

Ⅰ. Introduction
Implant treatment in the maxillary anterior region is challenging. It is often required in young patients with facial trauma or congenital defects and in older patients with alveolar bone resorption due to chronic periodontal disease or a long-term edentulous state after tooth extraction. Prosthetic treatment options for partially edentulous anterior areas can be classified according to the need for bone grafting. If bone graft is not feasible, limited treatment options are available, such as a conventional bridge using a pink porcelain or a removable partial denture which can cover the alveolar defect.1,2 The most suitable treatment modality for aesthetic and functional satisfaction in adult patients with maxillary anterior defects is implant- supported fixed partial dentures (FPDs).3 However, horizontal or vertical bone augmentation is essential prior to implant placement, because insufficient bone is available in the maxillary anterior region.
The horizontal bone augmentation technique is divided into three categories: particulate or block-bone grafts with collagenous membranes, ridge splits or expansions, and distraction osteogenesis.4, 5, 6According to Fu et al., the three-dimensional buccolingual bone width available at the implant placement site is a key factor in the selection of augmentation techniques. Ridge split or expansion is possible in residual ridges with widths of 4–5 mm. In ridges with width ≥3.5 mm, simultaneous implant placement with bone graft or staged implant placement after guided bone regeneration, is planned depending on the expected primary implant stability. In case of residual ridge width <3.5 mm, primary implant stability cannot be achieved, and onlay bone grafting using a block-type bone is recommended.7
Autogenous block-bone grafts are the standard onlay grafts used to reconstruct horizontal ridge deficiencies. However, an intraoral/extraoral donor site is required for autografts, which is associated with problems such as paresthesia, increased costs, or discomfort in daily life.8Owing to these limitations, interest in allogeneic block-bones that are relatively less traumatic and safe has increased. Processing at the tissue bank and during surgery; selecting a block with both cortical and cancellous bone, shaping the block to fit the defect, and immobilizing the block contribute to favorable bone volume outcomes with allogeneic bone grafts.9Previous studies on the use of an allogeneic block-bone and collagen membrane with a follow-up period ≥12 months have reported success rates of 99%, 95.3–100%, and 100%.10, 11, 12, 13 Thus, it is a predictable clinical technique. Resorption of allogeneic bone blocks at the time of implant insertion is significantly lower (10–14%) than that of autogenous blocks.14
Herein, we report the use of allogeneic block-bone grafts for single- and multiple-tooth defects with severely atrophic alveolar ridges in the maxillary anterior region.
Ⅱ. Case Report
1. Case 1
A 21-year-old healthy, nonsmoker woman reported to the Department of Prosthodontics at Gangnam Severance Dental Hospital to request an aesthetic anterior prosthesis to replace the old crown of her upper left central incisor. Clinical examination revealed periodontal pockets up to the apical third and moderate-to-severe mobility (Fig. 1A, 1B). Radiographic examination revealed root resorption of the incisor and severe resorption of the surrounding bone (Fig. 1C). Cone-beam computed tomography (CBCT) was performed to measure the bone volume and plan the bone graft owing to vertical and horizontal bone loss (Fig. 1D). Since the patient was young, interested in an aesthetic smile, and did not want any invasive treatment at other sites, implant placement with an allogeneic block-bone graft was planned. Patient consent was obtained for all procedures.
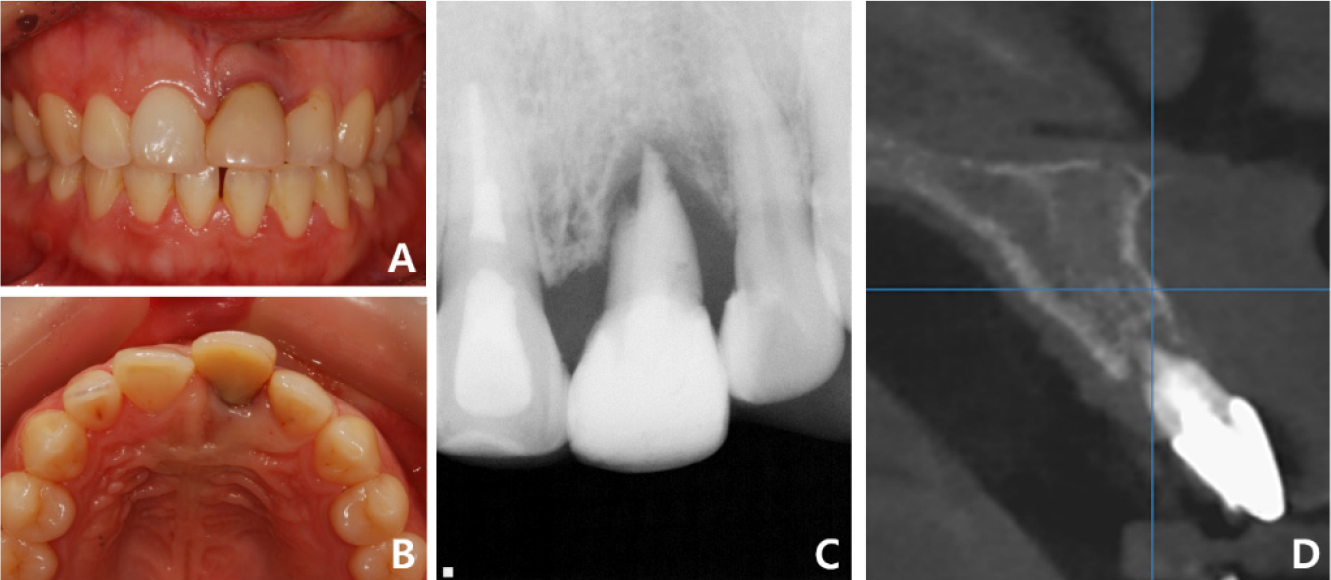
Fig. 1.
