

Ⅰ. Introduction
Treatment methods using dental implants include fixed prostheses, removable partial dentures (RPDs), and implant-supported overdentures.1 Among these, implant-supported fixed prostheses are preferred by patients because of their aesthetic appeal and psychological satisfaction.2 However, they have limitations such as the requirement of sufficient width and depth of residual alveolar bone and high costs.3 For patients with severe alveolar bone resorption, the use of implant-supported RPDs or overdentures may be more advantageous compared to fixed implant prostheses for lip support, hygiene maintenance, and stress distribution during mastication owing to the support, stability, and retention provided by the implants.4,5 Implant-supported overdentures use attachment devices, primarily categorized into solitary type and bar type.6 Compared with solitary attachments,7 bar-type attachment devices require a significantly larger interarch space and involve a more complex fabrication process. Nevertheless, they offer increased stability due to the splinting effect between implants, and additional attachments on the bar can enhance retention.8
The conventional fabrication process for bars is complex and requires jaw-relation registration after impression taking. However, recent advancements in computer-aided design/ computer-aided milling (CAD-CAM) technology have simplified the fabrication of milled bars.9 Moreover, to improve patient convenience, methods combining impression making and jaw-relation recording in a single step have been devised.
The JB Fork (PNUADD Co., Ltd., Busan, Korea) is a one-step jaw-relation record system that can be integrated with digital protocols for fabrication of dental prostheses. It allows for simultaneous impression-making, verification of the maxillary anterior tooth arrangement, and recording of vertical and horizontal jaw relations, thereby facilitating the establishment of the occlusal plane. This device consists of upper and lower plates, six upper anterior teeth, and screws. After obtaining the