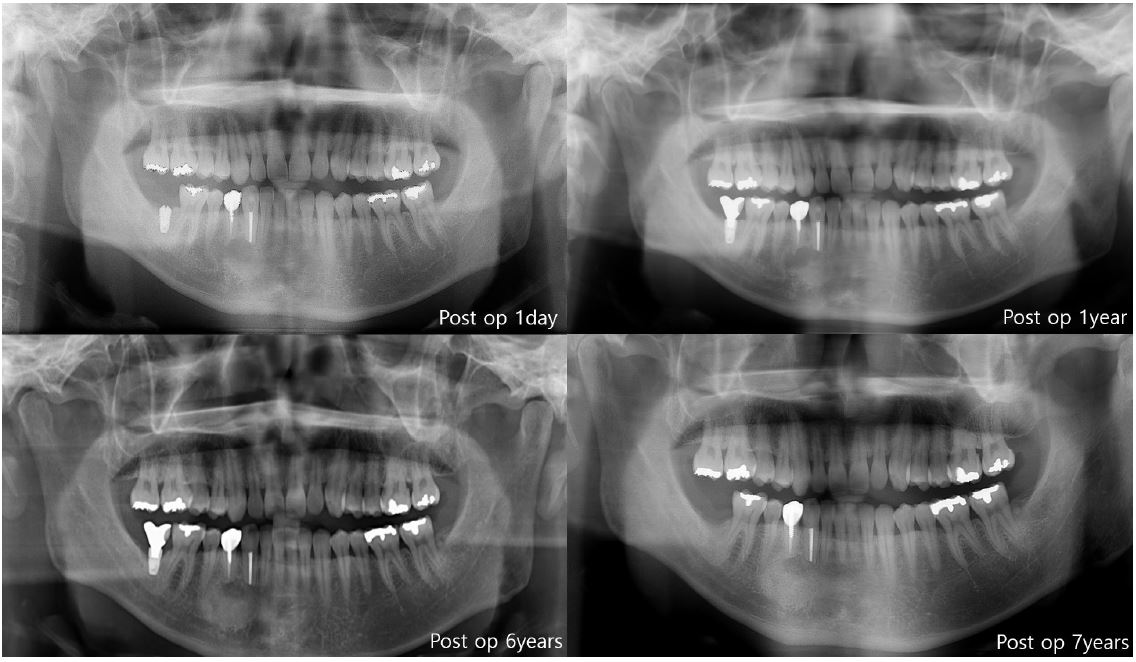
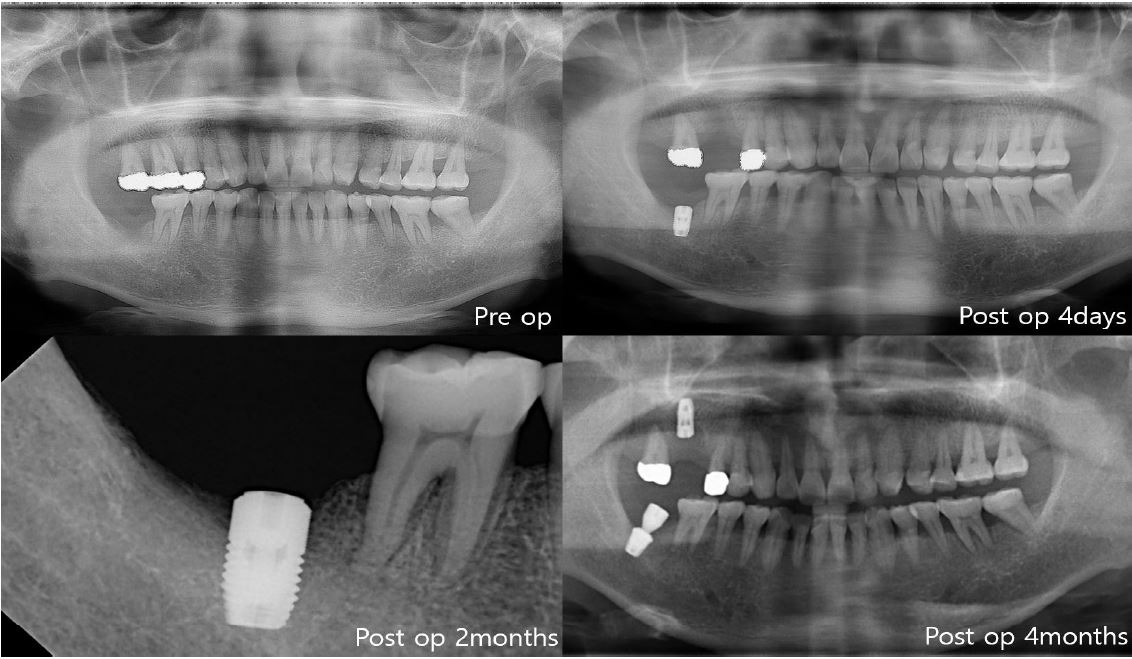
The first three cases of failure were classified as late failures. In one out of four cases, implant was removed at four months after implantation, and this was classified as an early failure (Fig. 6).
