

Ⅰ. Introduction
The use of implants in prosthetic rehabilitation for patients with edentulism is a widely accepted dental treatment that not only restores masticatory function but also significantly enhances the quality of life of patients.1 Implant-based treatment options for patients with edentulism can be broadly categorized into removable implant overdentures and fixed implant-supported prostheses.2 Despite the availability of numerous treatment approaches, it remains challenging for clinicians to determine the most appropriate treatment plan.
In patients with complete edentulism, a two-implant-retained overdenture has been proposed as the primary treatment option to achieve the minimal treatment objective.3 However, in cases of a completely edentulous maxilla, the variability in patient conditions makes it difficult to establish a standardized guideline therefore, no consensus has been reached regarding the optimal treatment approach.4
Therefore, we established patient-specific criteria for the optimal number and placement of implants based on different prosthetic treatment approaches in patients with an edentulous maxilla.
Ⅱ. Materials and Methods
The 26 patients included in this study underwent implant placement surgery performed by a single oral and maxillofacial surgeon. Two treatment approaches were used: implant-supported fixed prostheses and implant overdentures.
The analysis included variables such as mean patient age, number of opposing natural teeth, number of opposing implants, mean residual bone height in the maxilla, average number of maxillary implants placed, implant placement sites in the maxilla, economic factors influencing treatment preference, and presence of severe systemic conditions (coagulation disorders, severe diabetes, anticoagulant use, or a history of malignancy).
Ⅲ. Results
The criteria for distinguishing between the two treatment modalities, implant-supported fixed prostheses and implant overdentures, were analyzed. All implants placed in the patients exhibited 100% survival and success rate without any notable complications. Among the 26 patients, 10 received fixed prostheses, and 16 were treated with overdentures. The mean ages of patients in fixed prosthesis and overdenture groups were 65.2 years and 72.8 years, respectively, indicating that the overdenture group was, on average, 8 years older.
Regarding sex distribution, the number of male patients was identical in both groups (seven patients each). However, a significant difference was observed among female patients, with nine in the overdenture group and only three in the fixed-prosthesis group was observed. The number of opposing natural teeth was 7.5 in the fixed prosthesis group and three in the overdenture group, showing that the overdenture group had less than half the number of opposing natural teeth compared to the fixed prosthesis group. The ratio of opposing implants was 4:3 in favor of the fixed prosthesis group.
The mean residual bone height in the maxilla was 13 mm in the fixed prosthesis group and 8 mm in the overdenture group, indicating a difference of 5 mm. The proportion of patients with severe systemic conditions (cancer, bleeding disorders such as liver disease, severe diabetes, or anticoagulant use) was 0.3:0.6, indicating that the overdenture group had twice the proportion of patients with uncontrolled systemic diseases.
The study findings suggest that patients who underwent fixed prosthesis treatment were younger, had more opposing natural teeth, greater residual maxillary bone height, fewer severe systemic diseases, and better financial resources. In contrast, patients treated with implant overdentures tended to be older, had fewer opposing natural teeth, had lower residual maxillary bone height, suffer from more severe systemic conditions, had fewer financial resources, and were more likely to be female.
On average, the fixed prosthesis group received nine implants, whereas the overdenture group received four implants. Implant placement for fixed prostheses was primarily in the central incisors, canines, one premolar, and two molars. Overdenture treatment involved implant placement in either the canines and second premolars or the lateral incisors and first premolars.
Ⅳ. Discussion
Implant-supported treatment of patients with maxillary edentulism offers significant advantages in terms of functional stability, retention, and psychological well-being. Treatment options are broadly classified into fixed and removable prostheses. The selection of an appropriate approach is determined by factors such as patient preferences, economic status, degree of alveolar bone resorption, soft tissue conditions, inter maxillary relationship, facial profile, lip support, smile line, and radiographic findings.
Most patients seeking implant treatment at dental clinics initially require fixed prostheses. Fixed implant-supported prostheses provide complete support from the implants, ensuring greater stability, improved oral function, enhanced esthetics, and better psychological and social well-being. However, the final treatment decision should be made based on a comprehensive examinations, diagnosis, and a well-structured treatment plan that considers the aforementioned factors.
