

Ⅰ. Introduction
Ⅱ. Materials and Methods
1. Specimen fabrication
2. Surface analysis using scanning electron microscopy
3. Fatigue strength test
Ⅲ. Results
1. Surface analysis using scanning electron microscopy
2. Fatigue strength test
Ⅳ. Discussion
Ⅴ. Conclusion
Ⅰ. Introduction
Zirconia is a ceramic material widely used in dentistry due to its excellent biocompatibility, high mechanical strength, and favorable esthetics.1 The demand for zirconia has particularly increased in recent years as a substitute material for dental prostheses, crowns, bridges, and even dental implants.2 To date, most zirconia prostheses have been fabricated using subtractive manufacturing (SM), in which pre-sintered zirconia blocks are milled. SM enables precise and consistent quality but is time-consuming, generates considerable material wastage, and has limitations in reproducing complex shapes.2,3
Additive manufacturing (AM) has emerged as an alternative to address these limitations. AM fabricates objects by successively stacking slurry-based layers, allowing efficient production of complex geometries while minimizing material waste.4,5 Among AM techniques, stereolithography (SLA), which polymerizes each layer with a laser, and digital light processing (DLP), which cures an entire layer simultaneously using a digital projector, are primarily employed for zirconia ceramics.2,6 SLA offers high precision but relatively slower curing, whereas DLP enables faster printing and denser surfaces but may result in fine surface undulations.⁶
Recent studies have explored the fabrication of zirconia dental prostheses using AM systems. Cho et al. reported that the internal trueness of AM-manufactured crowns ranged from 26.47 to 48.23 µm.7 Furthermore, the flexural strength of 3 mol% yttria-stabilized tetragonal zirconia polycrystal (3Y-TZP) zirconia produced via three-dimensional (3D) printing exceeded the minimum requirement of 800 MPa established by the International Organization for Standardization (ISO) 6872 for monolithic multi-unit restorations.8,9,10,11 These results indicate that AM techniques possess adequate mechanical and geometric properties suitable for zirconia prosthesis manufacturing. Additionally, zirconia exhibits uniform shrinkage during sintering, enabling larger printed models to contract into highly accurate final forms.12 This property is particularly advantageous for fabricating small and complex dental components, such as implants.
Both SM and AM allow for customized manufacturing. AM offers the unique advantage of producing multiple identical specimens in a single build cycle, thereby enhancing the efficiency and cost-effectiveness of large-scale dental prosthesis production. However, in conventional zirconia 3D printing systems, the number of specimens that can be produced simultaneously remains limited due to restrictions in platform size and resin vat volume. Overcoming these limitations requires AM systems with larger platforms and high-resolution light sources. Therefore, further research is needed to assess the structural stability of zirconia dental prostheses fabricated using such large-area systems.
For the clinical application of zirconia implants, several requirements must be satisfied, including precise component fit, biocompatibility, and fatigue resistance under prolonged functional loading. The ISO specifies these requirements and the corresponding test methods for ceramic implants in ISO 13356:2015. If zirconia specimens produced with a large-area 3D printing system meet these standards, commercial-scale manufacturing of dental implants using AM would be feasible. Dental implants must endure repeated masticatory loads within the oral environment; therefore, their fatigue resistance under long-term cyclic loading is a critical determinant of clinical success.13,14
Accordingly, this study aims to evaluate the mechanical stability of zirconia specimens fabricated using a large-area AM system by assessing fatigue strength, thereby verifying their clinical applicability and exploring their potential for high-throughput production. The null hypothesis of this study states that zirconia specimens fabricated using a large-area AM system do not meet the fatigue strength requirements specified in ISO 13356:2015.