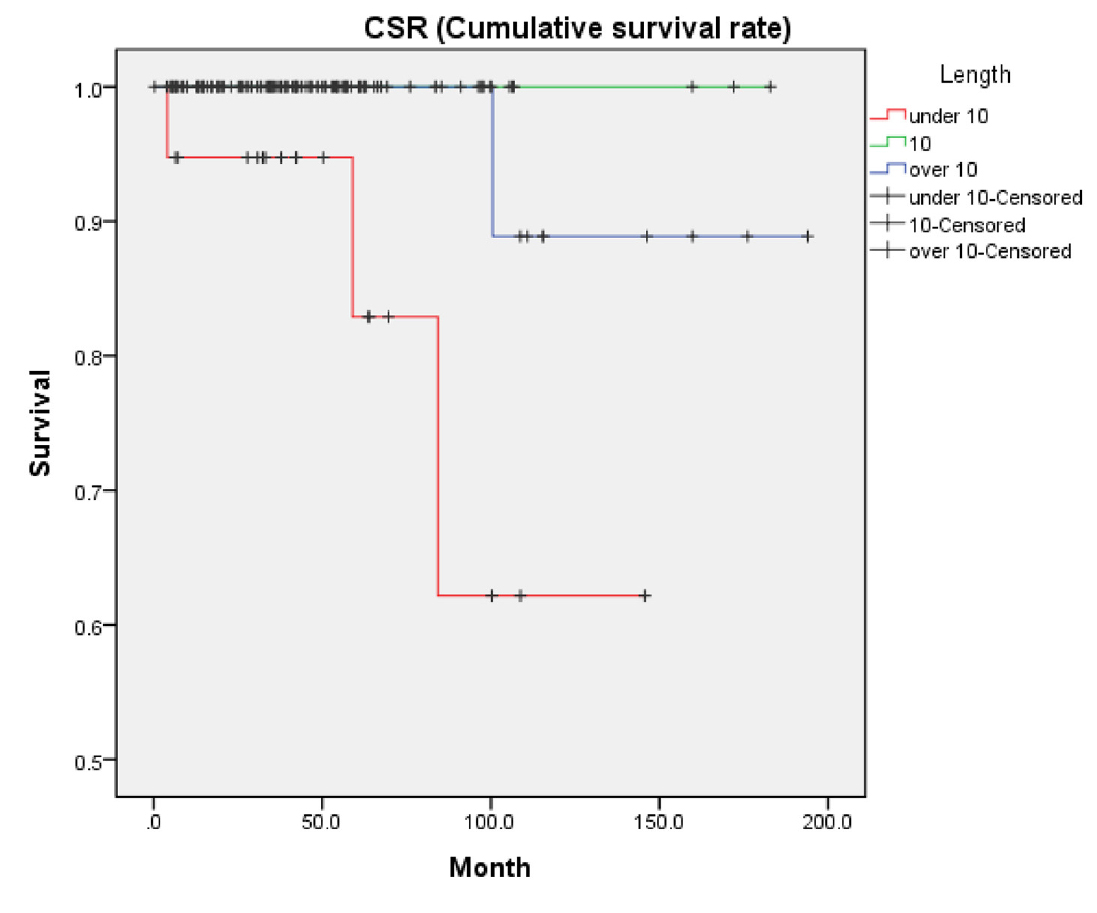
Implant length over 10mm was installed in 87.1% patients of this study (128 implants). Short implant under 10mm was installed in 12.9% of the patients. Among the four failed patients, three patients received implant length of 8, 9, 9 mm, respectively. The other patient underwent implant surgery with 13mm implant (Table 2). Upon analysis, a significant association was observed between implant length and CSR (p = .002) (Fig. 7).