impressions of the overlapping areas on the upper and lower plates, screws are assembled to determine the vertical dimension and perform Gothic arch tracing. After the Gothic arch tracing, a small hole is created at the apex of the tracing using a round bur. A tray adhesive is applied to ensure the proper adhesion of the silicone bite-registration material (FUTAR D, Kettenbach GmbH & Co. KG, Eschenburg, Germany). This record can be integrated with the intraoral data (obtained using either intraoral scans or final impressions). Furthermore, facial scan data can be incorporated to generate a virtual patient that includes facial information. Compared with the conventional method, protocols using this device reduce the number of patient visits and save the time required for fabrication and adjustment of occlusal rims. Herein, we describe the case of a completely edentulous patient in whom aesthetic and functionally satisfactory results were obtained using the JB Fork to record the jaw relation for full-arch prosthodontic restoration using five maxillary and four mandibular implants, a milled bar with ADD-TOC attachments (PNUADD Co., Ltd., Busan, Korea), and zirconia prostheses fabricated using a CAD-CAM method.
Ⅱ. Case Report
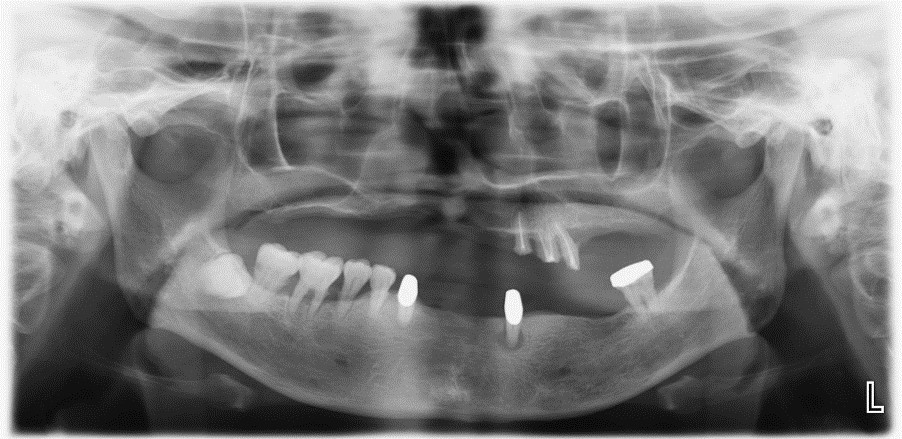
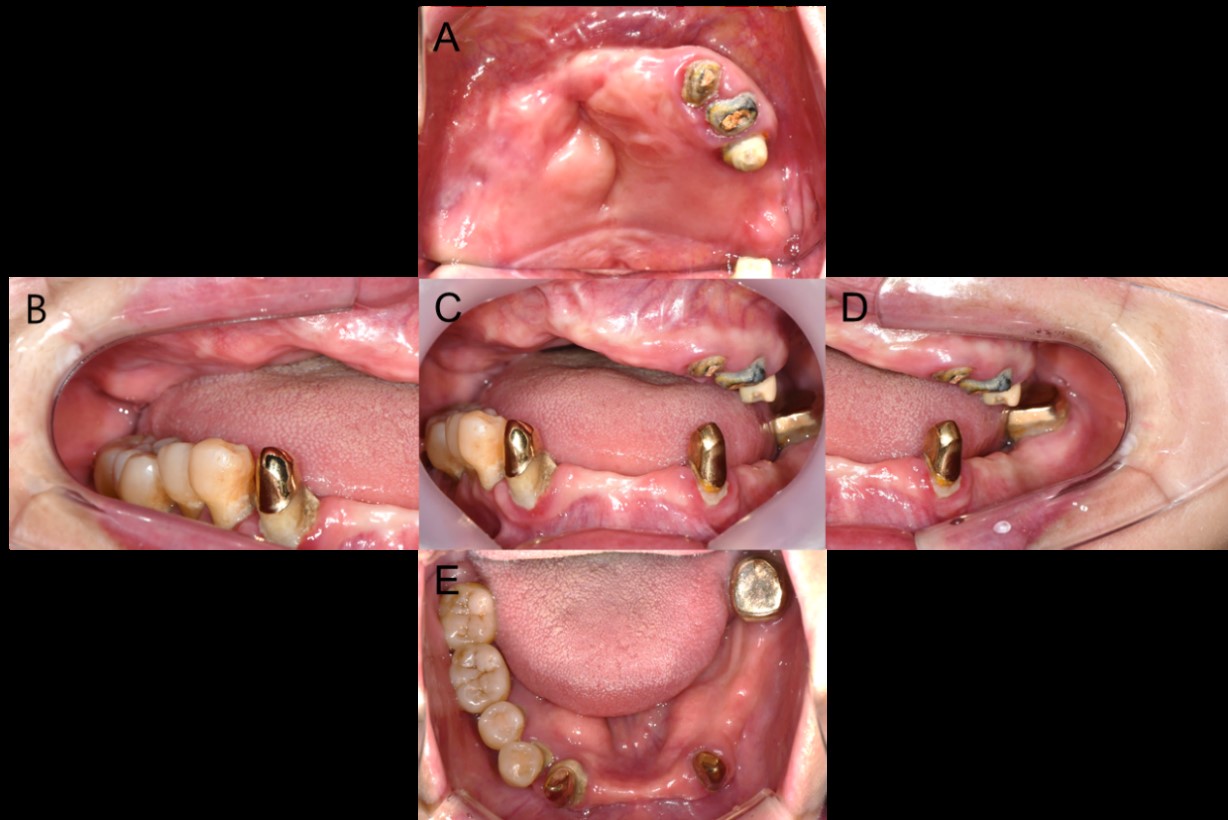
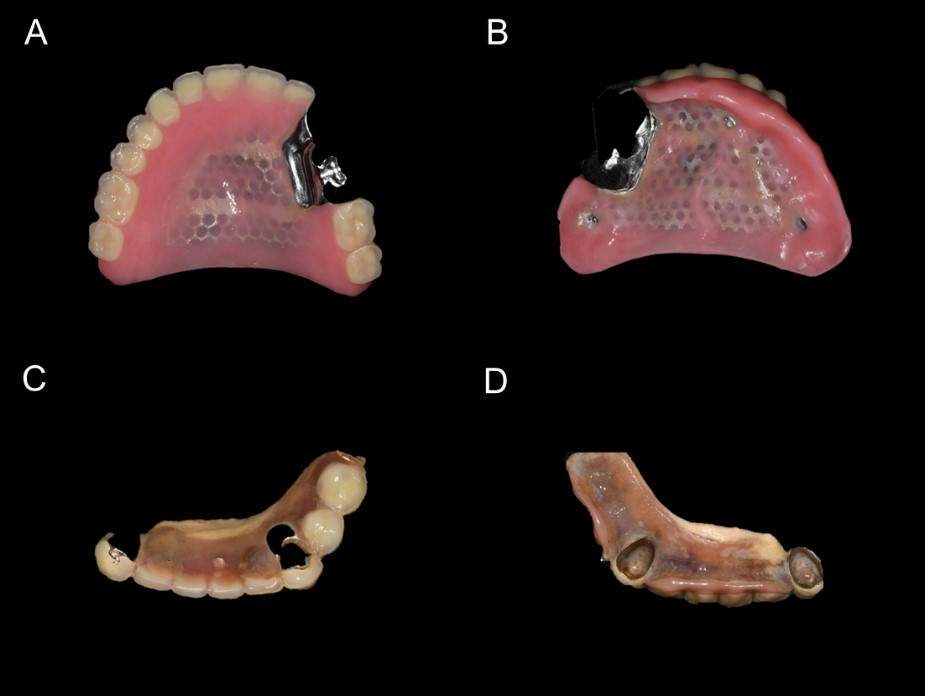
A 53-year-old woman requested new dentures because of a fracture of the teeth supporting her existing prosthesis. Medical history revealed no significant systemic issues, except for a history of cleft lip and palate surgery performed approximately 100 days after birth. Radiographically, generalized alveolar bone resorption was observed in the maxilla, and the remaining teeth #25, 26, and 27 had been prepared for a bridge that had been lost. In the mandible, an apical lesion was observed in tooth #33 and moderate periodontitis was noted (Fig. 1). Clinical examination revealed severe vertical and horizontal bone loss in the anterior regions of the maxilla and mandible, and several teeth were mobile. The existing maxillary denture showed signs of artificial tooth wear, whereas the mandibular partial denture was contaminated and discolored due to inadequate oral hygiene maintenance (Fig. 2 and 3).
