

Ⅰ. Introduction
Implant overdentures have a better long-term prognosis than complete dentures and a high success rate in the mandible.1,2,3 Compared to clasp-retained removable partial dentures, implant overdentures have advantages in maintenance and stability and are less affected by the positions of the placed implants.4,5 Implant overdentures are generally divided into solitary and bar types, according to attachment. The solitary attachments include the ball, cap, magnet, and double crown types.6 In the double crown method, a friction pin structure can be added as an additional attachment using the spark erosion technique.7 The friction pin gives a retentive force, allowing a passive fit between the inner and outer telescopic crowns. The friction pin can be activated when a decrease in retention of the overdenture is found during the maintenance period.
This case report describes the prosthetic treatment of an implant-supported double-crown-retained removable denture in a case of failure of an implant-supported fixed dental prosthesis (FDP) due to medication-related osteonecrosis of the jaw (MRONJ).
Ⅱ. Case Report
A 78-year-old female patient presented with gingival swelling and pain in the anterior arch. The patient mentioned that the implant-supported FDP was set up approximately 15 years ago in a local dental clinic (Figs. 1 and 2).

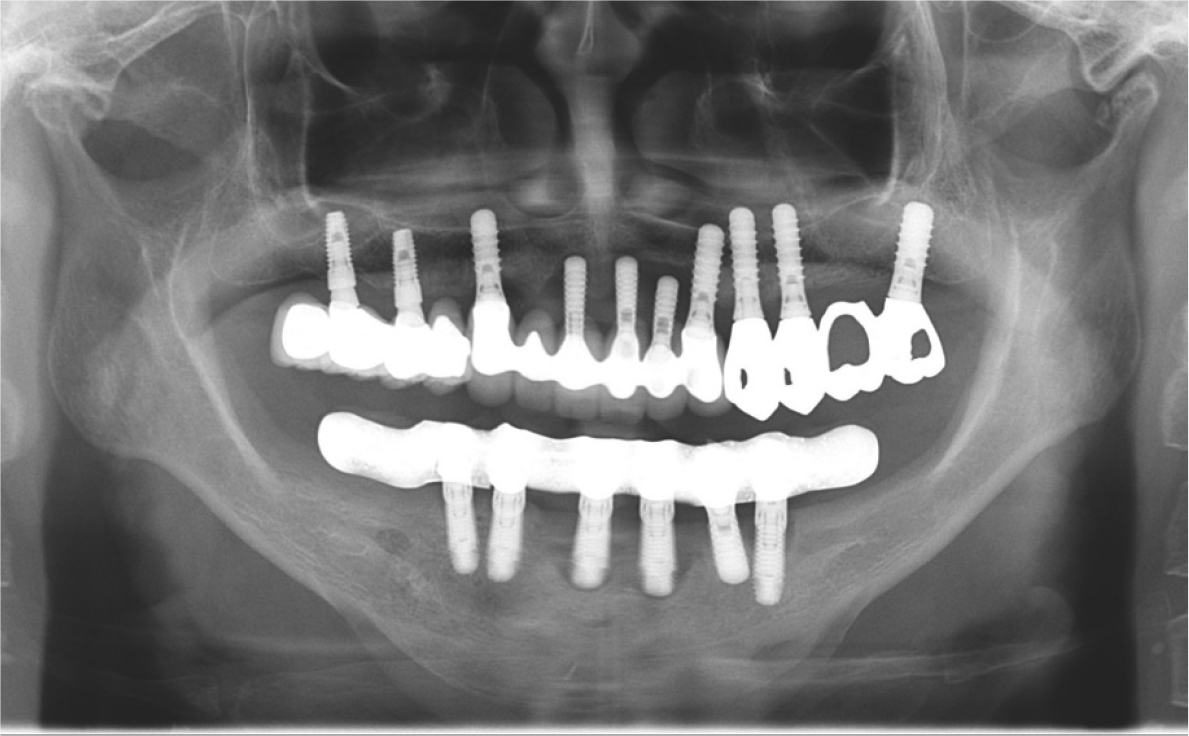
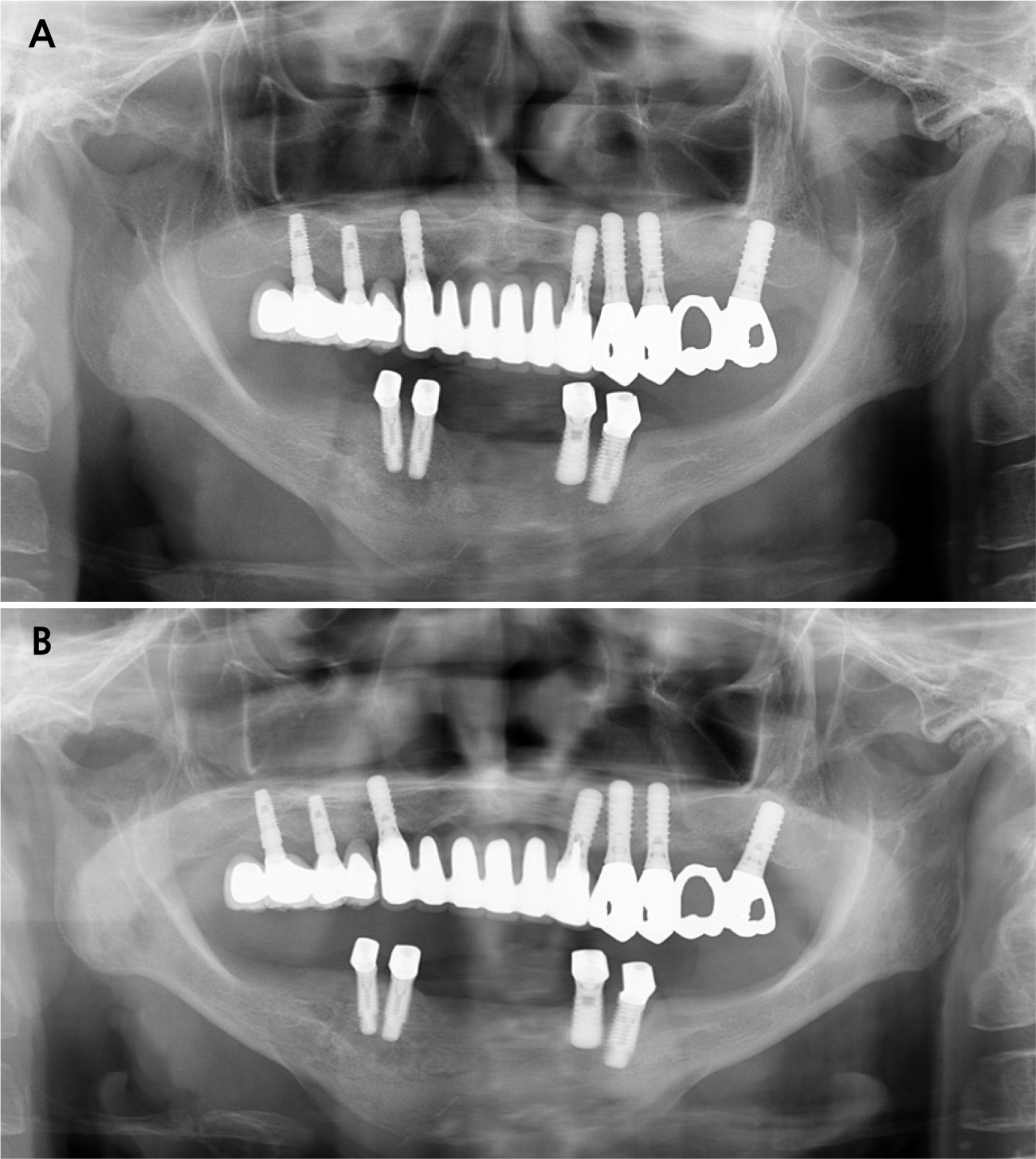
Clinical and radiographic examinations revealed bone resorption and inflammation around the implants in the maxilla and mandible, and the implant threads were exposed in the oral cavity (Fig. 3). The implants in #11, 21, 22, 31, and 41 areas (Brånemark System Mk II TiUnite; Nobel Biocare AB, Göteborg, Sweden) were diagnosed as failing because of osteomyelitis caused by MRONJ. The patient had been receiving alendronate-based drugs for osteoporosis since 2015. Meanwhile, no critical biological concern was found in other implants, except for mild peri-implantitis. The treatment modalities were explained to the patient, and implant-supported double-crown-retained removable dentures were chosen for the mandible.
