

Ⅰ. Introduction
Microstomia is defined as a small oral aperture, and its etiology can be either congenital or acquired.1 Hypertrophic scarring and contractures from facial traumas, burn injuries, radiotherapy, and reconstructive surgery following perioral tumor resection often lead to microstomia.1, 2 Connective tissue disorders, such as scleroderma can also reduce mouth opening.2 Individuals with microstomia often experience aesthetic and functional issues, including shortened mouth commissure, limited mouth opening, difficulty in eating and drinking, and forceful blowing and swallowing.3 Additionally, patients with microstomia suffer from improper speech and sound production.3 Hence, in order to enlarge the oral aperture, commissurotomy is mandatory. Moreover, simultaneous vestibuloplasty may be required to obtain vestibular space for denture placement.4, 5
In this retrospective case study, we report total occlusal rehabilitation for a complicated case of microstomia associated with limited mouth opening and complete edentulism. A staged approach combining oral and maxillofacial surgery and prosthodontics was described.
Ⅱ. Case Report
Ethical approval for this study was obtained from the Institutional Review Board (S2018-0257-0001). On November 5, 2009, a 58-year-old female patient was referred to a local clinic for dental restoration. The patient had measles at the age of 4 years and skin necrosis on the left cheek, which may be due to a gangrenous disease affecting the soft and hard tissues of the mouth and face. At the age of 10 years, the patient underwent free flap reconstruction of the left cheek. However, progressive muscle contracture of the free flap led to facial asymmetry and microstomia. At the age of 32 years, she had tuberculosis and had taken medications for several weeks for treatment. One year after the patient recovered from tuberculosis, she underwent hysterectomy.
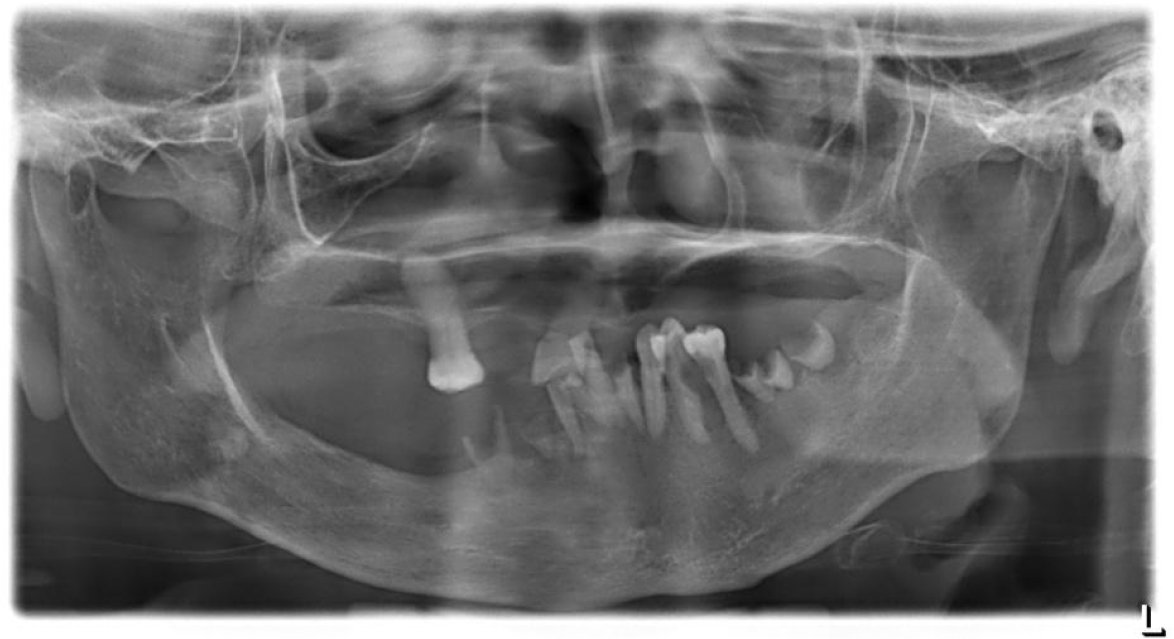
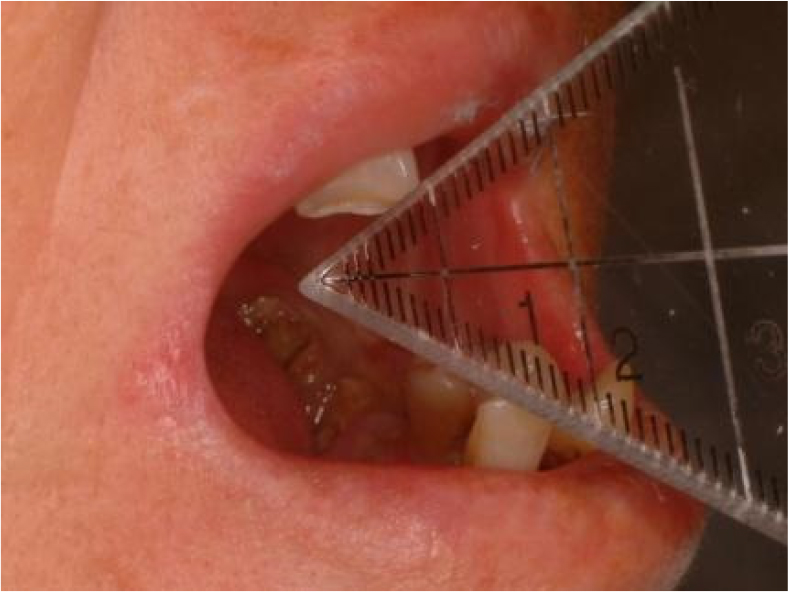
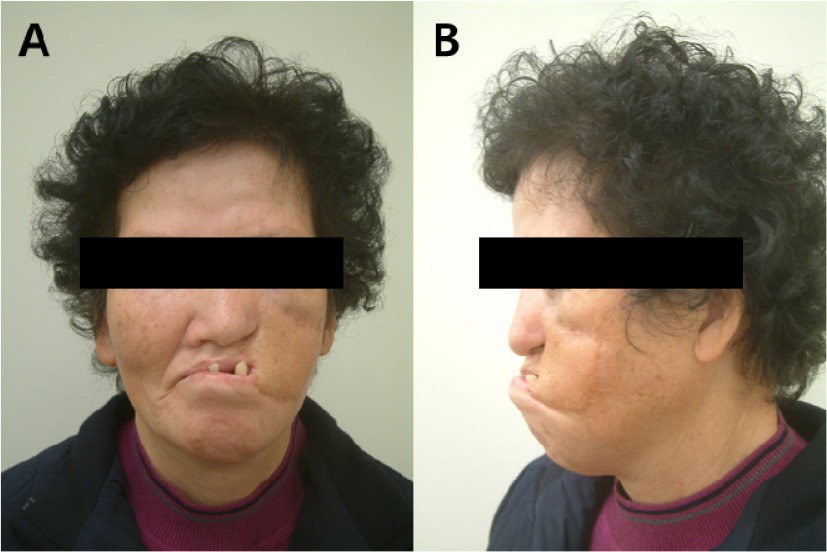
When the patient presented to the Department of Oral and Maxillofacial Surgery, an initial panoramic radiograph revealed multiple retained root tips and missing teeth (Fig. 1). The patient was unable to maintain good oral