Case 1: Intraoral and radiographic views at the patient’s first visit. (A) Periodontal disease is observed in tooth #21, (B) Pathologic migration of tooth #21 toward the labial side, (C) Periapical radiograph shows external root resorption in tooth #21, (D) Sagittal cone-beam computed tomography image shows alveolar bone resorption around tooth #21.
First, the left central incisor was extracted, and the crown portion of the tooth was bonded to the adjacent teeth as a provisional restoration. After a healing period of three months, ridge augmentation was performed using allogeneic bone blocks (Fig. 2). Under local anesthesia, a typical full-thickness mid-crestal incision was made and two divergent vertical incisions were made one tooth away from the surgical site on either side. A periodontal flap was elevated, and a periosteal-releasing incision for the augmented bone volume was made in the labial flap. The allogeneic block-bone (Tricortical Block 10 × 10 × 10 mm; Hansol Medical, Seoul, Korea) was trimmed to fit the alveolar defect and fixed using two microscrews. A double-layer collagen membrane (Bio-Gide®; Geistlich Biomaterials, Wolhusen, Switzerland) was applied over the graft, and the flap was sutured using non-absorbable nylon (Fig. 3). Gentle compression was applied for several minutes to promote primary fixation and hemostasis, and the patient was instructed to take postoperative precautions and medications.