Table 2.
Comparison of implant survival rates according to implant length. In three out of the four failure cases, the implant length was shorter than 10 mm (8, 9, 9 mm). In the other failure case, the implant length was longer than 10 mm (13 mm)
|
Implant length (mm) | Number | Fail | ||
| Number | Percent | |||
| <10 | 19 | 3 | 16 | 84.2% |
| 10 | 68 | 0 | 68 | 100.0% |
| >10 | 60 | 1 | 59 | 98.3% |
| Total | 147 | 4 | 143 | 97.3% |
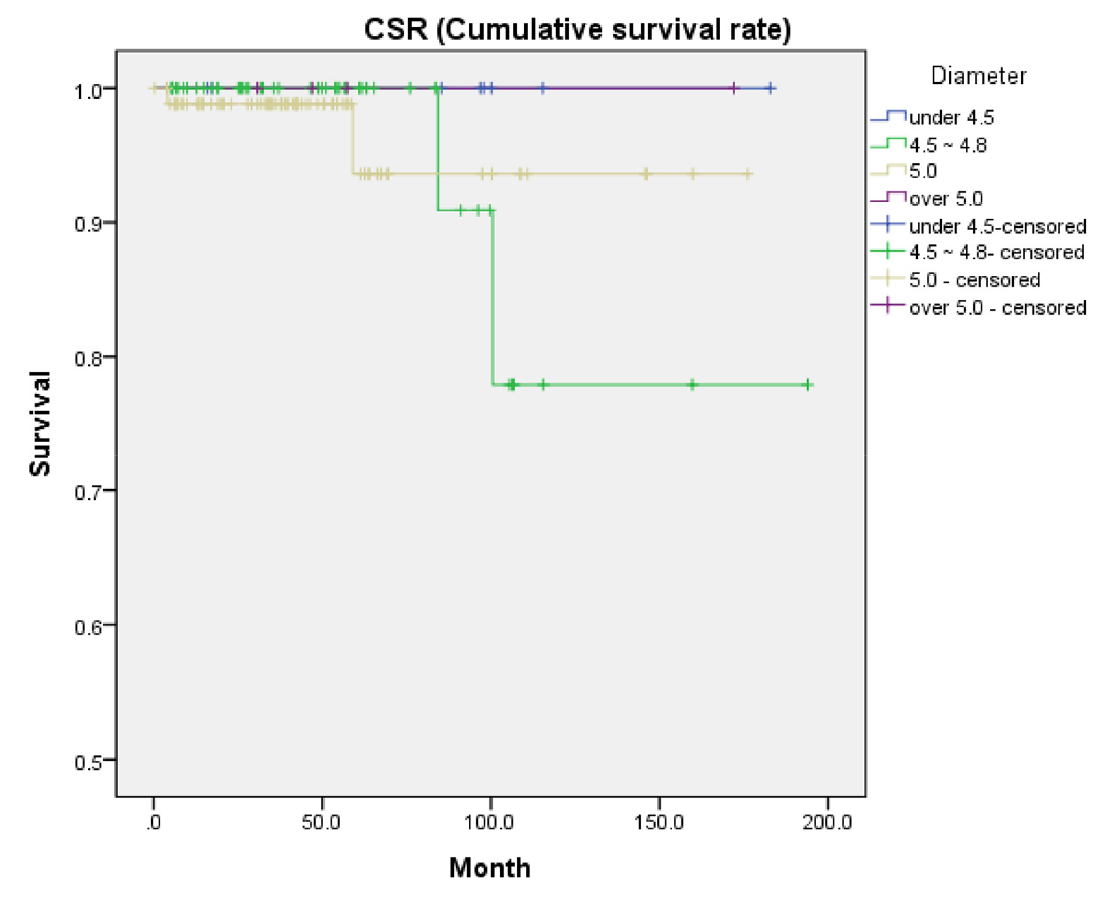
Among the four failed patients, two patients received implants wherein the diameter ranged from 4.5mm to 4.8mm, and the other two patients received implants of 5mm diameter (Table 3). Upon analysis, no significant association was found between implant diameter and CSR (p = .839) (Fig. 8).