hygiene because of limited mouth opening. Extra-oral examination revealed a 12-mm mouth opening and facial asymmetry with an anterior crossbite due to maxillary deficiency (Figs. 2 and 3A, 3B, respectively). Underdevelopment of the maxilla was associated with muscle contracture from the previous free flap. Intraoral examination revealed multiple missing teeth, retained roots, and loss of the buccal vestibule.
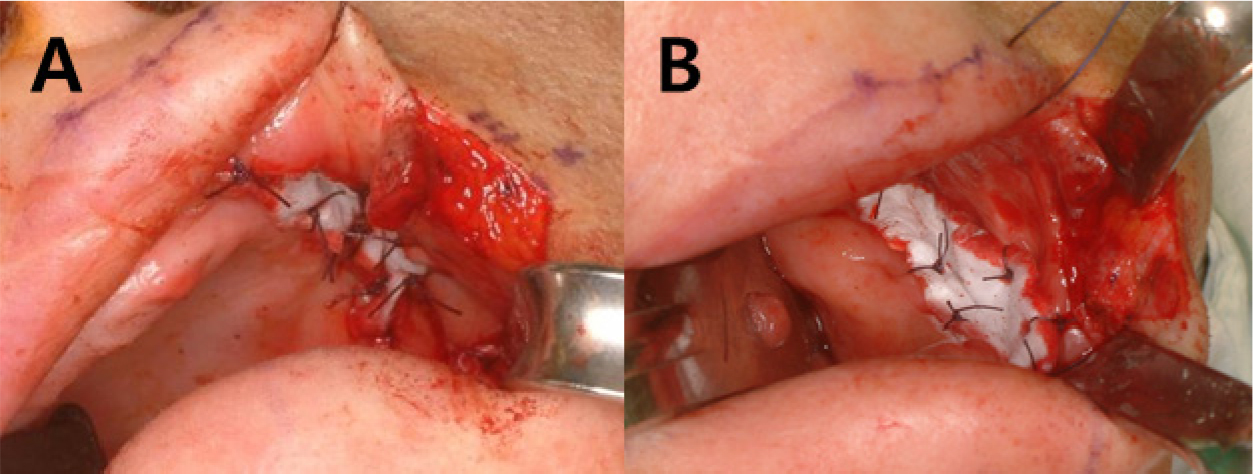
Based on a thorough clinical and radiographic examination, a staged reconstruction of the corner of the mouth was discussed and planned. Under local anesthesia, multiple retained roots were extracted in the first step. On January 13, 2010, under general anesthesia, left commissurotomy was performed to increase maximal mouth opening (Fig. 4A to 4C). The right commissure to the midline was measured. The design for commissurotomy was marked using the right commissure as a guide for positioning the new commissure, which was equidistant from the midline (Fig. 4A). First, the triangular area of the scar tissue on the left commissure was excised. The exposed oral mucosa was