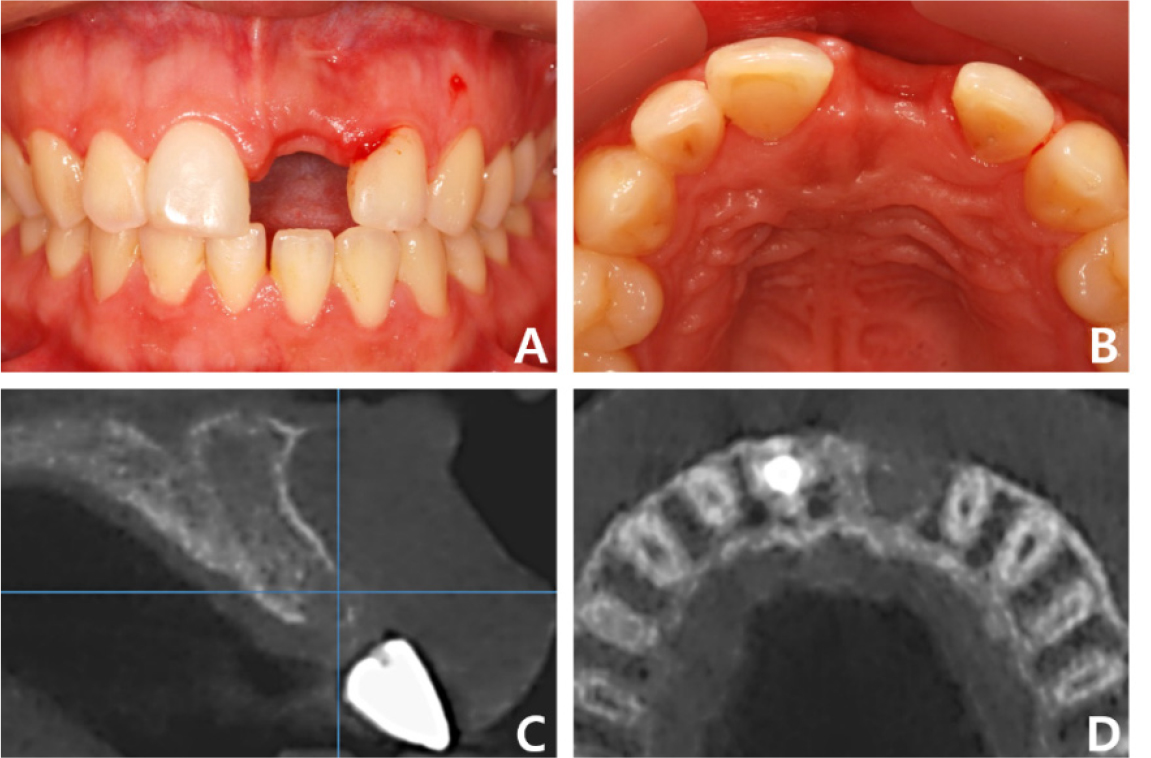
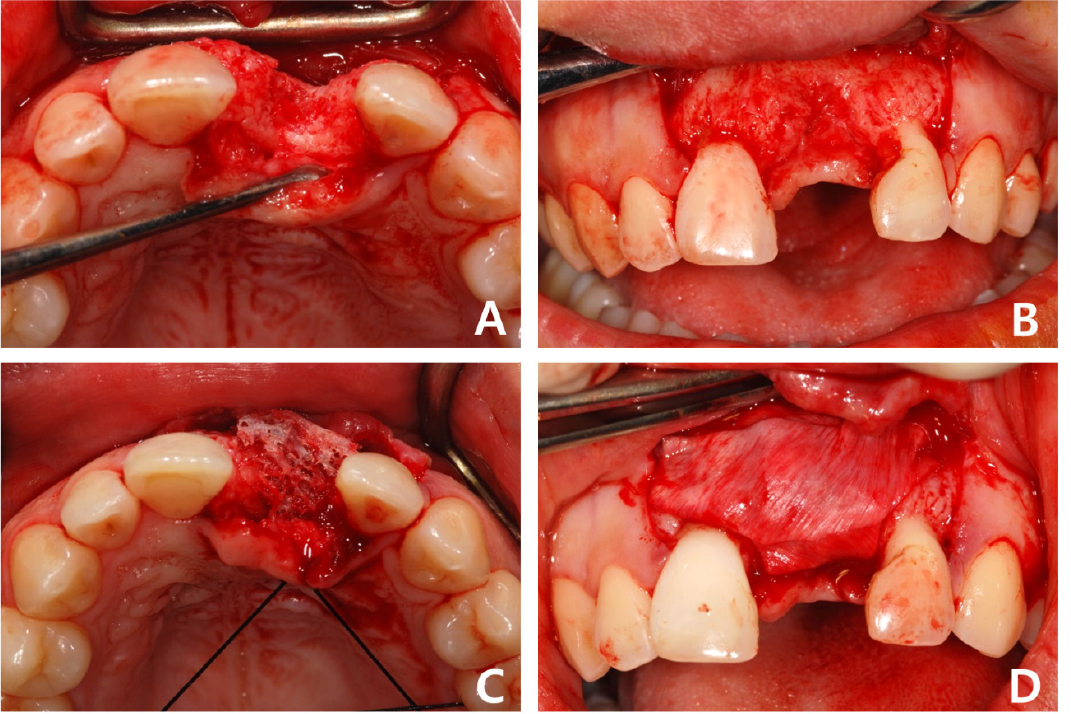
Fig. 3.
Case 1: Intraoral photos of allogeneic block-bone graft surgery. (A) Occlusal view before grafting, (B) Frontal view before grafting, (C) Allogeneic bone block has been grafted on the labial side in the #21 region, (D) A collagen membrane has been applied over the bone block for separation from the soft tissue.
Regular follow-up was performed during the bone remodeling phase of approximately four months, and the stability of the graft was confirmed using CBCT (Fig. 4A). The fixation microscrews were removed, and an implant was placed at the graft site (Fig. 4B). A bone-level implant (IU; Warantec, Seongnam, Korea) with a tapered body, diameter of 4.0 mm, and length of 10.0 mm was used (Fig. 4C). The initial fixation torque was 25 Ncm, and a healing abutment was connected to the implant (Fig. 4D). Three months after implant placement, provisional restoration was performed with soft tissue alterations. The final prosthesis was fabricated and the patient was satisfied with the new central incisor (Fig. 4E). At the 4-year follow-up, CBCT revealed a decrease in the grafted bone volume; however, the final implant prosthesis was intact (Fig. 4F).