Extraoral examination revealed a rightward deviation of the nasal tip and philtrum with insufficient labial support (Fig. 4). In the mandible, periodontal disease had resulted in generalized alveolar bone resorption, and a torus is present on the lingual side. The patient had previously used a maxillary RPD and mandibular Konus RPD. However, the maxillary prosthesis, specifically #23, #24, and #25, was lost, and the fit of the mandibular prosthesis was inadequate. Owing to the poor prognosis of the remaining abutment teeth in both arches, we decided to extract them. The patient desired more aesthetically pleasing prostheses than the existing ones and preferred implants to make a stable prosthesis with good retention. Considering the severe bone resorption in the maxilla, presence of a torus in the mandible, and patient's preference to avoid dentures, implant-supported prostheses were planned. However, financial constraints precluded full-arch implant restoration, and conventional complete dentures and implant-supported overdentures were considered unsuitable.

The treatment process was as follows. Initially, the remaining abutment teeth in both the maxilla and mandible were extracted at the oral and maxillofacial surgery department, and a temporary denture was provided. Cone-beam computed tomography (CBCT) performed 3 months after extraction revealed generalized alveolar bone resorption, particularly in the anterior maxillary region, necessitating bone grafting. Four months after bone grafting, a follow-up CBCT scan was performed to evaluate the reconstructed bone volume. Based on this evaluation, guided implant was performed at the following sites: #15, #16, #23, #25, and #26 in the maxilla, and #33, #36, #43, and #46 in the mandible (Fig. 5). After implant placement, the remaining abutment teeth were determined to have a poor prognosis and were extracted.

