

Ⅰ. Introduction
Sinus floor elevation via the lateral approach is a highly predictable and well-established procedure for rehabilitating the atrophic posterior maxilla. Perforation of the Schneiderian membrane remains the most frequent intraoperative complication. According to Yang et al., the incidence of membrane perforation is approximately 19%, and the presence of sinus septa increases this risk fourfold.1 Furthermore, Díaz-Olivares et al. reported an overall perforation rate as high as 30.6%.2 If not properly managed, these perforations can lead to graft migration, acute or chronic sinusitis, and ultimate implant failure.
Various surgical techniques have been proposed for managing this complication. The ‘Loma Linda’ pouch technique involves placing a resorbable collagen membrane over the perforation and folding it along the lateral window to create a protective pouch that contains the bone graft material.3,4 Another well-known approach, described by Fouad Khoury et al., is the ‘Khoury suture technique’, which involves directly suturing the torn edges of the Schneiderian membrane using fine resorbable sutures, often supplemented with fibrin glue or an additional barrier membrane for reinforcement.5
Although conventional approaches are effective, they present significant clinical challenges. Direct suturing is highly technique-sensitive due to restricted visual access and the fragile nature of the thin sinus mucosa, which is prone to further tearing under tension.2,5 Conversely, simply placing or folding a membrane often results in mechanical instability; during the physical packing of particulate bone graft materials, the membrane frequently rolls, folds, or is displaced entirely into the sinus cavity, thereby compromising the integrity of the repair.6,7
To overcome these critical limitations, a modified surgical technique utilizing a custom “handle” design for the resorbable collagen membrane is presented, combined with the strategic application of fibrin glue. This technical note details a step-by-step surgical procedure and demonstrates its clinical application in stabilizing the membrane, securing bone grafts, and promoting healing.
Ⅱ. Case Report
1. Surgical Procedure
The proposed technique is specifically indicated when Schneiderian membrane perforation occurs during the lateral-approach sinus floor elevation. The procedure begins with a lateral window osteotomy, in which the inferior border of the bony window is deliberately positioned approximately 2 mm above the actual sinus floor to facilitate optimal surgical access and subsequent bone healing. If a perforation is detected during elevation of the sinus mucosa, the operator carefully elevates the membrane further around the defect. This intentional elevation folds the surrounding tissue, effectively reducing the overall effective size of the perforation. To repair the defect, a resorbable collagen membrane was custom-cut to cover the area adequately. During this customization, one corner of the membrane was intentionally left protruding to create a distinct ergonomic “handle” shape.
Using surgical forceps or a dental pincette, the operator grasps this customized “handle” to smoothly insert and position the membrane over the defect within the sinus cavity. The handle allowed precise directional control and physically prevented the membrane from rolling inward or becoming lost in the cavity during insertion. Once positioned, a small amount of fibrin glue (Tisseel, Beriplast, or Green Plast) was applied to the edges of the membrane to firmly adhere it to the surrounding intact Schneiderian membrane and adjacent bony walls for initial stabilization. Subsequently, the particulate bone graft material was thoroughly mixed with fibrin glue to create a single, cohesive, putty-like graft mass. The cohesive mass was then gently packed into the sinus cavity, where its unified structure significantly resisted physical dispersion and prevented the graft particles from migrating through the repaired perforation. Finally, the lateral bony window that was removed during the initial osteotomy was repositioned at the surgical site. Additional fibrin glue was applied along the osteotomy margins to stabilize the repositioned window before the primary wound closure was achieved using routine suturing.
2. Case Presentation
A 71-year-old female patient presented to the Department of Oral and Maxillofacial Surgery with bilateral maxillary posterior sinus pneumatization. Systemically, she had hyperlipidemia and osteoporosis, with a history of denosumab (Prolia; Amgen, Thousand Oaks, CA, USA) injection 30 months before the planned surgery. Additionally, she was taking clopidogrel prophylactically (Plavix; Sanofi, Paris, France), which was discontinued 5 days before the surgical procedure following medical consultation. Tooth #26 was extracted 4 months before presentation. The right maxillary sinus was successfully treated using lateral sinus augmentation and implant placement. Lateral sinus augmentation and simultaneous implant placement at site #26 were planned for the edentulous left posterior maxilla.