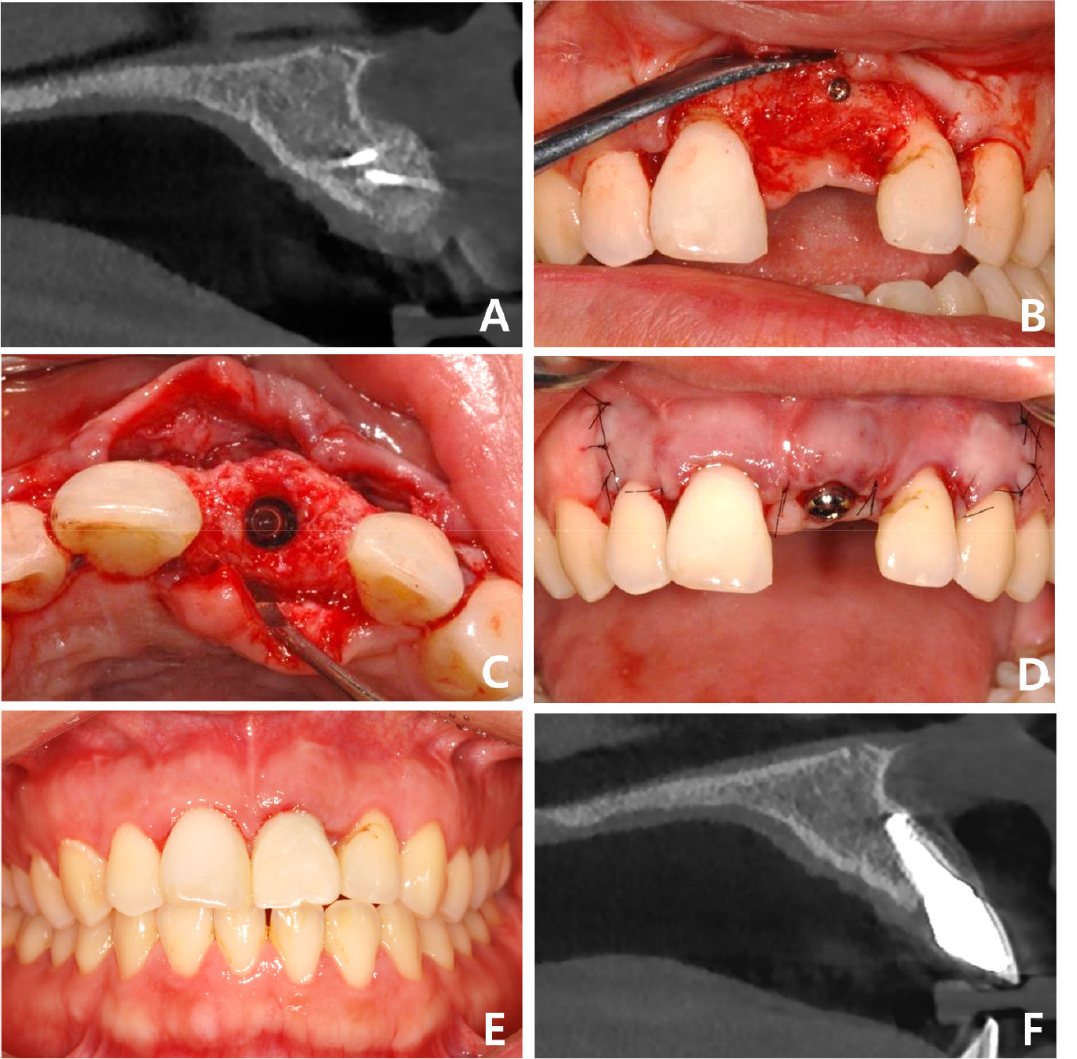
Fig. 4.
Case 1: Intraoral and radiographic views related to implant placement and final prosthesis at the grafted site. (A) Sagittal CBCT image of the grafted site before implantation, (B) Frontal view after flap elevation for implantation, (C) Occlusal view of augmented site after implantation, (D) Frontal view after healing abutment connection, (E) Frontal view after final prosthesis delivery, (F) Sagittal CBCT image of the implant prosthesis at the four-year follow-up. CBCT, cone-beam computed tomography.
2. Case 2
A 63-year-old woman who was on medication for hyperlipidemia visited the Department of Prosthodontics at Gangnam Severance Dental Hospital because she wanted to change old bridges due to porcelain fractures. Clinical and radiographic examinations revealed secondary dental caries in the maxillary left first premolar under an anterior 7-unit FPD (Fig. 5). Because it was necessary to extract a terminal abutment tooth, implant placement at sites #23 and #25 was planned for the rehabilitation of the left lateral incisor, canine, and premolars. A 4-unit implant-supported FPD with a #22 mesial cantilever was planned, and the patient agreed to the treatment plan of implant-supported FPD for improved aesthetics and function.