Ⅱ. Materials and Methods
1. Specimen fabrication
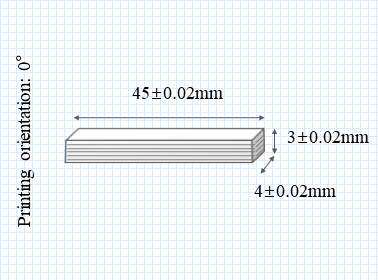
Rectangular zirconia specimens (4 mm × 3 mm × 45 mm) with 0.15 mm rounded edges were fabricated using a 3Y-TZP slurry (3DCERA; 3D Controls, Busan, Korea) via a 3D printing process. A total of seven specimens were prepared: five for fatigue testing and two for surface analysis using scanning electron microscopy (SEM) (Table 1).
Table 1.
Details of materials and processing methods
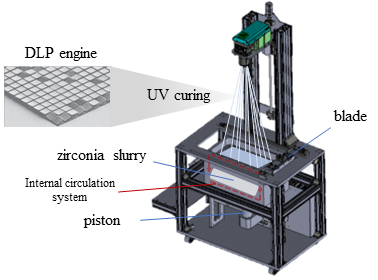
The specimens were printed using a custom-built, top-down digital light processing (DLP)-based 3D printer. This vat photopolymerization system employed a 3,840 × 2,160 resolution projection engine with a pixel pitch of 150 µm on the XY plane. The build size was 685 mm × 350 mm × 20 mm, providing a large-area platform that enabled the simultaneous fabrication of multiple specimens using this large-area system (Fig. 1). Print accuracy was optimized through a dual-blade recoating system, which ensured uniform layer spreading.
The slurry was selectively cured via photopolymerization at a build angle of 0° (Fig. 2). Layer slicing and build paths were configured using a proprietary slicing software (3D Controls Slicer; 3D Controls), and no support structures were generated. The layer thickness (Z-axis resolution) was set to 25 µm.
Following printing, uncured slurry was removed using a direct-spray cleaning device (C1; 3D Controls) to minimize damage to the green bodies. After drying, the specimens underwent debinding and sintering. The debinding process followed the manufacturer’s protocol, consisting of a temperature ramp from 165°C to 410°C over approximately 11.5 h, followed by sintering at 1,100–1,450°C for about 4.5 h (R0; 3D Controls) (Table 2).
Table 2.
Debinding and sintering protocol
| Debinding & Sintering Protocol | |||
| Set temperature (°C) | Heating rate (°C/min) | Holding time (h) | Total time (h) |
| 165 | 5.0 | 2.0 | 2.47 |
| 250 | 0.8 | 3.0 | 4.77 |
| 410 | 0.8 | 1.0 | 4.33 |
| 1100 | 6.0 | 1.0 | 2.92 |
| 1450 | 8.0 | 1.0 | 1.73 |
2. Surface analysis using scanning electron microscopy
Surface morphology and the presence of defects, including cracks or pores, were examined using a scanning electron microscope (Apreo S; Thermo Fisher Scientific, Waltham, MA, USA). To enhance electrical conductivity and image resolution, the specimens were gold-coated before imaging. SEM analysis was performed at an accelerating voltage of 10 kV, and images were captured at magnifications of ×1,000 and ×20,000.