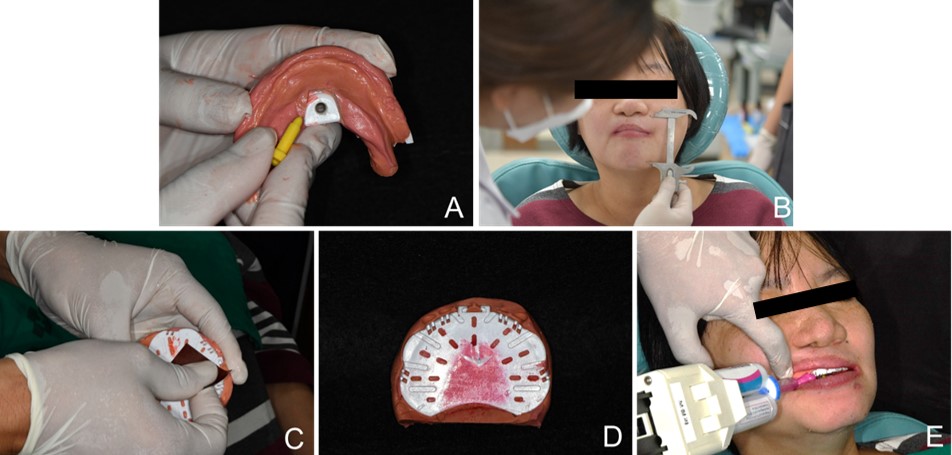
Three months after implant placement, a fixture-level impression was obtained using a custom tray and silicone impression material (Fig. 6). On the same day, the jaw relation was recorded using a JB fork. The process was as follows. First, a tray adhesive was applied to the maxillary plate for stable adhesion of the silicone material (Fig. 7A). Next, six anterior teeth were assembled on the maxillary plate of the JB Fork such that the midline was aligned with the facial midline and the incisal edges were positioned 1 mm below the upper lip. This procedure was performed to identify the location of the maxillary anterior teeth and check their vertical and horizontal positions in the oral cavity (Fig. 7B). Putty impression material (Express STD, 3M, Minnesota, USA) was applied to the plate, and the JB Fork was inserted into the mouth to check the position of the anterior teeth, midline, lip support, and incisal line (Fig. 7C).
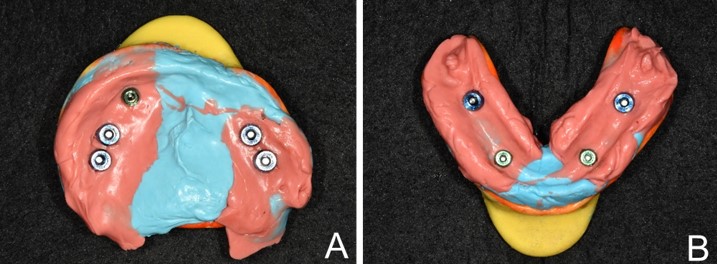

Fig. 7.
Recording the jaw relation using the JB fork. (A) Tray adhesive is applied to the maxillary plate, (B) Six anterior teeth are assembled on the maxillary plate for verifying the vertical and horizontal positions, (C) Putty is applied to the plate, (D) Silicone impression material is added for recording a wash impression.
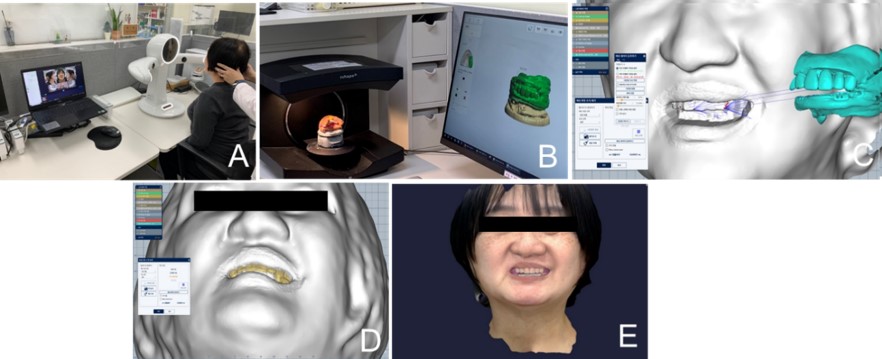
After hardening, the putty was trimmed. A wash impression was made using a silicone impression material (Fig. 7D). This procedure was repeated for the mandibular arch. Because the mandibular tray of JB Fork does not extend to the molars, the putty was pushed past the wing area toward the tongue with fingers. This silicone impression was overlayed on scan data for the master casts obtained from the final impression. A screw was attached to the mandibular plate to determine the patient’s vertical dimensions (Fig. 8A). The recorded vertical dimension matched that of the temporary denture (Fig. 8B). Occlusal paper was applied to the maxillary plate (Fig. 8C) and the maxillary anterior teeth were separated for gothic arch tracing (Fig. 8D). A small hole was prepared for fixation when no significant difference from the habitual tapping point was observed after Gothic arch tracing. Tray adhesive was applied, and the bite was registered using silicone material (Fig. 8E). Extraoral data were obtained using a facial scanner (Ray Co., Ltd., Hwaseong, Korea) with the JB fork in place (Fig. 9A). The bite-registration data obtained using the extraoral scanner were exported to create an STL file (Fig. 9B). The STL file was superimposed on the facial scan and JB fork data and aligned using the six anterior teeth (Fig. 9C and 9D). After combining with the previously scanned master casts, a virtual patient with aligned facial, bite, and oral data was generated (Fig. 9E).