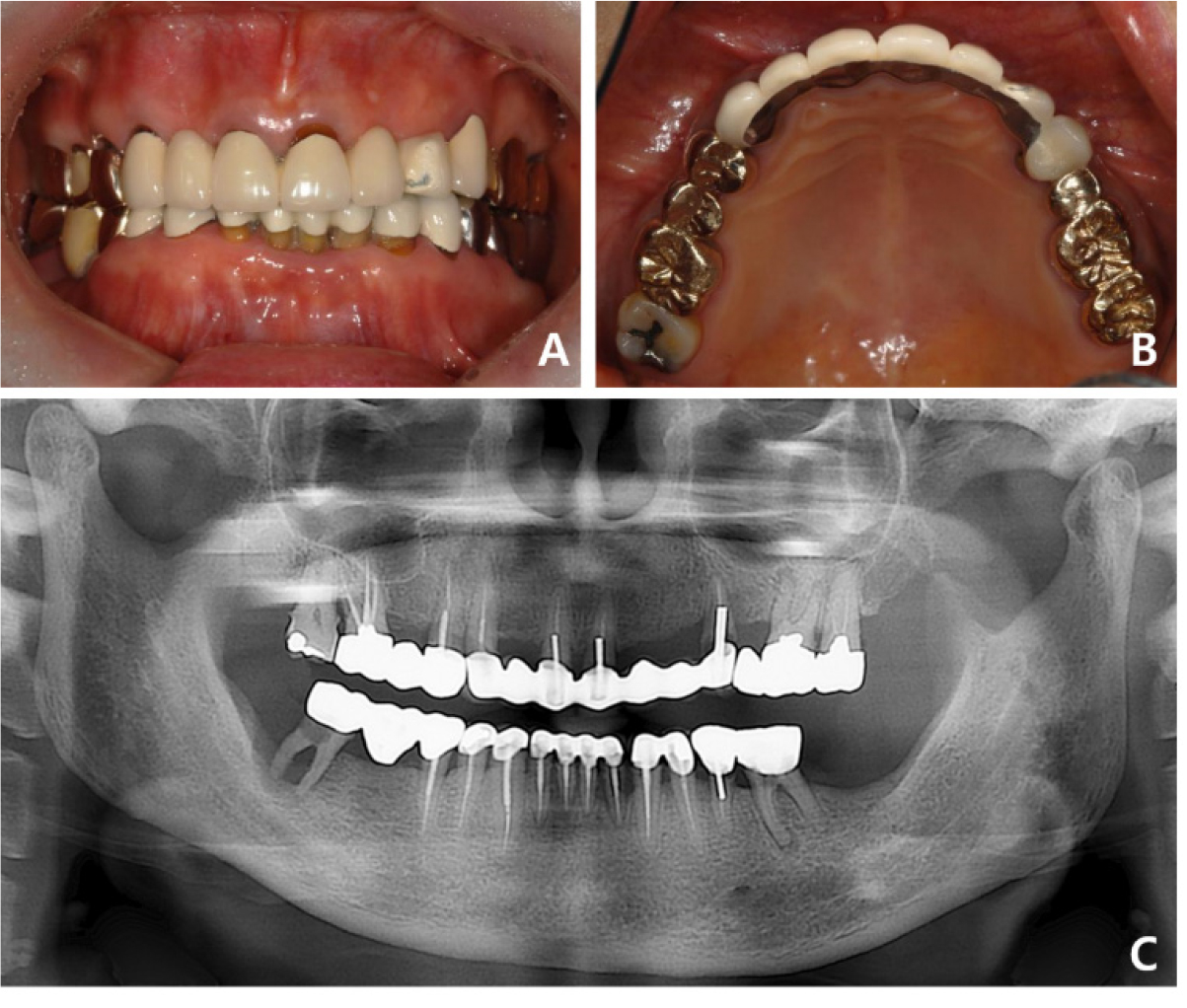
Fig. 5.
Case 2: Intraoral and radiographic views at the patient’s first visit. (A) A porcelain fracture is observed on the labial side of tooth #23 of the maxillary anterior ceramic prosthesis, (B) Seven-unit splinted maxillary anterior prosthesis from tooth #13 to tooth #24, (C) Panoramic radiograph suggests secondary caries in the abutment tooth #24.
The alveolar bone bed was evaluated for implant placement after removal of the old prostheses. In particular, the left side of the anterior maxillary ridge was severely atrophic due to the long-term edentulous state after tooth extraction. CT showed sufficient bone height; however, the bone width was approximately 3 mm, indicating a narrow and thin alveolar ridge. Because the patient was old, bone graft using allogeneic, rather than autogenous, block-bone was considered to minimize damage. An incision was made in the left maxillary surgical site under local anesthesia. After a full thickness of periodontal flap was elevated, an allogeneic block-bone (Tricortical Block 20×40 mm; Hansol Medical) was adjusted into a ‘J’ shape and fixed to the alveolar bone using two micro screws (Fig. 6). The cancellous surface of the block-bone was attached to the alveolar bone and the cortical surface to the soft tissue. Additionally, a particulate bovine bone graft (Bio-Oss®; Geistlich Biomaterials) was placed around the grafted block-bone using a collagen membrane (Bio-Gide®; Geistlich Biomaterials), and the wound was sutured without tension. Six months after grafting, two implants with length 10.0 mm and diameter 4.0 and 4.5 mm (IU; Warantec) were placed in the #23 and #25 regions, respectively (Fig. 7).