3. Fatigue strength test
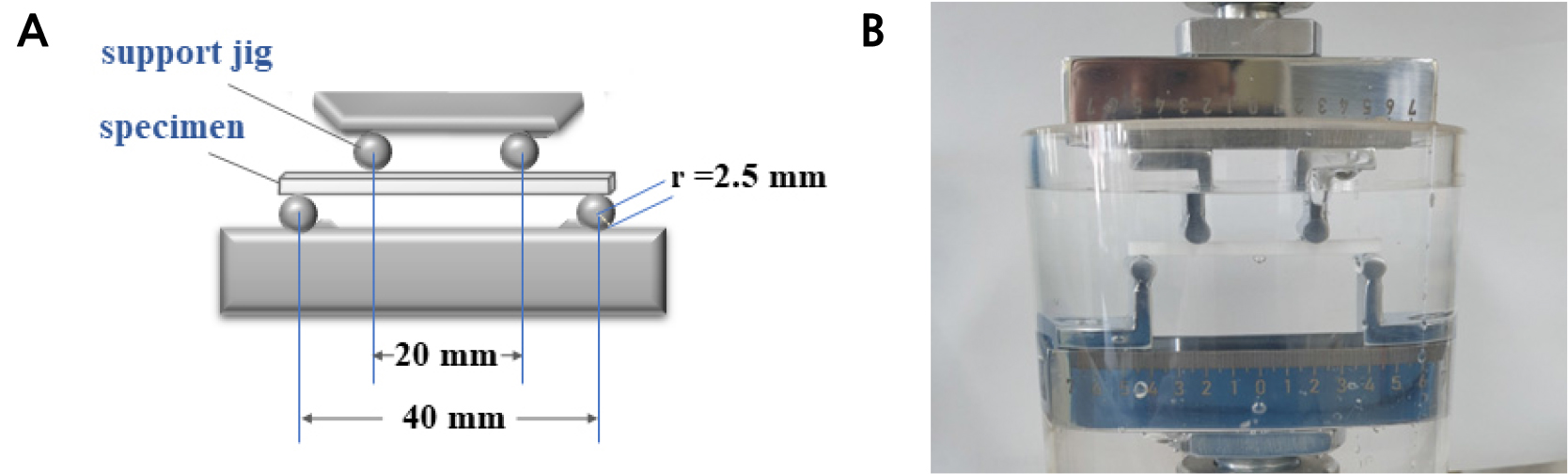
Fatigue strength was evaluated in accordance with ISO 13356:2015 standards. Testing was conducted using a universal testing machine (E-3000; Instron ElectroPuls, High Wycombe, UK) equipped with a four-point bending jig (Fig. 3A). The loading protocol applied a maximum stress of 320 MPa at a cyclic frequency of 12 Hz, with an R-ratio of 0.1, for up to 1,000,000 cycles.
During testing, specimens were immersed in 0.9% saline solution (Clean Two Injection; JW Pharmaceutical, Seoul, Korea), and the ambient temperature was maintained at approximately 23°C (Fig. 3B). Cyclic loading continued until specimen fracture or completion of the predetermined number of cycles. Specimens that did not fracture were classified as “survived”.
Ⅲ. Results
1. Surface analysis using scanning electron microscopy
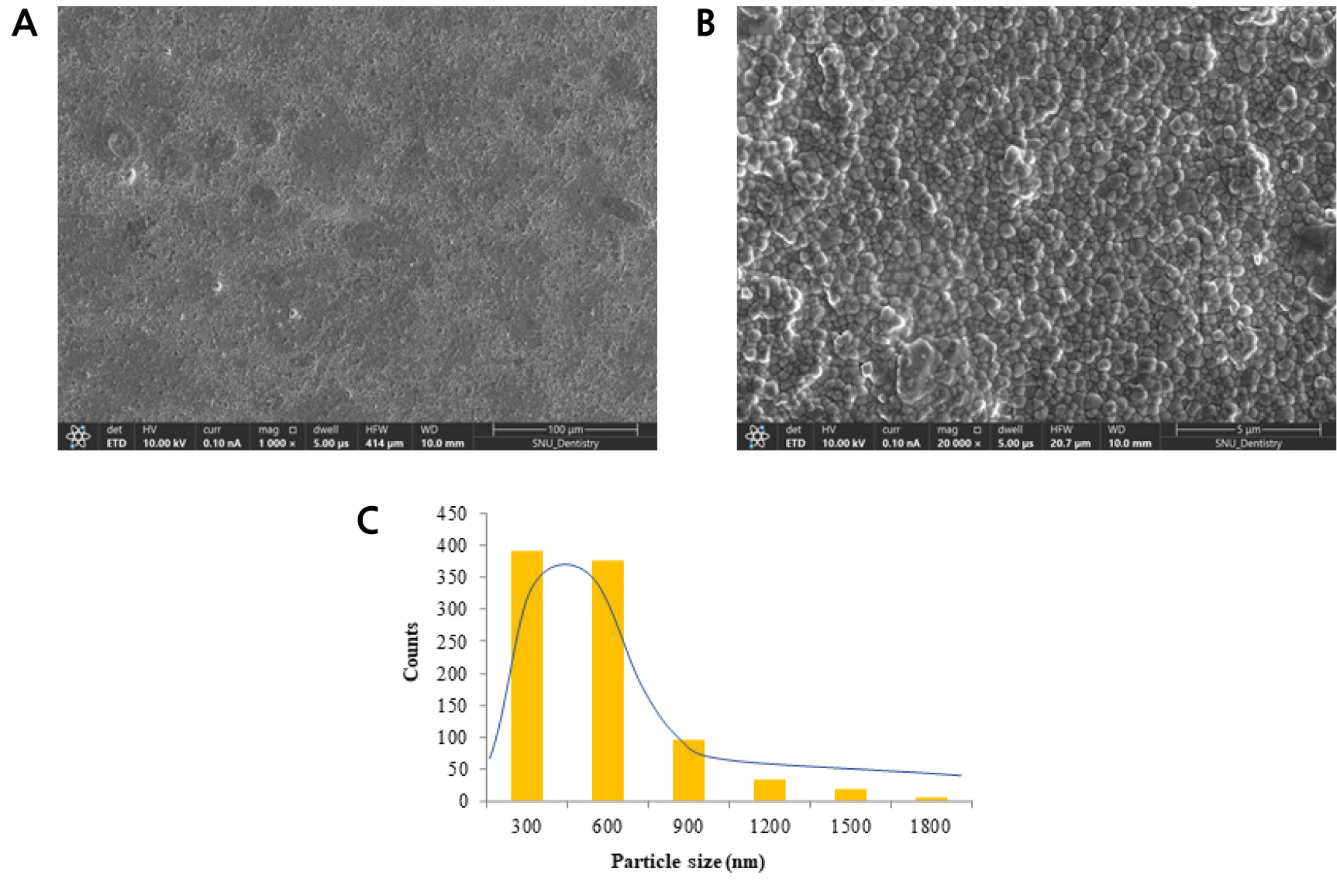
At low magnification (×1,000), no surface cracks or defects were observed, and the surfaces appeared relatively smooth and flat. At high magnification (×20,000), densely packed zirconia grains were identified (Fig. 4A and 4B). Quantitative analysis showed that 391 grains were < 300 nm, 378 were < 600 nm, and fewer than 170 grains were between 900 and 1,800 nm (Fig. 4C).
2. Fatigue strength test
All specimens survived cyclic loading without fracture or crack formation under the test condition of 1,000,000 cycles. No structural damage or failure was observed in any specimen (n = 5) (Table 3).
Ⅳ. Discussion
This study evaluated the surface microstructure and fatigue strength of zirconia specimens fabricated using a large-area AM system. Particularly, the possibility of achieving mechanical stability was examined with reference to the requirements specified in ISO 13356:2015 for ceramic implant materials.