As shown in the Table 1, the patients eligible for implant-supported fixed prostheses had a significantly lower average age and half the prevalence of uncontrolled systemic diseases than those in the overdenture group. Considering that advanced age and female sex are generally associated with lower residual bone height and decreased bone quality, the proportion of female patients in the overdenture group was thrice higher than that in the fixed prosthesis group. Regardless of sex, patients with greater residual bone height and more opposing natural teeth were more likely to require implant placement, leading to a higher tendency for fixed prosthesis treatment.
In the present study, patients receiving implant-supported fixed prostheses commonly had implants placed in the central incisors, canines, one premolar, and two molars, whereas those undergoing implant overdenture treatment typically had implants placed in either the lateral incisors and first premolars or the canines and second premolars. The analysis presented in Table 2 demonstrates it is evident that the placement of maxillary implants was adjusted according to the number of opposing mandibular molars and premolars.
Table 1.
Comparison of patient distribution between implant-supported fixed prosthesis and overdenture treatment groups based on analytical factors
| Mean age | Male-to-female ratio | Severe systemic conditions proportions | Mean residual bone height | Average number of opposing teeth | |
| Fixed prosthesis | 65.2 | 0.43 | 0.3 | 13 | 7.5 |
| Overdenture | 72.8 | 1.29 | 0.6 | 8 | 3 |
Table 2.
Distribution and number of maxillary implants based on the number and location of opposing mandibular teeth in implant-supported fixed prosthesis treatment
| M2, PM1 | M1, PM2 | M1, PM1 | |
| M2 | 5 | . | . |
| M1, PM2 | . | 3 | . |
| M1, PM1 | . | . | 2 |