Table 3.
Comparison of implant survival rates according to implant diameter. In two out of the four failure cases, the diameter is between 4.5 and 5 mm. In the other two cases of failure, the diameter is 5 mm
|
Implant length (mm) | Number | Fail | ||
| Number | Percent | |||
| <4.5 | 8 | 0 | 8 | 100.0% |
| 4.5~4.8 | 49 | 2 | 47 | 95.9% |
| 5 | 86 | 2 | 84 | 97.7% |
| >5.0 | 4 | 0 | 4 | 100.0% |
| Total | 147 | 4 | 143 | 97.3% |
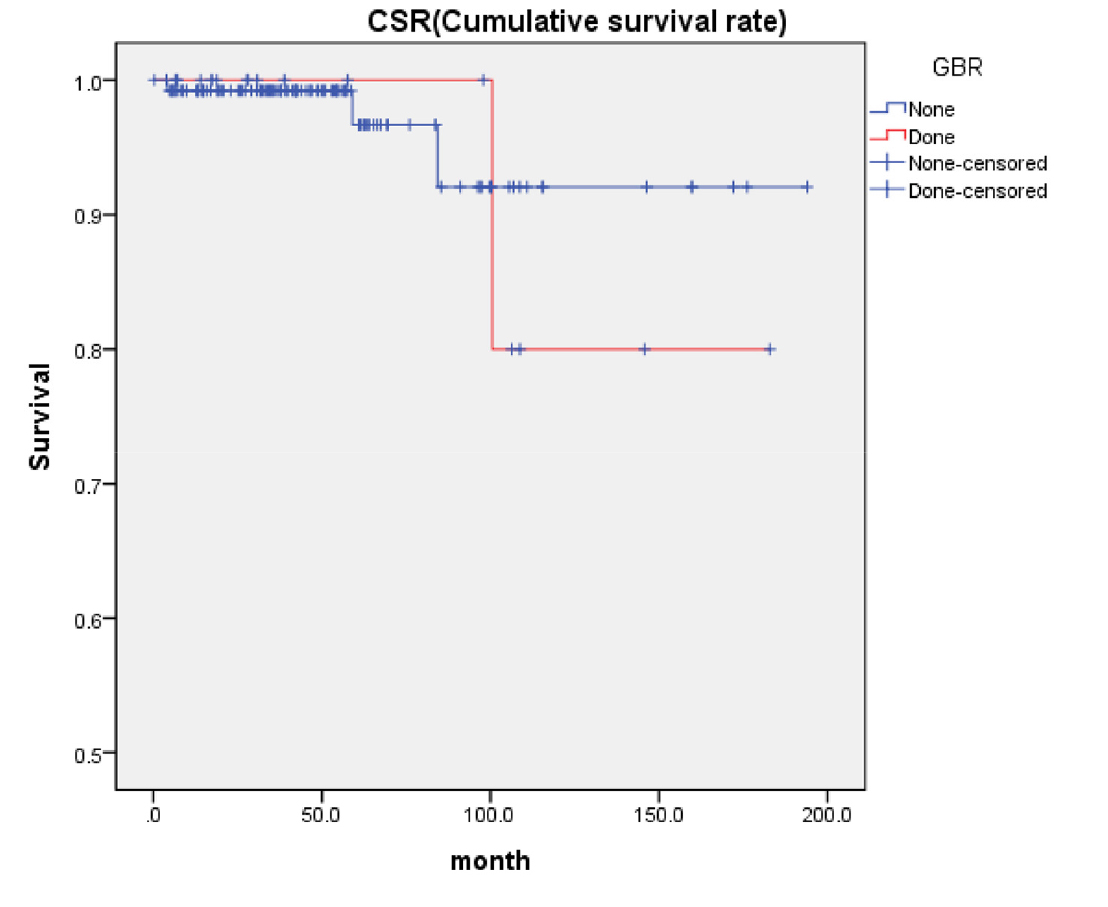
Among the four cases of failure, only one received GBR procedure during implantation (Table 4). Upon analysis, no significant association was found between GBR and CSR (p = .771) (Fig. 9).