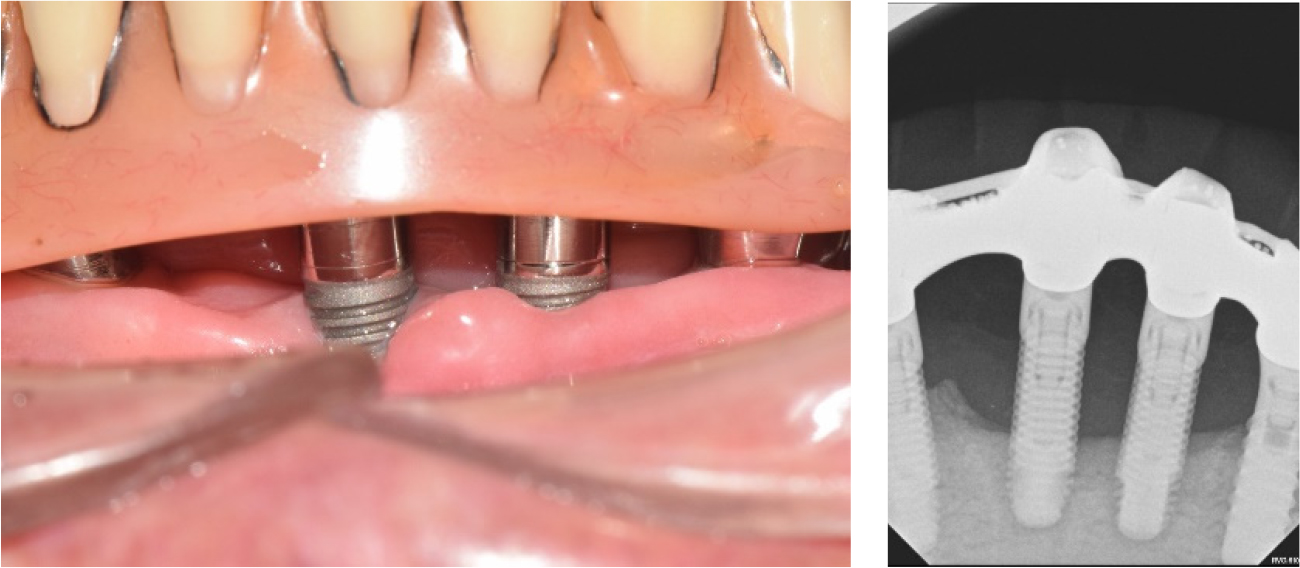
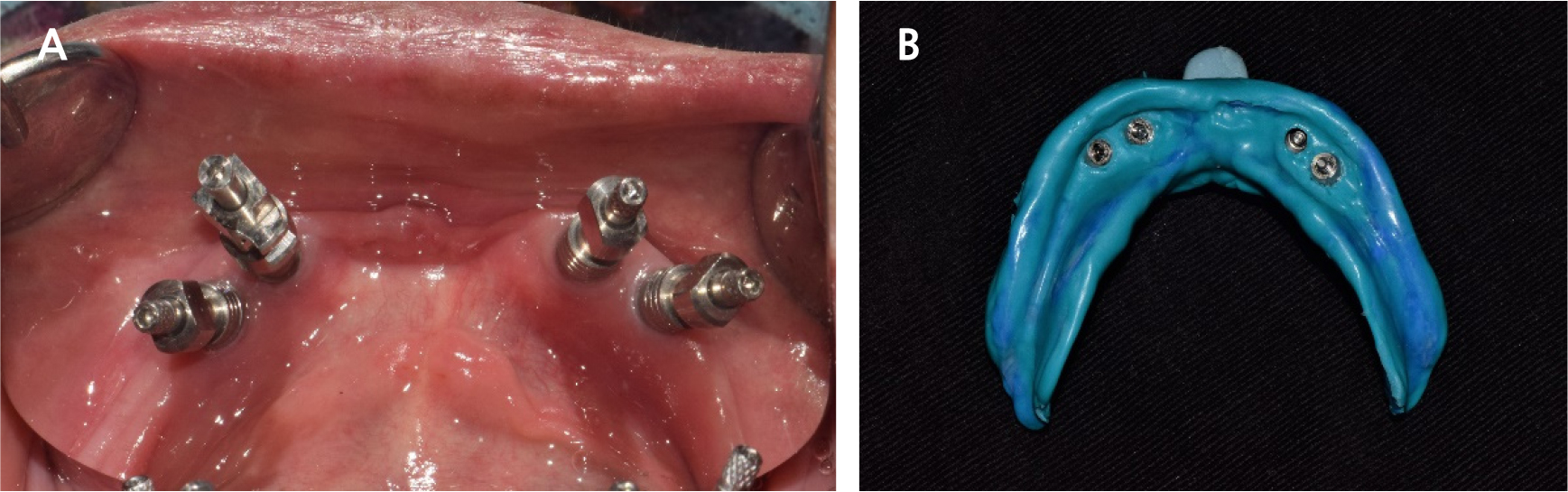
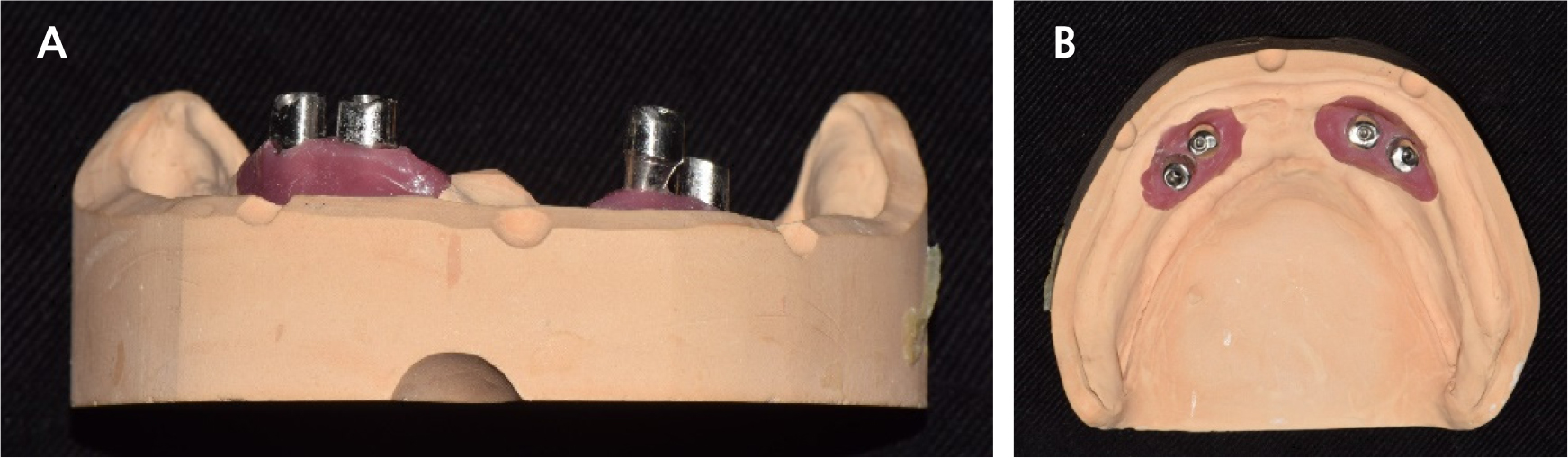
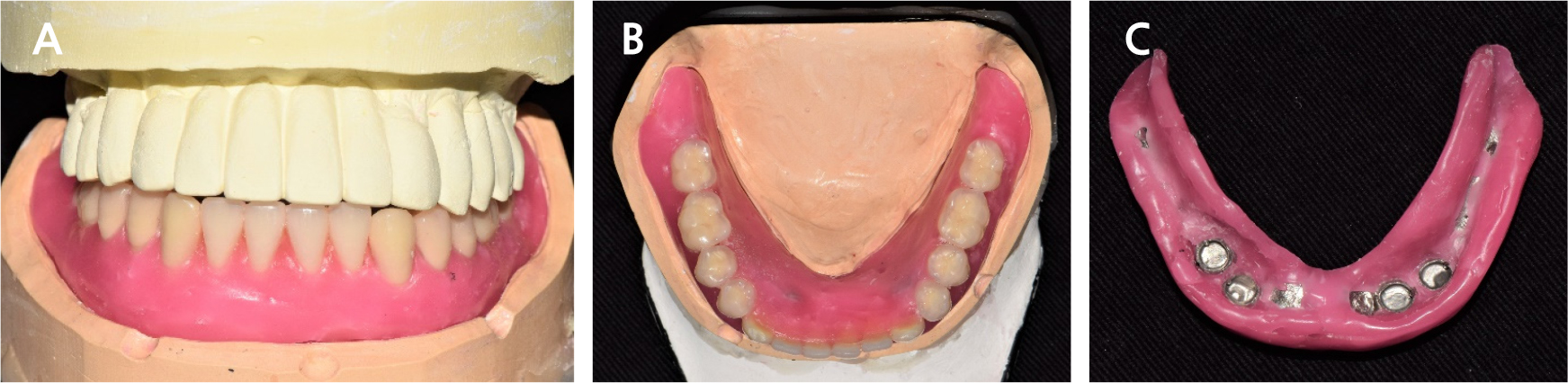
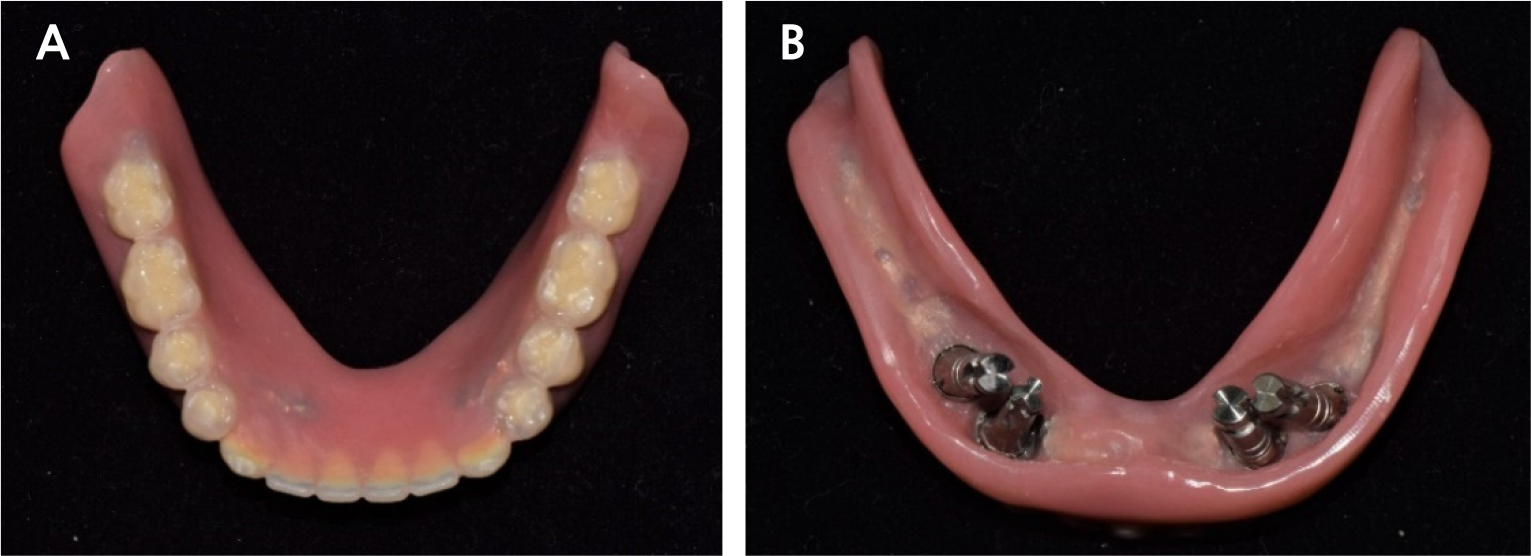
The FDP in the anterior area of the maxilla and the full-arch FDP in the mandible were removed, and the hopeless implants were removed under local anesthesia. After three months of healing (Fig. 4), when the gingiva and underlying bone stabilized, prosthetic treatment commenced. a six-unit metal ceramic FDP was fabricated in the maxilla using conventional silicone impression and casting procedures. In the mandible, pick-up impression taking was performed for the four remaining implants using an individual tray and silicone materials (Aquasil Ultra LV; Dentsply Sinora, Philadelphia, PA, USA) (Fig. 5). Inner crowns with a 2° convergence angle and a chamfer margin were fabricated for the four implant fixtures with Co-Cr alloy (VeraBond 2V; Aalbadent, Fairfield, CT, USA) (Fig. 6). The corresponding outer crowns were fabricated and attached to the metal framework of the denture using a laser welding technique. Afterwards, fabric pins with the diameter of 0.8 mm were placed on the outer crowns using the spark erosion technique. The vertical dimension of