In the cases presented in this study, when both mandibular molars were present, corresponding maxillary implants were placed in both molar regions (Fig. 1A). Similarly, when one mandibular molar and two premolars were present, the maxillary implants were placed with one molar and two premolars (Fig. 1B). The cases in which one maxillary premolar and one molar implant were placed in alignment with the opposite mandibular teeth supported a fixed prosthesis (Fig. 1C).
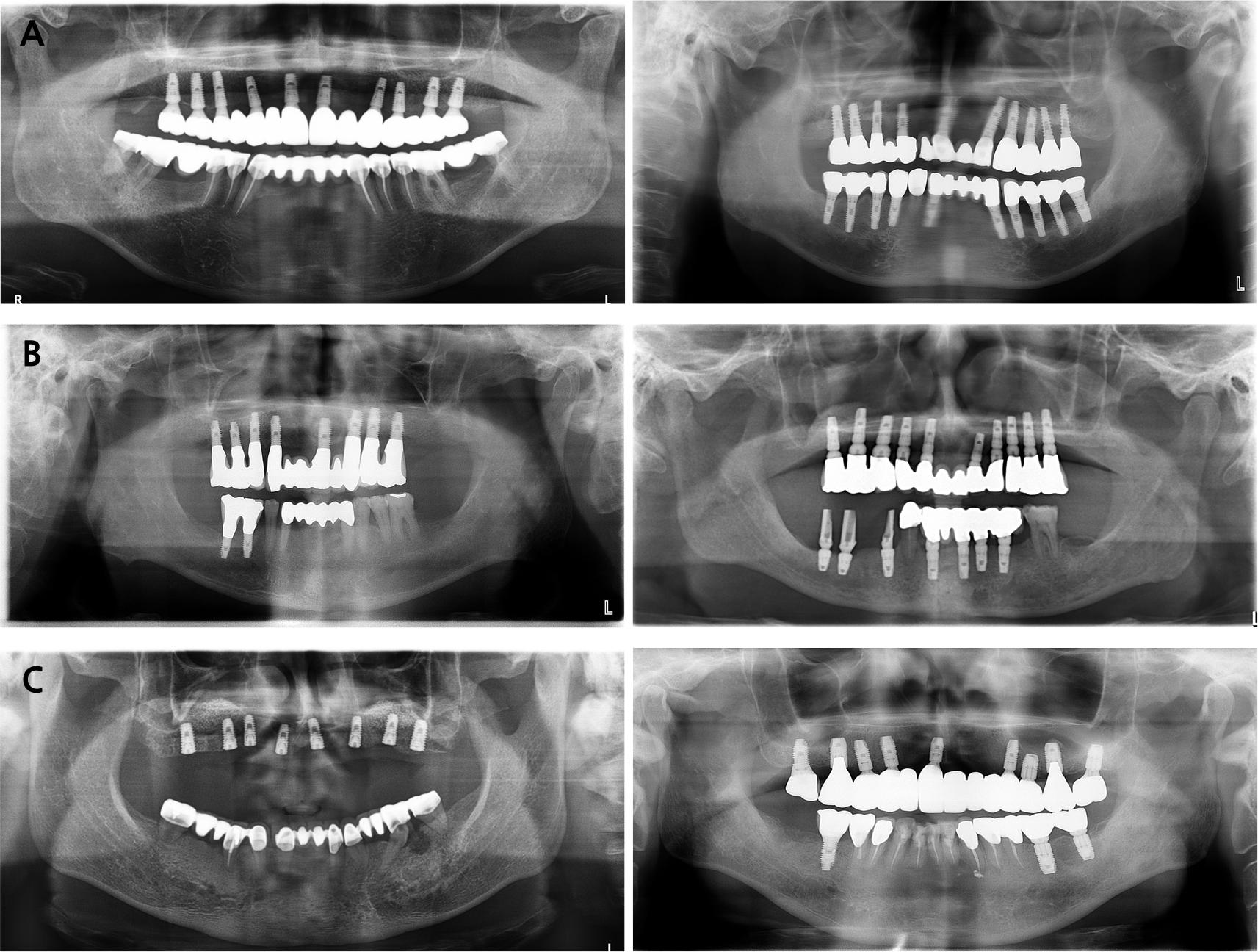
Fig. 1.
Maxillary implant placement according to the presence of mandibular opposing premolars and molars in implant-supported fixed prosthesis treatment. (A) Both mandibular molars are present, (B) One mandibular molar and two premolars are present, (C) One mandibular molar and one premolar are present.
Misch proposed that optimal implant placement for fixed maxillary prostheses should include the central incisors, bilateral canines, bilateral second premolars, and bilateral first molars (#11 or #21, 13, 15, 16, 23, 25, 26), as this configuration minimizes stress within an ovoid arch, providing an optimal biomechanical distribution.5
By contrast, patients with insufficient residual bone or a narrow alveolar ridge require guided bone regeneration (GBR) or ridge splitting procedures. However, the additional procedures inevitably prolong the treatment period and increase the risk of complications, posing a challenge for both clinicians and patients. Consequently, in such cases, implant overdentures are the preferred treatment due to patient-related factors.6
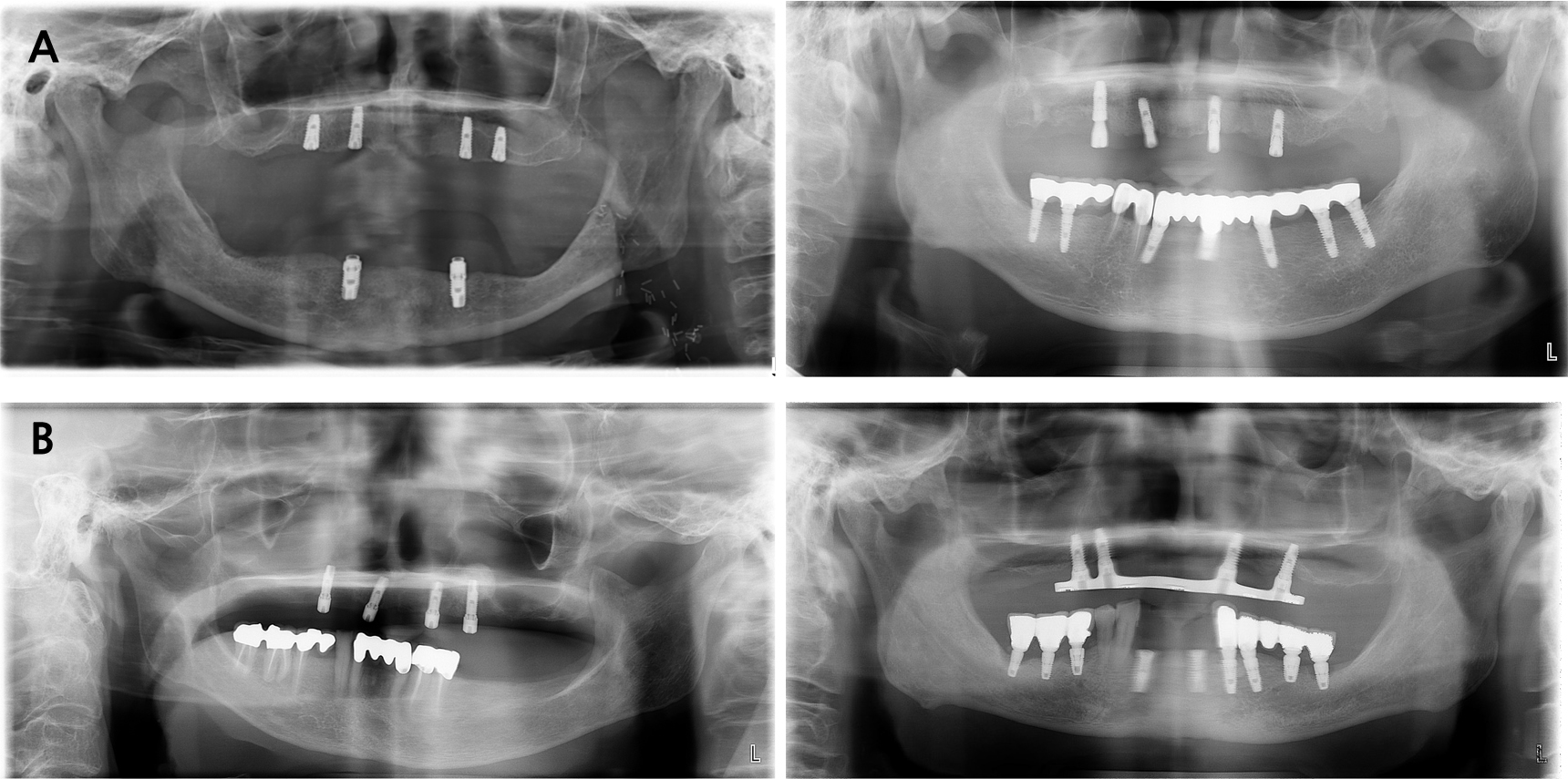
In this study, implant placement for overdentures was commonly performed on the maxillary lateral incisors and first premolars or the canines and second premolars. Table 3 shows the relationship between the location and number of opposing mandibular teeth and maxillary implant placement sites. Thus maxillary implant placement for overdenture support was performed independently of the location of the opposing mandibular teeth. (Fig. 2A and 2B).
Table 3.
Analysis of maxillary implant placement location and number based on the distribution and number of opposing mandibular teeth in implant overdenture treatment
| LI, 2nd PM | C, 1st PM | |
| LI, 2nd PM | 4 | 5 |
| C, 1st PM | 3 | 4 |