Surgical procedures were performed under local infiltration anesthesia using 2% lidocaine with 1:100,000 epinephrine. Under intravenous conscious sedation with midazolam, a midcrestal incision was made, and a full-thickness flap was elevated (Figs. 1A and 1B). Perforation occurred during the lateral window approach and elevation of the Schneiderian membrane (Fig. 1C). A previously described modified surgical technique was immediately applied. During the procedure, the initial perforation of the Schneiderian membrane was intraoperatively estimated to be 5–7 mm in diameter (Fig. 1C). To reduce the defect size, the sinus membrane was elevated around the perforation site. This additional elevation allowed the surrounding tissue to fold, effectively reducing the functional size of the perforation to an estimated 3–4 mm, nearly half the original size. Subsequently, a resorbable collagen membrane was custom-trimmed to include a protruding “handle” measuring approximately 5 mm in length at one corner (Fig. 1D). By grasping the handle, the membrane was precisely directed into the sinus cavity and positioned over the perforation without rolling. Crucially, while the main body of the membrane completely covered the defect internally, the 5-mm handle was left resting on the external surface of the lateral bony wall, physically preventing the membrane from slipping inward (Fig. 1E). Fibrin glue (Tisseel; Baxter Healthcare Corp., Deerfield, USA) was used to stabilize the membranes. Considering the patient’s compromised bone metabolism, a synthetic bone graft material (Frabone; Inobone Co., Ltd., Cheonan, South Korea) and recombinant human bone morphogenetic protein-2 (Novosis; CGBIO Co., Ltd., Seoul, South Korea) were used to enhance osteogenesis (Fig. 1F). The particulate graft, rhBMP-2, and fibrin glue were thoroughly mixed to form a cohesive mass that was carefully packed into the subantral space without particle migration (Fig. 1G). During bone grafting, the implant was placed at site 26 (Superline II; Dentium, Suwon, South Korea), and a healing abutment was connected. The lateral bony window was repositioned and securely fixed using fibrin glue, followed by primary flap closure with 4-0 vicryl (Ethicon, Inc., Somerville, USA) (Figs. 1H and 1I).
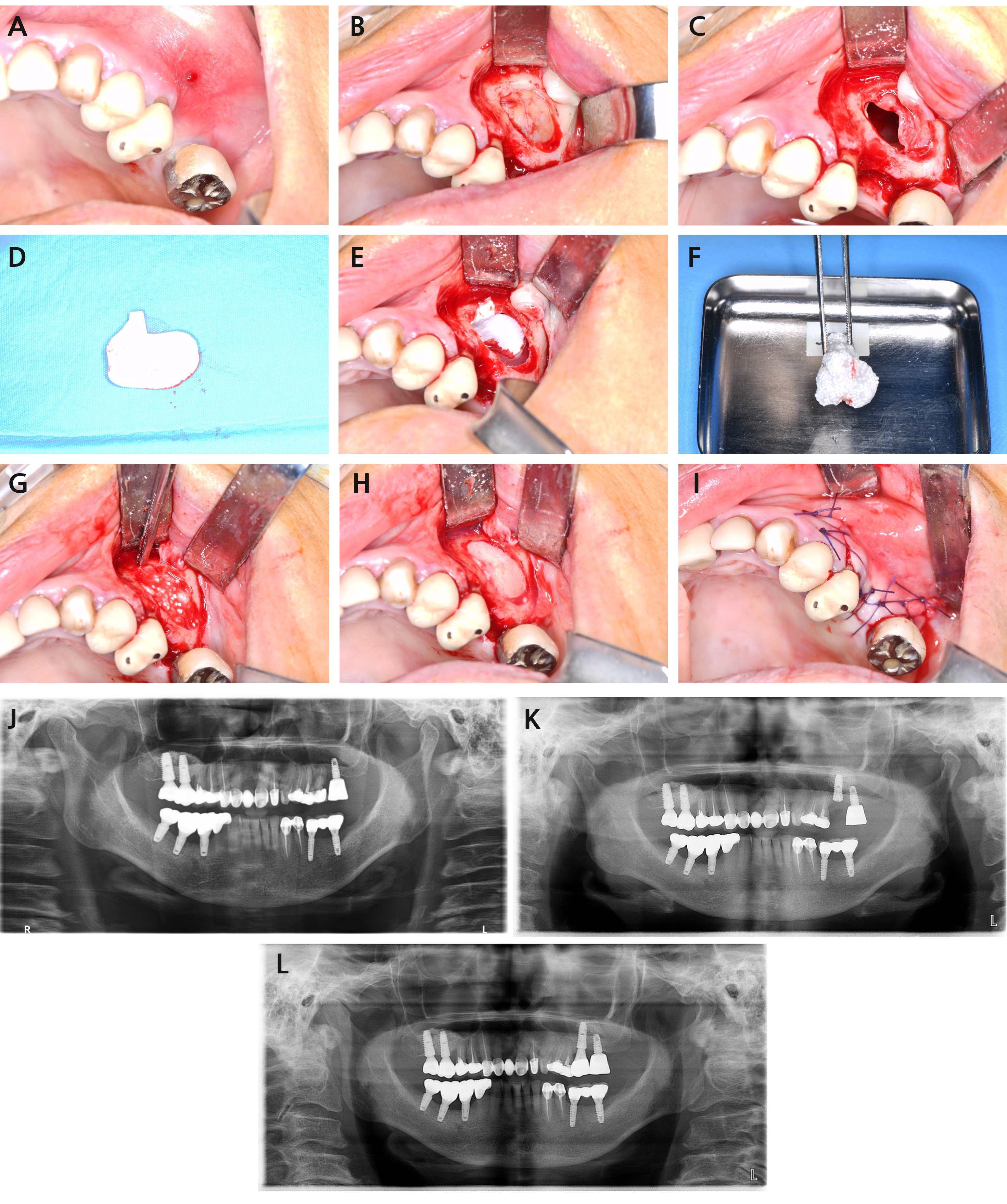
Fig. 1.