the occlusion was established considering esthetics and function. Artificial teeth (Endura; Shofu, Kyoto, Japan) were arranged using the group function concept and a wax denture was created (Fig. 7). After confirming the wax denture in the oral cavity, a definitive prosthesis was fabricated using flasking, wax wash, and resin packing procedures (Fig. 8).

Periodic recall checks were done every three months after the delivery of the definitive prosthesis. During the three year follow-up period, no periodontal or prosthetic complications were observed (Fig. 9). The patient was satisfied with the ease of hygienic care for the definitive prosthesis, and the implants were well maintained.
Ⅲ. Discussion
The survival and failure of implants are determined by various factors, such as periodical conditions, opposing dentition, stress distribution, oral hygiene, and medical conditions. According to Tallarico’s study, the survival rate of the implant reached 95.0%.8 Despite the high survival rate, medically compromised conditions and oral hygiene factors can aggravate implant stability. In this case, the implants should be removed because of osteomyelitis around the implants due to MRONJ. Thus, the previous implant-supported FDPs were removed and replaced with a double-crown removal denture using the remaining implants. The new denture maintained its position for three years, and MRONJ did not progress further or relapse. The patient also adapted well to the replaced prosthesis.
When a few implants remain in the arch, fixed prostheses or overdentures can be considered.8 Overdentures are preferred in cases where the implant position is not favorable and the implant axes are not parallel to each other. In particular, in patients with MRONJ, prostheses must be detachable, repairable, and easy to clean. Verma et al. reported that implant overdentures have a high success rate in the mandible and a good long-term prognosis.1,2,3 Various attachments can be used in implant overdentures, such as ball, bar, locator, and double crown types. Krenmair et al. examined a high success rate and survival rate by comparing ball and telescopic attachments and reported no significant differences between the attachment systems over five years.9 In addition, Duohong Zou et al. compared bar and telescopic attachments and reported that dental plaque and calculi were observed more frequently in the bar group, even though both treatment methods were effective during periodic recall checks.10,11,12 Thus, in the present case, a solitary type attachment system was considered to facilitate oral hygiene care. Moreover, considering the possible loss of the remaining implants due to MRONJ, a bar attachment system was not recommended because of the repair difficulty. Among the solitary attachment systems, the double crown system was selected because the four remaining implants were not parallel for use in the locator system.
During the follow-up period of three years, the patient was satisfied with the function and maintenance of the new prostheses, and MRONJ did not progress further, and no prosthetic complications were noted. The focus of implant-supported double-crown removable dentures is to check whether excessive lateral force is applied to the implant in use. To minimize possible complications, it is important to examine the fit of the denture to the underlying gingiva. Additionally, thorough oral hygiene care should be provided.
Ⅳ. Conclusion
An implant-supported double-crown-retained removable denture provides a treatment modality for patients who experience implant failure due to medication-related osteonecrosis of the jaw. Double-crown-retained removable dentures are recommended when the remaining implant axes are not favorable and thorough oral hygiene care is needed.