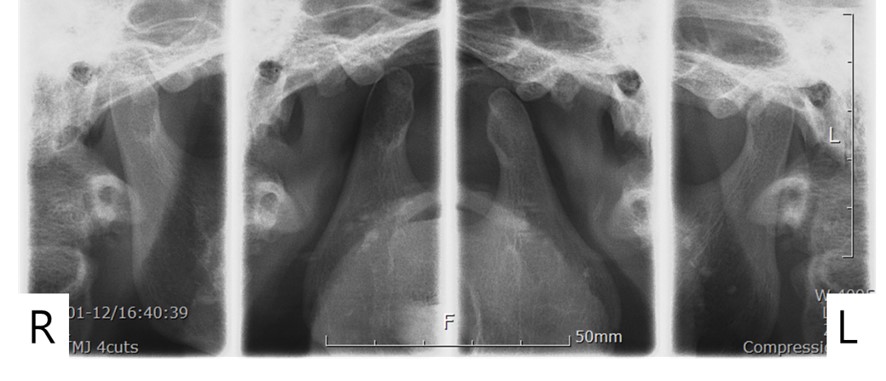
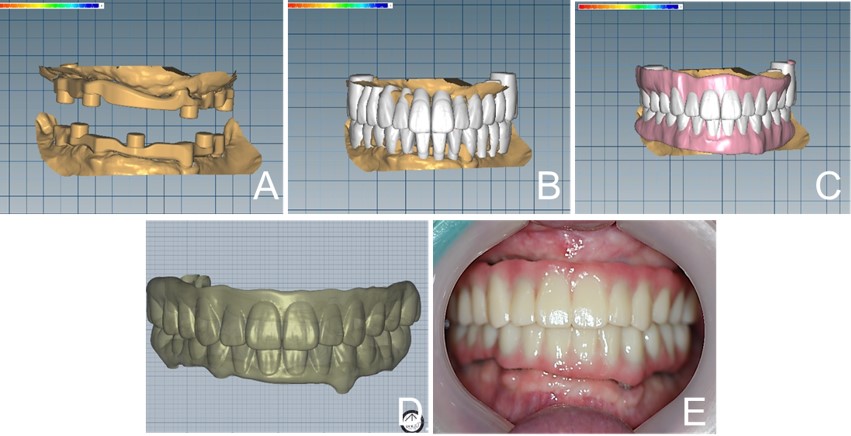
The process for designing the prosthesis on the superimposed CAD data was as follows: To fabricate the bar and zirconia prosthesis, the artificial teeth were arranged, and the bar was designed to match the position of the teeth (Fig. 10A). The tooth arrangement was guided by the Camper’s plane obtained from the facial scan data (Fig. 10B). The scan body was superimposed within the CAD software to verify the position of the implant fixtures, and the direction of bar insertion was determined (Fig. 10C). A minimum space of 2–3 mm was maintained between the bar and the gingiva, and holes were created for connector attachment. Subsequently, the gumline was designed based on the designed bar and tooth arrangement, providing space between the prosthesis and the gingiva on the buccal and palatal sides for ease of oral hygiene (Fig. 10D). A provisional prosthesis was fabricated using polymethyl methacrylate, and the bar was milled from titanium (Fig. 10E). After the bars were placed in both arches, radiographs were obtained to ensure a proper fit before attaching the provisional prosthesis. Owing to potential discrepancies during the superimposition process, the occlusion of the provisional prostheses and aesthetic aspects, such as midline alignment and oral hygiene, were evaluated (Fig. 11). Although the fit of the provisional prosthesis was good, the visibility of the bar buccally through the gingival space was deemed unesthetic. Therefore, additional coverage was provided cervically on the buccal side, and more space was created on the palatal side for oral hygiene. After fitting the provisional prosthesis, a