Surface analysis showed no visible cracks or pores at low magnification (×1,000), and high-magnification imaging (×20,000) revealed a uniform distribution of fine zirconia particles. Grain size analysis demonstrated that most particles were smaller than 600 nm, indicating a relatively dense and homogeneous microstructure. Previous studies by Theunissen et al.15 and Wang et al.16 reported that smaller grain sizes can enhance mechanical properties. Consistent with these findings, this study suggests that fine grains contribute to improving the mechanical strength and fracture toughness of zirconia ceramics. Maintaining grain size within an optimal range is therefore critical for ensuring the structural integrity and mechanical stability of zirconia specimens fabricated using large-area AM systems.
The surface observed under low-magnification SEM corresponded to the top surface of specimens printed at a 0° orientation without any polishing or post-processing. The surface appeared generally flat with minor roughness. In conventional SM, zirconia blocks are milled from pre-compacted material, producing smoother surfaces.7 In contrast, AM builds structures layer by layer from a slurry, followed by debinding and sintering. Thus, the surface microstructure of AM products can vary depending on build orientation, particle size, and sintering conditions,17,18 potentially differing from that of milled implants. Surface roughness influences early biological responses such as osseointegration, cell adhesion, and protein adsorption,19,20 underscoring the need for further research on surface treatment strategies to enhance the biocompatibility of AM-fabricated implants.