According to Raghoebar, Sadowsky, and Jemt, when comparing implant and overdenture survival rates based on the number of implants and whether they were splinted, overdentures supported by four or more splinted implants demonstrated higher survival rates for both implants and prostheses. Furthermore, a wider distribution of implants in overdenture treatments has resulted in better prognoses. This principle stems from the fact that maxillary bone quality is inferior to mandibular bone quality. Although a two-implant overdenture is commonly recommended for the mandible, a minimum of four implants is required for the maxilla to ensure optimal outcomes.7,8,9
Additionally, Slot and Katsuolis reported that when four or more implants were used, no significant difference was observed in implant survival rates between cases where six implants were placed and those where only four implants were placed, whether in the anterior or posterior region.10,11
One of the limitations of this study was its small sample size. The number of patients in the implant-supported fixed prosthesis group was significantly lower than that in the overdenture group, making it difficult to draw statistically significant conclusions. Additionally, because more than one specialist was involved in the prosthetic treatment, a possibility of operator-dependent variability existed during the treatment planning phase.
Ⅴ. Conclusion
This study is significant because it provides clear guidelines on the optimal number and placement of implants for different implant-supported prosthetic treatment plans, an area for which no universally accepted criteria have been established. For implant-supported fixed prosthesis treatment, placing eight implants, including bilateral central incisors, canines, one premolar, and two molars, has been demonstrated to yield favorable prognoses. In the case of implant overdentures, placing four implants, either in the bilateral lateral incisors and first premolars or in the bilateral canines and second premolars, was sufficient for successful treatment outcomes.
