

Ⅰ. Introduction
Since the concept of osseointegration was introduced by Brånemark, implant treatment in partially or completely edentulous patients has become one of the most reliable treatment methods with excellent clinical results; this is due the continuous development of technology.1, 2, 3 As the use of dental implants becomes common, complications are also increasing. Implant complications can be largely divided into biological and mechanical complications, and the causes of complications in each case are diverse. Biological complications include peri-implant mucositis, peri-implantitis, marginal bone resorption, implant loss, etc. Mechanical complications refer to complications occurring in the implant, implant components, and superstructure.4 According to Shemtov-Yona and Rittel, unlike biological complications that occur during a relatively short follow-up period, mechanical complications of implants occur later and more frequently.5 At the same time, the authors emphasized the need to prepare for mechanical complications because implants are placed as a more general treatment method and the lifespan of existing implants increases. When deformation or implant structural fracture occurs, various methods must be considered for repair, ranging from a simple method of replacing the structure to a complex method of removing even a fixture, depending on the degree of damage to the implant structure.6 Among various mechanical complications, in particular, many studies have reported abutment screw loosening. According to Sadid-Zadeh et al., a higher frequency of abutment screw loosening was reported in a posterior area than in an anterior area, which was attributed to a higher load.7 If the screw is simply loosened, clinicians can check the screw to confirm that there is no problem and tighten it again; however, if the screw has a problem or the loosening phenomenon persists for a long time, screw fracture, abutment wear, deformation and even fixture fracture can result. If there is a problem with the abutment or fixture, even if the screws are re-tightened, problems such as micro-movement of the prosthesis can continue. There are two methods of taking an impression of an implant prosthesis: the conventional method of transferring the implant’s position using impression material, impression coping and laboratory analog, and the digital scanning method using an intraoral scanner. Although the conventional method is generally used, errors may occur during the process of locating the impression coping or making a working model, which may cause discomfort or induce a vomiting reflex in the patient while waiting for the impression material to be placed. Additionally, as the number of implants increases, the skill of the clinicians becomes more sensitive; therefore, a digital scanning method using an intraoral scanner has emerged as a method to overcome these disadvantages. In the case of fabricating a prosthesis according to a digital workflow using the digital scan method, the entire process of impression taking, working model making, wax mold production, etc., does not require materials or time; thus, the overall process is efficiently performed on the computer.8
Recently, with the rapid development of computer technology in the dental industry, a custom implant system using computer-aided design and computer-aided manufacturing (CAD-CAM) has been introduced into dentistry.9, 10 The customized implant system has the advantage of being able to fabricate an aesthetic prosthesis because it can adjust the retention force and insertion path of the prosthesis using an abutment fabricated by optimizing the emergence profile of the patient's tooth, and the margin of the prosthesis can be set subgingivally. Additionally, since the margin can be formed according to each gingival shape, side effects caused by residual cement or food press-in can be prevented, and hygiene management is easy, which is advantageous to the health of tissues around the implant.11 However, in order to use the digital method, components suitable for the implant system, such as the scan body and digital laboratory analog, are required.
Since the 1990s, the use of implants in the dental field has increased in earnest, and the size of the implant company market continues to grow both at home and abroad. In addition to famous companies, such as Straumann, Danaher, Dentsply Sirona, Osstem, and Dentium, there are numerous implant companies, each with their own strengths. However, clinicians select the type of implant system based on various judgments. During market development, problems, such as old implants being discontinued or related components not being imported into the country, may occur. Clinicians may be in a difficult situation when a problem occurs with an implant for which components are difficult to obtain, and no guidelines have been presented to solve this situation. Therefore, in this case, an upper implant prosthesis was made by directly fabricating implant components that are difficult to obtain in the Republic of Korea, and this report is considered to have great clinical implications considering the patient’s age.