Intraoperative surgical sequence and radiographic evaluation of lateral sinus augmentation and perforation repair. (A) Preoperative occlusal view, (B) Bony window opening during lateral sinus augmentation, (C) Clinical view of the Schneiderian membrane perforation, (D) A resorbable collagen membrane customized to include a protruding “handle”, (E) Guided insertion of the customized membrane into the perforated sinus cavity via the handle, (F) Preparation of a putty-like cohesive graft mass, (G) Post-grafting view of the cohesive bone mass within the sinus, (H) The lateral bony window repositioned and initially stabilized using fibrin glue, (I) Flap repositioning and primary closure with sutures, (J) Panoramic radiograph taken 4 months preoperatively, prior to the extraction of tooth #26, (K) Panoramic radiograph obtained after lateral sinus augmentation surgery, (L) Panoramic radiograph obtained after final prosthesis delivery.
A rigorous postoperative sinus care protocol was followed to prevent displacement of the stabilized bony window and graft material. The patient was instructed to avoid blowing her nose for 4 weeks, sneeze with her mouth wide open, and refrain from using straws for 1–2 weeks to avoid sudden pressure changes within the sinus. Systemic decongestants including pseudoephedrine were prescribed to maintain nasal patency and prevent congestion-induced pressure spikes. These precautions, along with the internal support provided by the cohesive graft mass, ensured stable healing without displacement or graft leakage.
The postoperative healing was uneventful, with no signs of sinus complications. All sutures were removed two weeks postoperatively. Three months postoperatively, second-stage implant surgery was successfully performed, revealing stable clinical osseointegration and healthy peri-implant tissue. Immediate postoperative panoramic radiography revealed an initial graft height of approximately 15.2 mm, with no evidence of bone graft particle leakage into the maxillary sinus through the repaired membrane. After 6 months of healing, the remaining vertical bone height was measured at 13.3 mm, demonstrating stable maintenance of the augmented volume (Figs. 1J to 1L).
Ⅲ. Discussion
Successful management of Schneiderian membrane perforations is a critical determinant of long-term outcomes in sinus floor elevation.2 While various repair techniques have been documented, they often remain technique-sensitive and prone to mechanical instability during bone grafting.3,5 The “handle-designed” membrane technique described in this report offers three distinct clinical advantages that address the limitations of conventional methods.