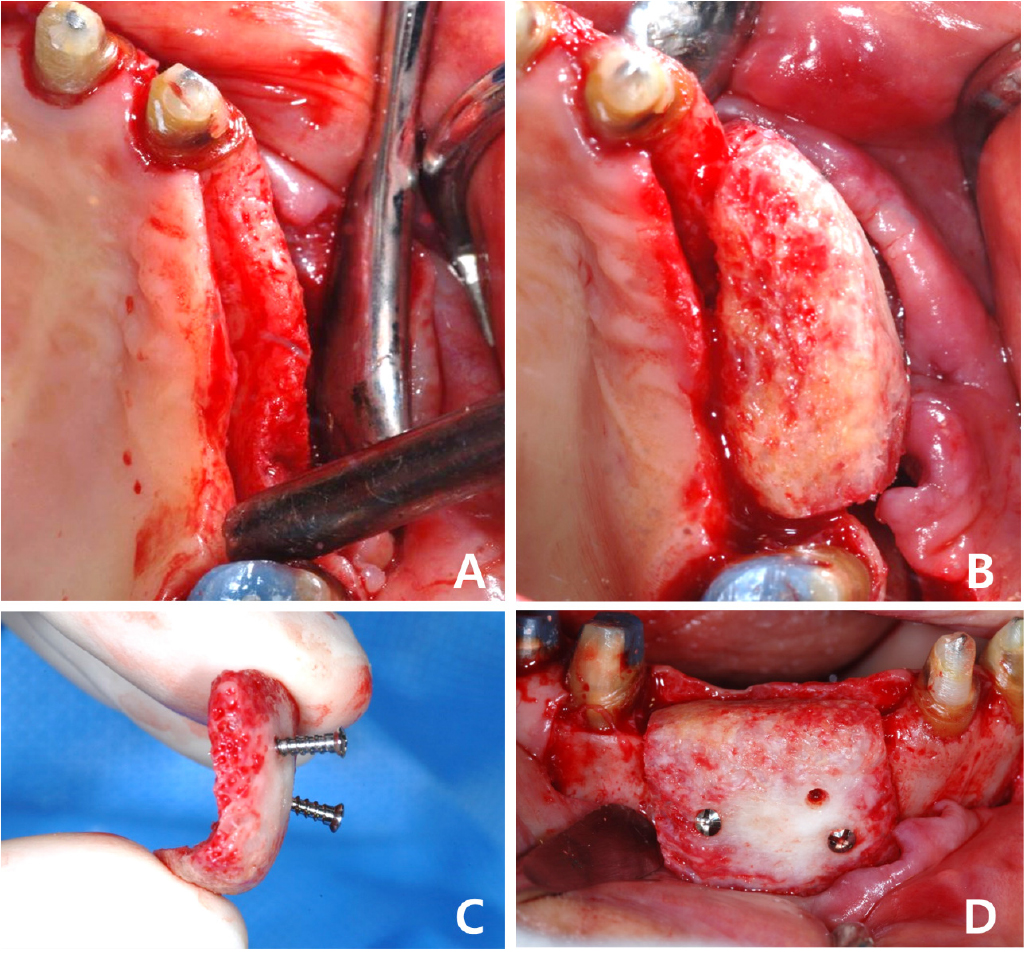
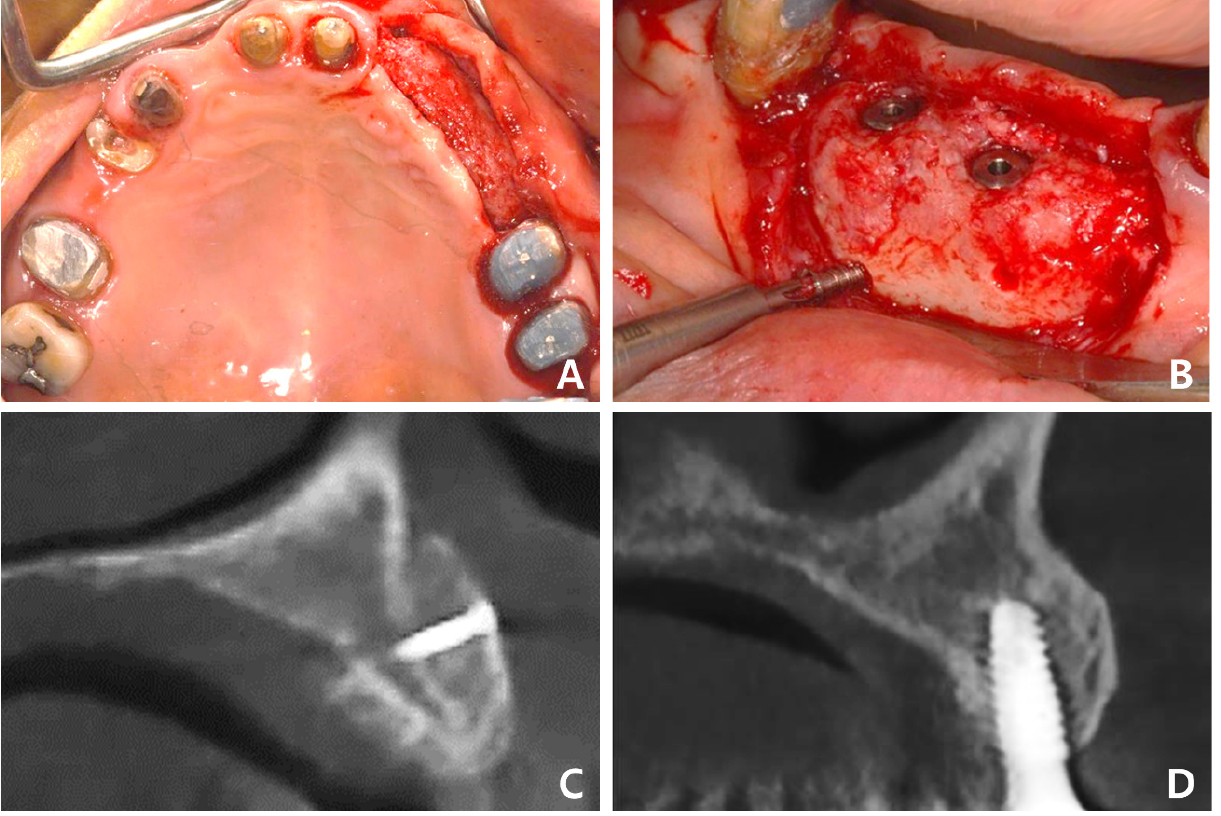
Fig. 7.