temporomandibular joint (TMJ) radiograph (Fig. 12) was used to check for TMJ abnormalities. The patient was monitored with the provisional prostheses for three months to evaluate occlusal stability, patient satisfaction with facial aesthetics, and ease of oral hygiene. Definitive prostheses were fabricated when the patient reported no discomfort. A Trios 4 intraoral scanner (3Shape, Copenhagen, Denmark) was used to capture the bar and provisional prostheses positions. Corrections were made to the midline and gum designs based on the provisional prostheses, and the definitive prostheses were designed (Fig. 13). An ADD-TOC connector (PNUADD Co., Ltd., Busan, Korea) was attached to the bar with a torque of 35 N·cm, and the definitive prostheses were milled from zirconia blocks. The definitive prostheses were inserted in the mouth, and fit and occlusion were verified. To protect the TMJ, partial group function occlusion was established, and the last molars were discluded. A vent hole was created in the metal housing adhesion area inside the zirconia prosthesis, and the metal housing was fixed using a self-adhesive resin cement (G-cem LinkAce; GC Corporation, Tokyo, Japan). After insertion of the definitive prosthesis, extraoral photographs (Fig. 14) revealed enhanced labial support and correction of commissural sagging resulting from the reduced vertical dimension. The patient was educated regarding oral hygiene practices. Six months after prostheses insertion, the patient reported satisfaction with the aesthetics and function. Regular follow-ups to monitor the implants and prostheses are ongoing.
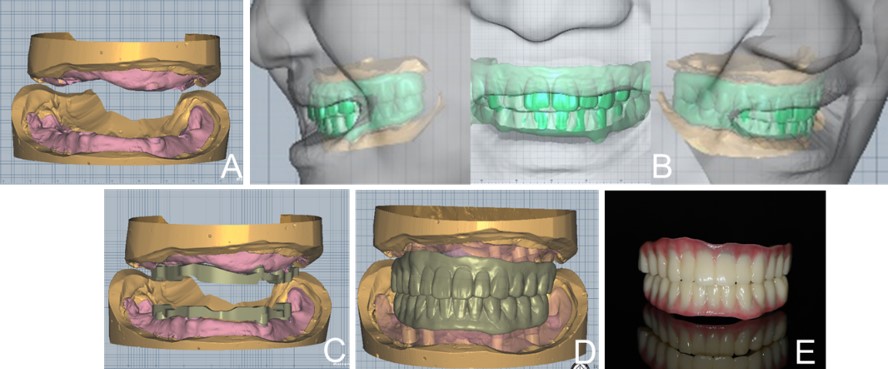
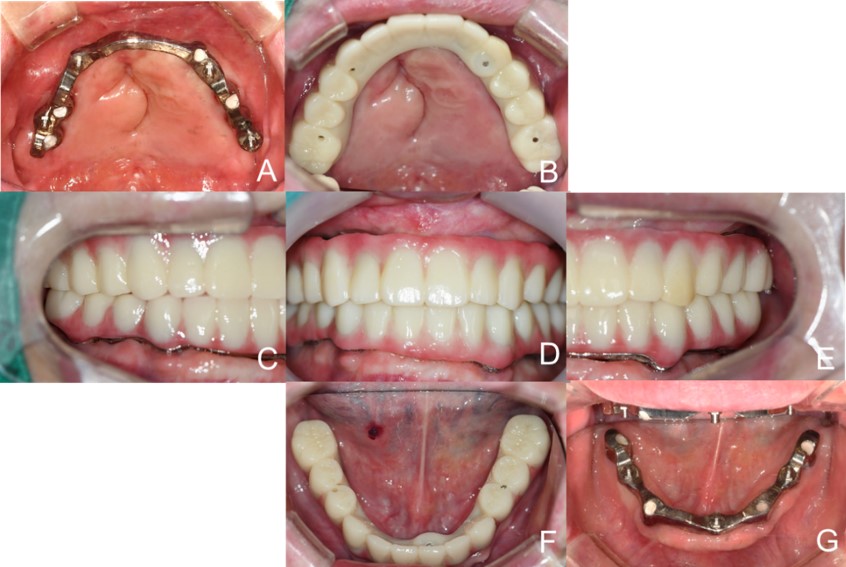
Fig. 11.