Ⅱ. Case Report
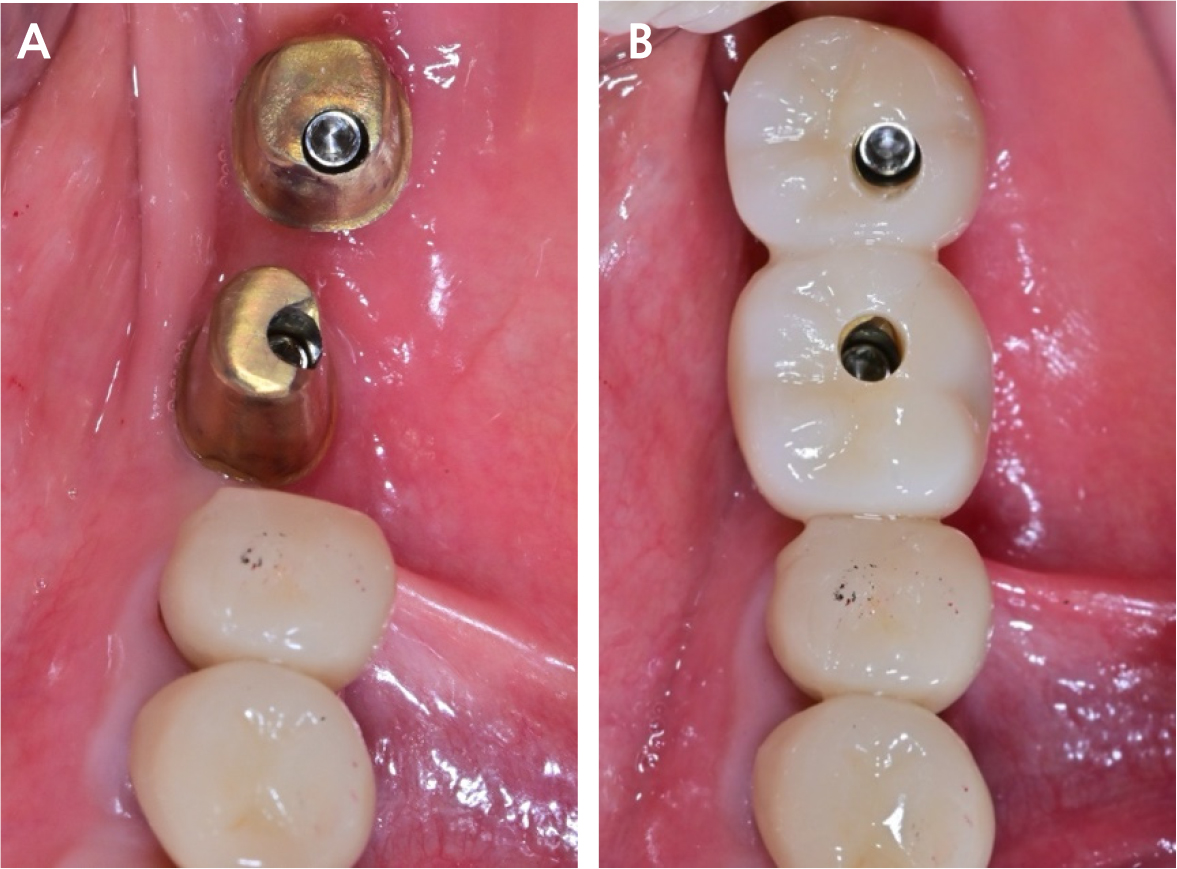
A 73-year-old woman was referred for prosthetic treatment of a maxillary left molar implant at the Department of Oral and Maxillofacial Surgery of the Seoul National University Dental Hospital. Due to pain in the left temporomandibular joint and limited mouth opening, she was receiving treatment with arthrocentesis at the Oral Medicine and Oral and Maxillofacial Surgery department of the same hospital. We found that an implant fixture in the lower left first molar area which was a Zimmer's Spline Φ3.25, and the second molar area which was TSV Φ4.5 from the same company. Periapical radiography showed mild marginal bone loss in the first molar area; however, there was no inflammatory reaction or fixture damage. Osseointegrations of both the implants were intact (Fig. 1A). It was determined from clinical examination that the occlusal dimension of the existing implant prosthesis in the lower left posterior teeth, which is the antagonist, was low. When the existing prosthesis was removed from the oral cavity and evaluated, plaque deposition and wear of fixture connection area of the abutment and some ill-fitting margins of crowns were observed (Fig. 1B and 1C). In order to recreate a harmonious occlusal plane, it was necessary to remake the implant prosthesis. When remaking an implant prosthesis, as a general method, after removing the existing prosthesis, an impression coping suitable for the fixture is connected, and an impression using an impression material such as polyether is obtained. However, components of the implant were not officially imported into the Republic of Korea, thereby making it impossible to take impressions in the traditional way. A domestic company produced a digital scan body (Scanbody Z2, Z6; Dentalrix, Daegu, Korea) compatible with the Zimmer's Spline and TSV (Fig. 2A). Therefore, a new prosthesis had to be fabricated with a digital workflow instead of the traditional method. First of all, after attaching each digital scan body suitable for the fixture, scanning was performed using an intraoral scanner (Trios 3; 3Shape, Copenhagen, Denmark). The implant at the lower left second molar position could be remade using a