Case 2: Intraoral and radiographic views of grafted site. (A) Sufficient bone bed for implantation is observed after block-bone grafting, (B) Two implants have been placed and submerged at the grafted site, (C) Sagittal CBCT image of the grafted site before implantation, (D) Sagittal CBCT image of the grafted site after implantation. CBCT, cone-beam computed tomography.
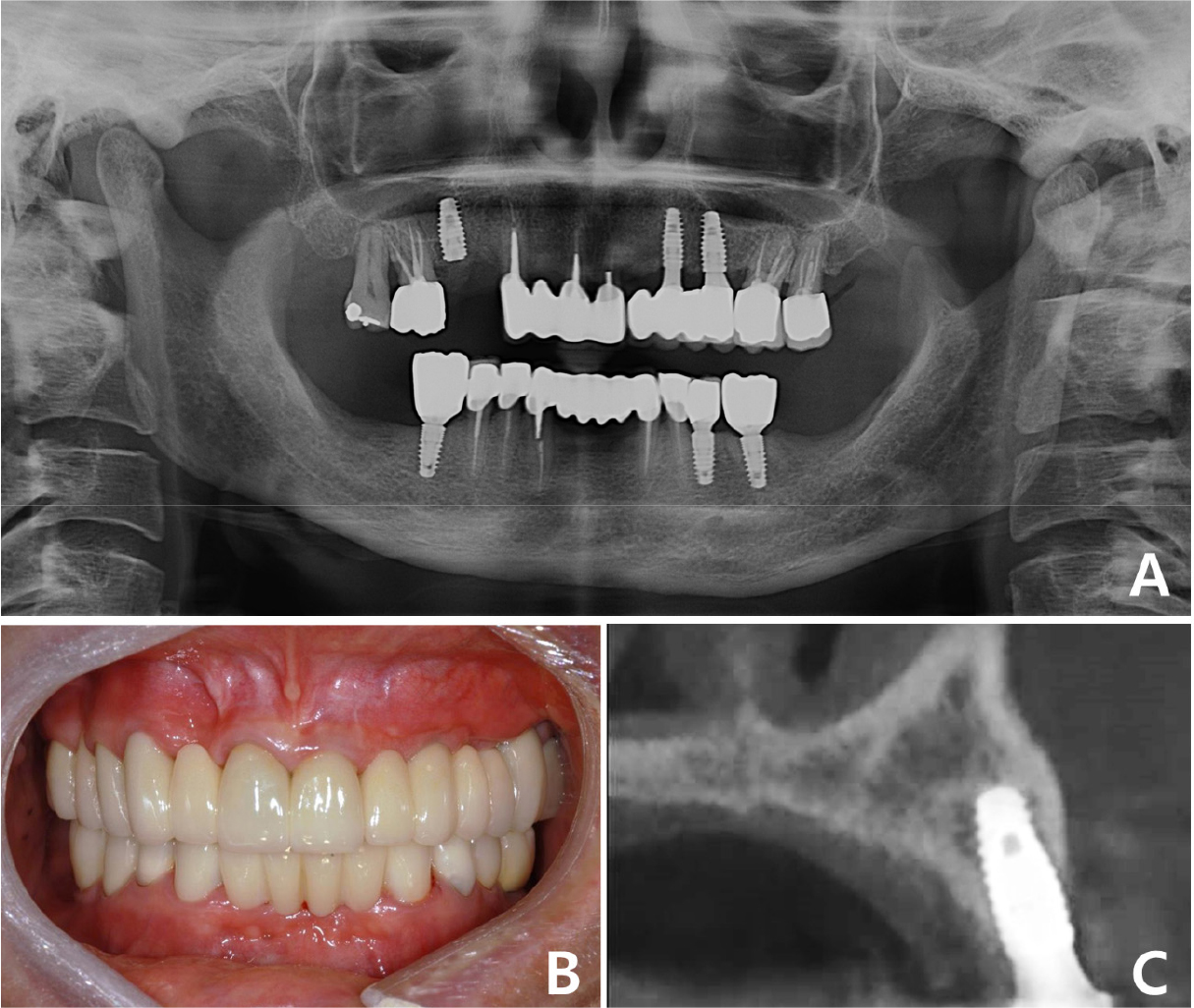
After a sufficient remodeling period of six months, the surgical site was evaluated as stable, and healing abutments were connected. The final 4-unit implant-supported FPD with a mesial cantilever was installed after the provisional phase (Fig. 8A, 8B). All procedures regarding implantation of allogeneic block-bone grafts were successfully performed, and no surgical-site complications were observed on CT three years postoperatively (Fig. 8C). The patient was satisfied with the aesthetic and functional outcomes of full-mouth rehabilitation using implant-supported FPDs.