Ⅳ. Discussion
Single tooth implant replacement constitutes a major portion of all implant treatments, accounting for 28% of all implant treatment in dentistry.9 The best advantage of single tooth implant is that it preserves the adjacent teeth. Besides, it also prevents complications associated with prosthetic treatment, such as periodontitis, risk of endodontic treatment, esthetics, and marginal compatibility. However, since single implants are not supported by adjacent structures, there could be an increased risk of failure when compared to multiple implants (Fig. 10A, 10B). The application of excessive force applied to implants may compromise osseointegration which is like traumatic occlusion.10 Single implant survival rate has been evaluated in previous studies. The survival rates were 96.5% and 97% respectively for a single implant as reported by Romanos and Goodacre.10,11 Lindh et al. meta-analyzed the results of nine studies on single implants in 1998 and reported a cumulative success rate of 97.5% for an average of six-year loading period. This analysis included a total of 570 implants.12 Jung et al. reported a cumulative success rate of 94.5% for single implants.13 Becker et al. reported a cumulative survival rate of 95% for posterior single-tooth implants.14 Misch et al. reported a cumulative survival rate of 98.9% from a 10-year retrospective study on posterior single tooth implants.15
As the distribution and strength of occlusal and lateral force are different in each tooth, the success rate for single implant could be different, depending on the implant location. The occlusal force of mandibular second molar area was 10% greater than that of the mandibular first molar.2 Also, when the mandibular second molar area has contact in lateral movement, it receives a large lateral force.3 If a third molar erupts normally, occlusal force in single implant in the involving the second molar could be distributed equally in both sides (Fig. 10C). However, as the second molar implant has no posterior teeth, all forces are applied to the implant (Fig. 10D).16 In addition, the bone of the mandibular molar region has low bone density than the mandibular anterior region.17 Therefore, the mandibular second molar single implant may have a higher risk of failure than the other single posterior single implants. In this study, four implants were removed. Three were late and one was early failure. As the mandibular second molar area experiences excessive loading and oral hygiene management is difficult, late failure may occur. In early failure cases, poor bone quality may contribute to the early failure of the implant.