advanced and sutured to the skin edges. Vestibuloplasty of the left posterior maxilla and mandible was performed using supraperiosteal dissection and a collagen sheet (Terudermis®; Terumo Co., Tokyo, Japan) graft (Fig. 5A, 5B). Postoperatively, the patient maintained a small bite block for 2 weeks to avoid acute postoperative relapse.

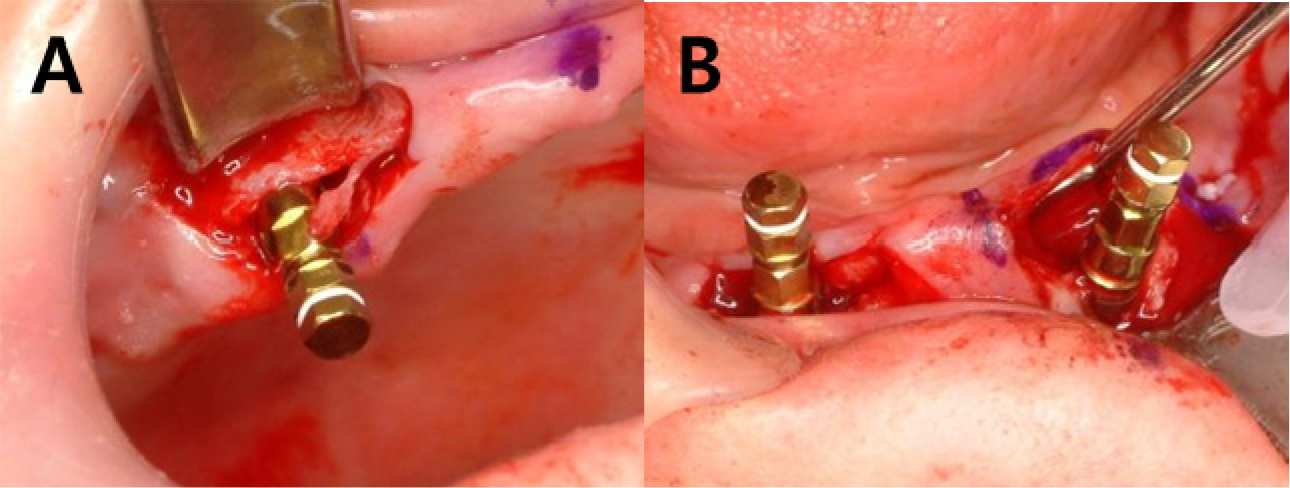
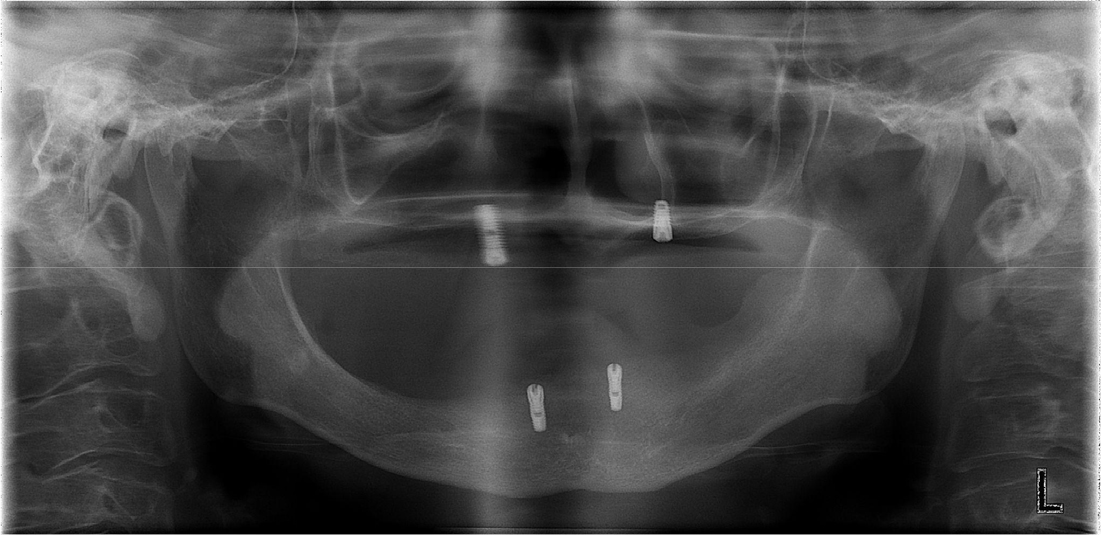
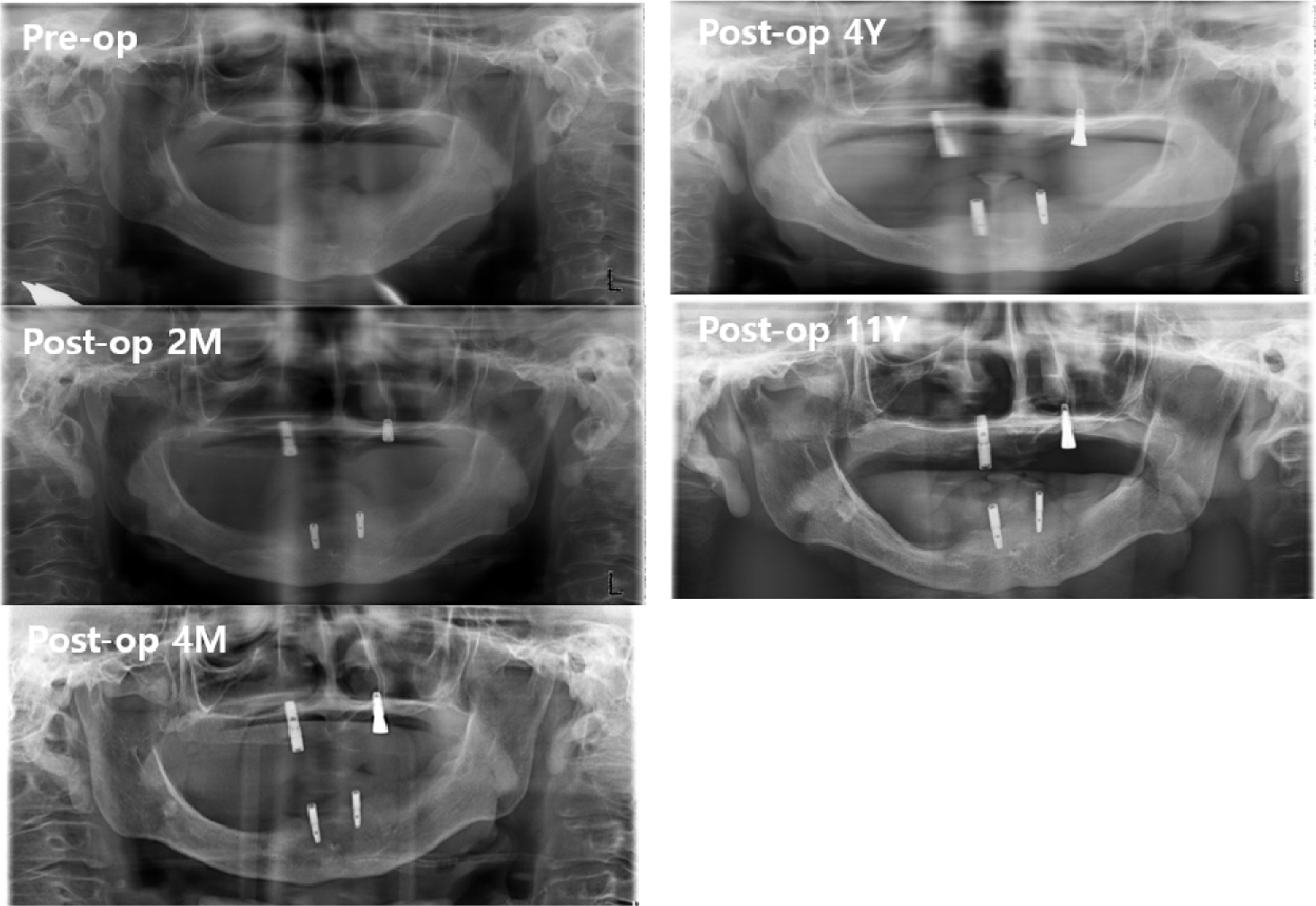
Postoperatively, the maximum mouth opening was increased from 12 to 35 mm, and the oral commissure was enlarged. After 2 months of recovery, temporary complete upper and lower dentures were delivered to the patient (Fig. 6). On January 19, 2011, two implants were placed in each arch under general anesthesia (Fig. 7). A panoramic radiograph revealed four implants (Fig. 8). At the Department of Prosthodontics, magnet-attached overdentures were fabricated and delivered 6 months after implant installation (Fig. 9). Vestibuloplasty creates a larger surface area for better denture adaptation. The patient was followed-up for 11 years without any complications (Fig. 10).