conventional method by a scan body and ready-made digital laboratory analog. However, the Spline system at the first molar position was not supplied domestically; therefore, it was directly fabricated using digital technology. The connection part that comes into contact with the fixture of the digital scan body is similar to the intaglio on the top of the fixture. Therefore, scanning the digital scan body using an industrial high-resolution, high-precision non-contact image measuring device (Wintek Classic 3020; Wintek Technology, Singapore) was conducted (Fig. 2B and 2C). Data of the top of the fixture was reproduced using the principle of reverse engineering, and CAD software (Solidworks Professional 2019; Dassault Systèmes, Vélizy-Villacoublay, France) was used to merge with the lower part of digital laboratory analog (IZEN implant) data (Fig. 3). A customized digital laboratory analog was fabricated using a three-dimensional (3D) printer (Cara Print 4.0; Kulzer GmbH, Hanau, Germany) and resin (Print Stone Beige; Kulzer GmbH) (Fig. 4A). Based on intraoral scan data, a digital working model was fabricated using a 3D printer (Pro 3D printer; SprintRay, Los Angeles, USA) and resin (S-Plastic model 2.0; Graphy Inc., Seoul, Korea). A ready-made digital laboratory analog for the lower left second molar and a customized digital laboratory analog for the first molar were installed in the digital working model (Fig. 4B). These data were transferred to the CAD software (exocad DentalCAD; exocad GmbH, Darmstadt, Germany) (Fig. 4C). The definitive customized abutments and zirconia crowns were designed using the same software (Fig. 4D and 4E). The definitive prostheses were evaluated for their connection with the implant fixture, occlusion, and aesthetics, and were placed in the patient's mouth (Fig. 5). The patient expressed satisfaction with the functional and esthetically improved prosthetic treatment.

Fig. 1.
Initial condition of implant-restoration complex. (A) periapical radiograph showing mild alveolar bone loss and ill-fitting margins of prostheses, (B) clinical photograph of implants, (C) extraoral photograph of old implant prostheses showing wear, ill-fitting margin, and dental calculus deposition.