Intraoral photographs after provisional prostheses delivery. (A) Occlusal view of the maxilla with the milled bar, (B) Occlusal view of the maxilla with the provisional prosthesis, (C) Left lateral view, (D) Frontal view, (E) Right lateral view, (F) Occlusal view of the mandible with the provisional prosthesis, (G) Occlusal view of the mandible with the milled bar.

Ⅲ. Discussion
This patient experienced a reduction in the retention of existing restorations owing to the loss of previous prostheses and mobility of the remaining abutment teeth. Owing to a history of cleft lip and palate surgery, the patient had inadequate residual bone in the maxilla, and chronic periodontitis caused mobility in all remaining abutment teeth in the mandible. In patients with moderate to severe bone resorption, maintaining oral hygiene becomes challenging with fixed implant prostheses, and the risks of unesthetic prostheses and prosthesis and screw fractures are higher. According to Bulaqi et al.10 increased prosthesis length is correlated with a higher incidence of screw loosening and increased stress in the bone surrounding the implant. Zitzmann et al.11 reported that in patients with increased vertical implant-crown space, an implant-supported overdenture is often easier to manage and maintain than a fixed prosthesis. This patient had >15 mm of space above the gingival margins. Therefore, a conventional denture or milled bar would allow better maintenance of oral hygiene and be more aesthetically pleasing than a fixed prosthesis. However, owing to the patient's relatively young age and preference for avoiding denture-type prostheses, a hybrid prosthesis, that was fixed in the mouth but could be removed if necessary, was chosen. Furthermore, because of the significant aesthetic demands of the patient, zirconia, which offers excellent shade reproduction,12 was selected. Moreover, zirconia provides greater resistance to wear and discoloration compared to acrylic resin,13 resulting in better durability and hygiene. Therefore, zirconia–bar prostheses were used in this study. The prostheses were designed to minimize bar exposure above the gingival margin, while providing sufficient space on the palatal side to facilitate oral hygiene.
The conventional method using occlusal rims can be used to obtain jaw relations, including the vertical dimension, centric relation, midline, incisor teeth position, and occlusal plane. However, this method requires multiple patient visits, and additional time is required for occlusal rim fabrication and adjustment. The JB fork used in this study offers the advantage of simultaneously recording impressions and jaw relation, which streamlines the process. Additionally, the data obtained from articular registration can be superimposed with intraoral and facial scan data, allowing easy conversion into CAD data for the arrangement of artificial teeth and prosthesis design. This system involves creating a putty template on the plate and obtaining information for overlay with the silicone impression. Using a screw in the mandibular tray allows the determination of the vertical dimension, and Gothic arch tracing simplifies the process of recording jaw relations. The key difference between the JB fork system and previous CAD-CAM denture systems is the ability to determine the vertical and horizontal positions of the maxillary anterior teeth by assembling six anterior teeth on the maxillary plate. This approach allows for precise alignment of the anterior teeth and enables the use of these teeth as reference points for superimposing facial data with occlusal registration data obtained using the JB fork. This unique feature enhances the accuracy and efficiency of integrating occlusal and facial data into prosthetic design. However, because of the possibility of bite errors, it is necessary to check the midline, occlusal plane, and jaw relation in the provisional prosthesis and incorporate the necessary changes in the definitive prosthesis. Additionally, a modified provisional prosthesis can be applied to patients to assess its fit.
Ⅳ. Conclusion
The use of a milled bar combined with ADD-TOC attachments for removable zirconia prostheses resulted in good functional and aesthetic outcomes in a patient with severe bone resorption. Additionally, using the JB fork for recording the jaw relation reduced the number of patient visits and streamlined the process by allowing direct integration with CAD software, making it a more convenient treatment method than the conventional method using occlusal rims.