Ⅲ. Discussion
Severe alveolar ridge atrophy is the main factor that makes aesthetic rehabilitation difficult, especially in the maxillary anterior region. Allogeneic block-bone grafts allow implant placement without additional damage to the patient. Most previous studies have reported successful functional and aesthetic outcomes with allogeneic block-bone grafting. Allogeneic block-bone has a high potential for bone-defect regeneration. Despite the positive clinical results with allogeneic block-bone grafts, their success in terms of long-term prognosis and volume stability of the grafted site is unclear. Comparison of the postoperative and follow-up CBCT images in the two clinical cases presented revealed a decrease in buccal bone thickness at the allogeneic block-bone-grafted site three or four years after implant placement. Schlee et al. reported that the remnants of the allogeneic block-bone were surrounded by newly formed bone matrix and the normal bone marrow was visible between the bony trabeculae.15 In another human histological study in which allogeneic bone grafts were retrieved via biopsy, the grafted sites were very similar to the host’s native bone, and abundant osteocytes were observed within the sections and osteoblasts lined the edges of the calcified structures. In addition, signs of vascularization were observed in all evaluated specimens.16
In 2012, Nissan et al. performed histological and histomorphometric examinations of cylindrical sample cores collected from regions grafted with cancellous bone block during implant placement. They suggested that new bone formation was age-dependent because statistically significant histomorphometric differences regarding newly formed bone and residual cancellous block allograft were found between younger (<40 years) and older (≥40 years) patients, respectively.17 Wilson’ showed that fresh autogenous cancellous bone chips were extensively vascularized by 1 week, and subsequent microscopic healing was rapid. In contrast, although allogeneic chips were incorporated into all defects, vascularization and histological healing rates were lower than those with fresh autogenous graft material. Vascular invasion was noted 1 week after allograft placement, and permeation of the entire graft occurred by 3–6 weeks. At 12 weeks, vascularization and new intramembranous bone deposition equaled those in autografts at 3–6 weeks.18 Thus, implant placement in the maxilla is possible six months after allogeneic block-bone grafting, compared with four months after autogenous bone grafting. Peleg et al. suggested that implant placement is possible after 3–4 months when the allogeneic block-bone is properly fused with the existing bone.19 Therefore, implants can be placed after a bone remodeling period of 3–4 months in younger patients with small defects, and six months or longer in older patients with a severely atrophic ridge requiring sufficient stabilization. Our first patient was young and had a single-tooth defect; therefore, implant treatment was possible four months after bone grafting. However, the second patient was old with a multiple-tooth defect that required sufficient remodeling over approximately six months.
Stable bone conditions were confirmed at all stages and no specific complications were observed in either case. Previous other studies have reported dehiscence or infection as complications of allogeneic block-bone grafts. However, only few graft failures have been reported, although up to 33.3% of patients experienced soft-tissue related side effects.15 Soft-tissue complications did not lead to the total loss of allogeneic block-bone grafts and progression to failure was prevented by applying a topical chlorhexidine gel or removing the exposed allogeneic bone chips beyond the soft-tissue boundary.19 In some cases, the grafted parts that did not fuse with the existing bone were sequestrated, but the available bone was sufficient for implant placement in other cases.13 Similar results were observed in several studies using allogeneic block-bones, and the rate of complications was equivalent to that with autogenous block-bone grafts.20
Ⅳ. Conclusion
We successfully grafted allogeneic block-bone in single- and long-span defects in the maxillary anterior region, with stable aesthetic and functional outcomes at regular follow-up after surgery. However, it is essential to discuss all procedures with the patient and share the possibility of failure and prognosis of allogeneic block-bone grafts.