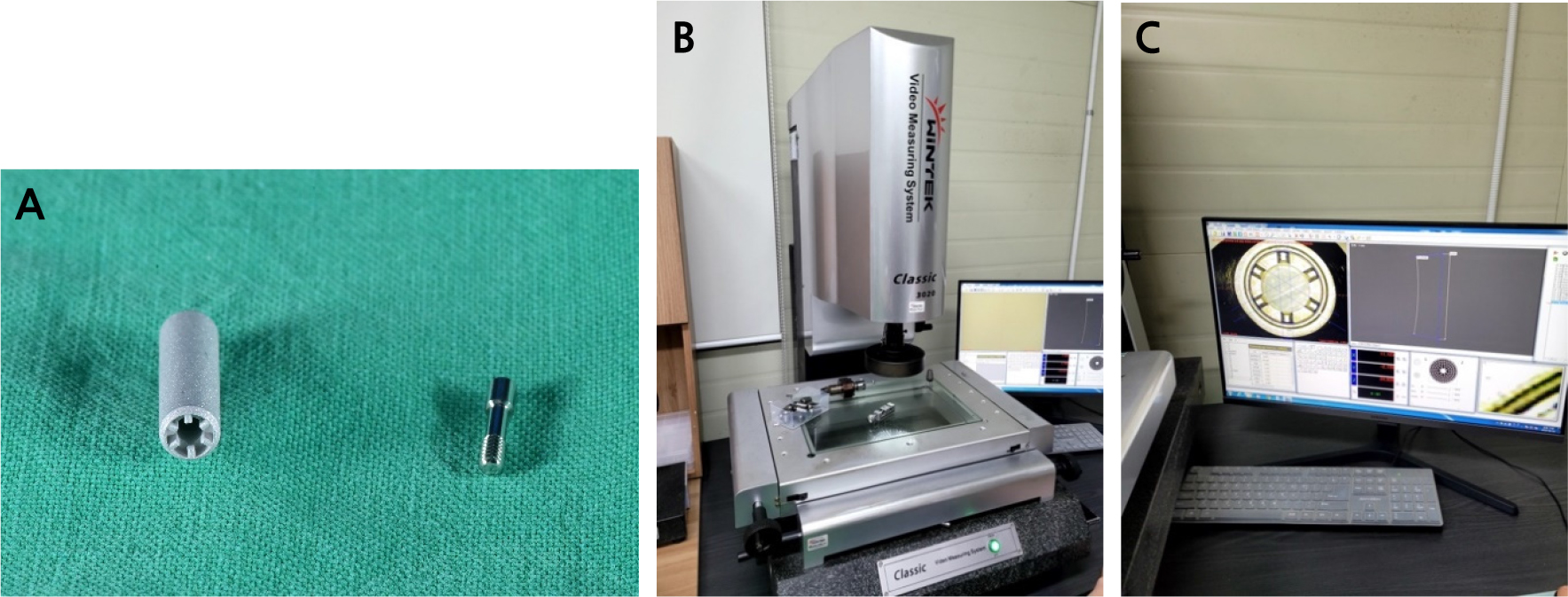

Fig. 3.
Design process of customized digital laboratory analog of Zimmer Spline 3.25. (A) scan body design, (B) inverted form of scan body data, (C) laboratory analogue data of TSV implant, (D) using reverse engineering and CAD software, the intaglio of the scan body was merged with the lower part of the laboratory analog of another implant system.
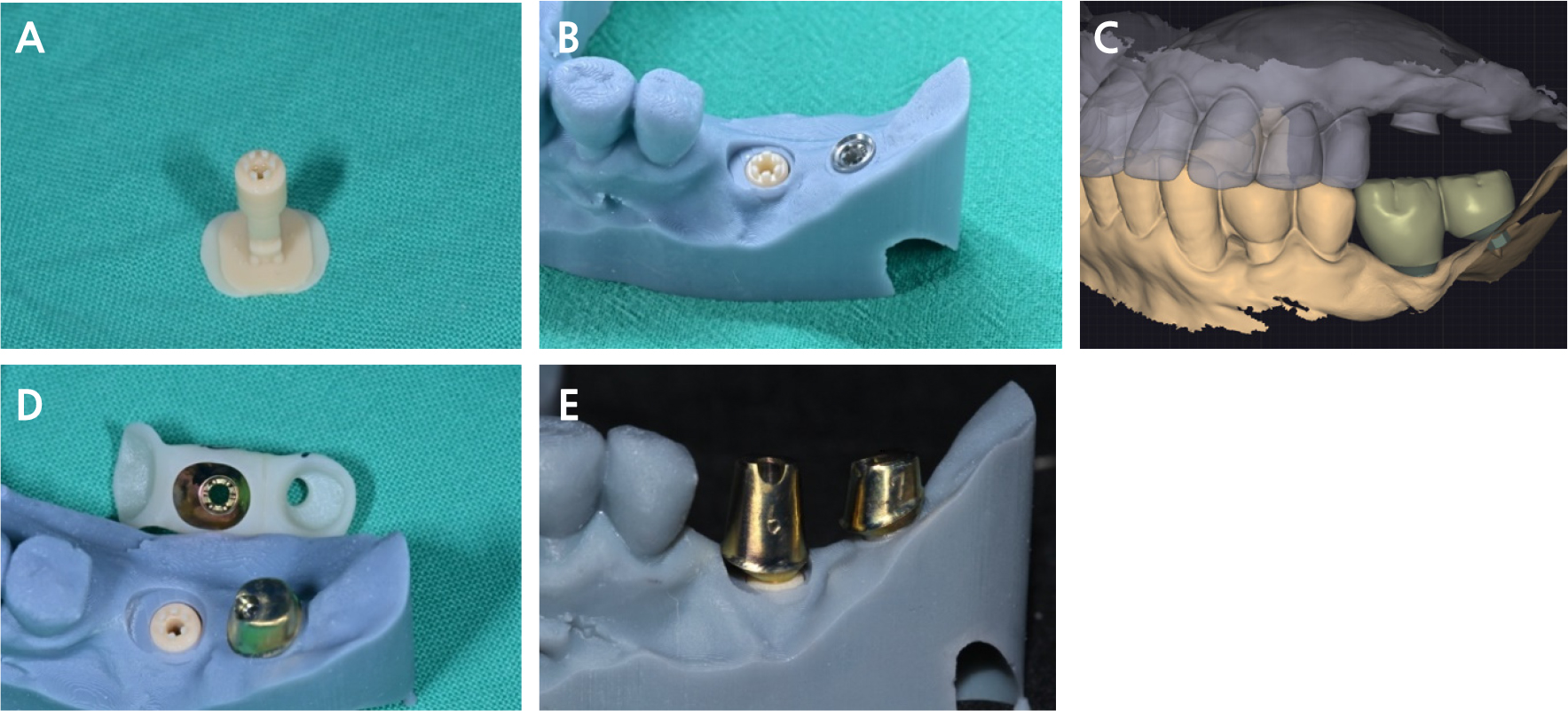
Fig. 4.
Digital laboratory analog and customized abutment. (A) three-dimensionally printed customized digital laboratory analog of Zimmer Spline 3.25, (B) three-dimensionally printed working model with laboratory analog, (C) superstructure design, (D) jig for abutment placement, (E) customized abutment connected to the laboratory analog.
Ⅲ. Discussion
In the 1990s, as dental implant treatment was introduced in earnest in the Republic of Korea, implants from various companies exist in the oral cavity of patients. Although numerous implant companies exist, not all of them may continue to produce parts. Products continue to evolve, and older models may become obsolete. However, depending on the national system, it may be difficult to import products from overseas. Various complications can occur in an implant due to various causes, among which is if the screw or abutment is damaged, the prosthesis must be remade by taking an impression from the fixture level. When faced with this situation, it can be disconcerting for the clinician if such components are not available. Using the method reported in this paper, even the upper prosthesis can be fabricated by directly making components that are not present. As implants become more popular and product types become more diverse over time, the technology to fabricate customized components has great clinical significance. A study by Huh et al. reported errors that may occur due to differences in data acquisition methods for each system in the CAD-CAM technology and those that may occur during the design and when fabricating the wrong abutment. Additionally, they reported the milling bar diameter and causes of errors that may occur in the CAD-CAM systems, such as errors due to wear and those occurring when converting scan files to STL files.12 Various steps, such as precision scanners, libraries, CAD software for merging data, and three-dimensional printers have been taken to fabricate customized implant components, and there are steps that can cause errors until the process of mounting them to the working model. Therefore, further studies are needed on the accuracy and clinical long-term prognosis of this method.
Ⅳ. Conclusion
For reasons such as abutment and prosthesis damage or an unacceptable occlusal table, there are cases in which a previously used implant prosthesis needs to be remade. In such cases, components suitable for the implant system, such as impression coping and laboratory analog, are required. In this case, a digital laboratory analog of an implant system, which is difficult to obtain in the Republic of Korea, was directly fabricated using reverse engineering and CAD-CAM technology. A successful prosthesis was placed, and the patient was satisfied with the functional and esthetically improved prosthetic treatment that was clinically meaningful. Further studies on the accuracy and long-term prognosis of this method are needed.