In the fatigue strength test, cyclic loading was applied at a maximum stress of 320 MPa, a frequency of 12 Hz, and an R-ratio of 0.1 for 1,000,000 cycles. All specimens survived without fracture or crack formation, leading to rejection of the null hypothesis. These results meet the mechanical performance criteria outlined in ISO 13356:2015 and represent an equivalent of approximately 2–3 years of masticatory loading in the oral environment. Thus, zirconia specimens fabricated using this large-area AM system demonstrated the potential to ensure mechanical stability during the early stages of clinical application. This finding is consistent with André et al.,21 who reported that 3Y-TZP zirconia exhibited sufficient fatigue durability under cyclic loading in aqueous environments. However, to date, no studies have reported the fatigue strength of additively manufactured zirconia specimens. Furthermore, because all specimens in this study were fabricated at a fixed 0° build orientation, the results should be interpreted with caution. Prior studies have demonstrated variations in mechanical strength based on build orientation.22,23
Previous research on the fatigue strength of ceramic- or resin-based AM materials has suggested their suitability for short-term prosthetic applications, while highlighting their limitations under long-term occlusal loading. Travitzky et al.24 reported fatigue strengths of 200–400 MPa in alumina-based AM materials, indicating restricted applicability in dentistry. Similarly, Tahayeri et al.25 demonstrated that resin-based prosthetic materials exhibit fatigue limits of approximately 40–60 MPa, considerably lower than those of zirconia or alumina. In contrast, the zirconia specimens fabricated in this study using a large-area AM system satisfied ISO standards. These findings indicate that the large-area AM process does not compromise the inherent strength of zirconia, despite the expansion of the build platform. The ability to maintain mechanical performance while simultaneously producing multiple zirconia prostheses highlights both efficiency and reliability, carrying important clinical implications.
Compared with the SM method, AM offers structural advantages by enabling the simultaneous fabrication of multiple identical specimens in a single process. Particularly, the large-area system used in this study allowed for an increased platform size and vat volume compared with conventional commercial systems, indicating the potential for producing more specimens per batch. The development of such systems not only provides an alternative to traditional manufacturing techniques but also carries significant implications for improving process efficiency and industrial productivity in standardized medical devices such as dental implants. Therefore, the use of a large-area AM system to fabricate zirconia specimens may represent a viable technological alternative for the mass production of dental prostheses, thereby addressing critical needs in dental practice.
This study had some limitations. First, fatigue testing was conducted under laboratory conditions using saline solution at room temperature, which does not fully replicate the actual oral environment, where temperature fluctuations, saliva, pH variations, and microbial activity may affect implant performance. Second, owing to the standardization requirements of ISO 13356:2015, the test specimens were constrained in terms of fixation and geometry, and did not fully replicate the shape of clinical implants. Therefore, these findings should be interpreted with caution when extrapolated to clinical applications.
Future research should incorporate repeated testing under conditions that more closely simulate the oral environment and use specimens that replicate the actual shape of dental implants. Beyond fatigue strength, comprehensive and multifaceted evaluations of additional properties—including biocompatibility, surface roughness, implant–abutment interface stability, and long-term clinical outcomes after implantation—are essential. As further evidence accumulates, large-area AM technology has the potential to support both industrial-scale production of dental implants and high-precision, patient-specific manufacturing.
Ⅴ. Conclusion
Zirconia specimens fabricated using a large-area AM system exhibited surfaces free of pores and structural defects. Under the fatigue loading conditions specified by ISO 13356:2015 for ceramic implants, all specimens withstood testing without fracture. These findings suggest that large-area AM systems can meet the mechanical requirements of zirconia dental implants, particularly regarding fatigue resistance, thereby supporting their feasibility for clinical applications.