Ⅲ. Discussion
Noma is a devastating infectious orofacial gangrenous disease that can lead to severe destruction of the soft and hard tissues.6, 7 The peak incidence of acute noma is between the ages of 1 and 4 years.7 However, its cause remains unknown.6 Malaria, malnutrition, measles, and poor oral hygiene may be risk factors for the development of noma lesions.6 Patients affected by noma can later exhibit serious facial disfigurement, trismus, ankylosis, oral incontinence, and speech problems.6, 7 Resultant wound contraction can lead to mouth stricture, which can progress to complete closure of the mouth aperture with intertwining teeth and bony fusion between the maxillomalar complex and the mandible, a condition that is extremely difficult to correct surgically.6 In this patient, the etiology of microstomia was measles; however, the exact medical records could not be obtained because of the distant timing of the surgery.
Patients with microstomia have difficulty inserting and removing prostheses.2 In this case report, the patient required commissurotomy to increase the maximal opening of the oral aperture. Commissurotomy also facilitates the enlargement of the intercommissural and interincisal distances and enables the insertion and removal of implant-supported overdentures. Moreover, it allows easier advancement of the mucosa and muscle to cover the defect from the excised scar tissue.8 However, in most cases, a staged approach is recommended.9 Postoperative scar contracture and asymmetry are often observed.2, 9
In addition to commissurotomy, vestibuloplasty was also required to increase vestibular depth and elevate the floor of the mouth.5 According to Isidor et al., decreased vestibular depth and elevated mouth floor require vestibuloplasty to increase prosthetic stability, retention, and function.5 It helps to enhance prosthetic retention and create an adequate area for prosthetic placement.5 In this case report, with the use of Terudermis, painful tissue harvesting was avoided, and a sufficient band of keratinized mucosa was generated.10 Additionally, the operative time was reduced. Terudermis is a bilayer graft comprising an outer silicone layer and an inner layer of mixed atelocollagen.11 The inner collagen layer works as a scaffold for cell migration and epithelialization, while the outer silicone layer functions as a barrier for protection.12 At 2 weeks postoperatively, the silicone layer was removed.
Compared to a conventional complete mandibular denture, an implant-supported mandibular overdenture is reliable and effective for reconstructing the edentulous mandible.4 It demonstrates a significant improvement in function, esthetics, and quality of life.10 Two-implant overdenture is known to be the first treatment option for patients with edentulous mandible.12 To increase support and retention of removable overdentures, various attachments have been used.14 In this case report, magnetic attachment was used, which has the advantages of a small size, strong attachment force, ease of cleaning, ease of placement for both the dentist and patient, and automatic reseating.13, 14,15 Additionally, magnetic attachments prevent the abutment from traumatic injury by the lateral force of the upper prosthesis.14 According to a study by Song et al., the dome-shaped magnet attachment had greater resistance in vertical and lateral retentive force than the flat-type magnet attachment.13
Compared with ball and attachments, magnet attachment has the least amount of strain regardless of implant number and distribution.16 However, magnets require encapsulation within an inert alloy because of poor corrosion resistance within oral fluids.15 In the 11-year follow-up, the upper and lower implant-supported overdentures were in good condition. The patient did not experience any pain around the implants. Implant mobility was not observed. The maximum mouth opening was reduced by approximately 5 mm, which may be due to inevitable scar contracture.
Ⅳ. Conclusion
Full-mouth rehabilitation of patients with microstomia and limited mouth opening requires both surgical and prosthetic procedures. Staged reconstruction using a multidisciplinary approach is necessary to achieve optimal aesthetic and functional outcomes. Commissurotomy and implant-supported overdentures are the most efficient and simple methods for rehabilitation of microstomia.