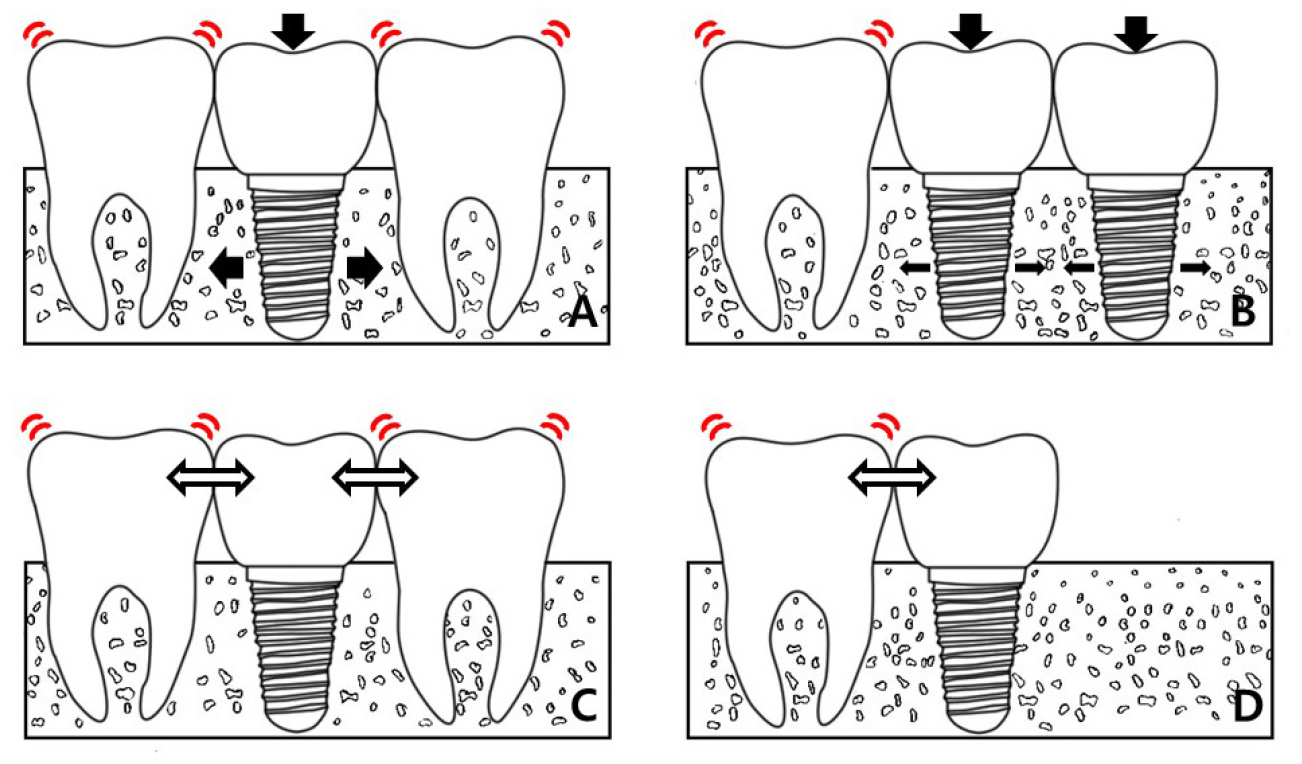
Fig. 10.
Distribution of force on implant. (A) Distribution of force in single implant, (B) Distribution of force in multiple implant, (C) Distribution of force in single implant with posterior teeth, (D) Distribution of force in single implant without posterior teeth. It is difficult to distribute forces in a single implant than in multiple implants (A and B). Moreover, in mandibular second molar single implant, it is difficulty to distribute forces as there are no posterior teeth behind the mandibular second molar (C and D).
Despite the many contributing factors, five-year CSR was 97.1% in this study. This was comparable or slightly better than previous studies involving single implants CSR. Therefore, in present results, the specific contributing factor of the single implant replacing mandibular second molar would not significantly impact on the survival rate.18,19,20,21,22 Also, the number of failures was small, so there was a limitation in finding accurate statistical significances.
There are several controversies on the association between implant survival and implant length. Misch et al. reported that implants shorter than 10mm have a high implant failure rate.8 Short implant is often implanted in the posterior region because of its proximity to the inferior alveolar nerve. Since stress distribution within the bone is biomechanically difficult to achieve in the short implant and heavy loading is also applied on the posterior region, there is an increase in the implant failure rate.23 Chang et al. also addressed that narrow implant diameter makes it more difficult to distribute stress to the bone.24 However, recent studies have reported that the length and diameter of implant may not affect implant failure.25 If short and narrow implants are selected because of proximity to nerve and limitation of bone quantity, the length and diameter could impact the implant survival.25,26 In this study, it was observed that implant length shorter than 10mm contributed to CSR. The reduced implant-to-bone area, poor bone quality and heavy occlusal loading are the major contributing factors for implant failure. In this study, implant diameter had no association with CSR. Nonetheless, it is important to note that narrow implant less than 3.5mm diameter was not installed.
Becker et al.27 and Fugazzotto et al.28 demonstrated that implant survival may not be significantly affected by GBR, when GBR is successful, and the initial stability is obtained. In this study, all the GBR cases were successful and stable in initial stability.