First, the novel “handle” design effectively overcomes the chronic problem of membrane displacement or “rolling” into the sinus cavity.8 Unlike standard membranes used in the ‘Loma Linda’ pouch technique, which can be easily pushed inward during the physical packing of graft materials, the protruding handle allows the clinician to maintain continuous tactile and directional control.6,9 By grasping this ergonomic extension, the operator can precisely bridge the defect without the risk of the membrane losing its orientation or collapsing into the antrum. Furthermore, by intentionally elevating the surrounding sinus mucosa to reduce the “functional size” of the perforation, the tension at the repair site is minimized, enhancing the predictability of the barrier function. This technique may be applicable even for perforations exceeding 10 mm. In our clinical experience, although the reduction in functional size through additional elevation may be relatively small (approximately one-third of the original defect) compared to smaller perforations, the procedure may remain effective. However, further clinical validation is necessary to confirm long-term efficacy in such cases. The handle design provides the critical mechanical stability and tactile control necessary to prevent membrane displacement during the packing of extensive graft volumes in these challenging cases.
Second, the strategic integration of fibrin glue (Tisseel; Baxter, Deerfield, IL, USA) as a biologic adjunct provides both mechanical stability and regenerative benefits.10,11 Fibrin glue provides initial stabilization of the bony window without tacks, reducing potential risks associated with mechanical fixation devices.10 In this case, mixing the synthetic bone graft (Frabone; Inobone, Seoul, Korea) and rhBMP-2 (Novosis; CGBIO, Seongnam, Korea) with fibrin glue transformed the particulate material into a single, cohesive, putty-like mass.12,13 This “sticky bone” approach is particularly advantageous in perforation cases, as it prevents the migration of individual graft particles through the repaired site. In this 71-year-old patient with a history of osteoporosis and denosumab (Prolia; Amgen, Thousand Oaks, CA, USA) therapy, the use of rhBMP-2 was essential to compensate for compromised bone metabolism. The fibrin glue acts as a stable carrier matrix, potentially optimizing the localized release of growth factors and ensuring a scaffold for osteoinduction within the augmented space.
Finally, the application of fibrin glue to secure the repositioned lateral bony window simplifies the procedure and reduces surgical time. By eliminating the need for additional mechanical fixation devices, such as titanium tacks or meshes, this approach minimizes postoperative discomfort and the risk of complications associated with foreign bodies.9 This streamlined protocol represents a more ergonomic and patient-friendly alternative to complex suturing techniques, which are often limited by restricted visual access and the fragile nature of the sinus mucosa. To further clarify the clinical utility of this method, the advantages and disadvantages of various sinus membrane repair techniques have been summarized in Table 1. Compared to the Loma Linda pouch and Khoury suture techniques, the handle technique may offer a superior balance between mechanical stability and technical simplicity. Furthermore, whereas the intrasinus rigid fixation technique provides high fixation strength for large perforations, our approach may achieve comparable stabilization with significantly lower technical difficulty, making it a more accessible solution for a wider range of clinicians.8
Table 1.
Comparison of Sinus Membrane Repair Techniques
Despite these advantages, this technical note is limited by its single-case design and the lack of long-term histological evaluation to confirm the quality of the newly formed bone. Quantitative studies comparing the stability of “handle-designed” membranes versus conventional shapes are warranted. Nevertheless, the simplicity and mechanical reliability of this modified technique suggest that it may be a practical and predictable solution for managing sinus membrane perforations even in medically compromised patients.
Ⅳ. Conclusion
The modified membrane application technique, featuring an ergonomic “handle” design and the strategic use of fibrin glue, may provide a highly practical and straightforward solution for repairing Schneiderian membrane perforations. By enabling precise tactile control, it effectively prevents inward displacement of the resorbable collagen membrane during graft packing. Furthermore, the integration of rhBMP-2-enriched synthetic bone grafts with fibrin glue not only stabilizes the graft into a cohesive mass that prevents particle scattering but also allows for seamless, tack-free repositioning of the lateral bony window. Ultimately, this comprehensive approach may facilitate predictable and safe implant site development and have clinical value in the management of sinus membrane perforations.
