

Ⅰ. Introduction
Ⅱ. Case Presentation
1. Case 1
2. Case 2
3. Case 3
4. Case 4
Ⅲ. Discussion
Ⅳ. Conclusion
Ⅰ. Introduction
Maxillary sinus pneumatization limits available bone height for implant placement in the posterior maxilla.1 To address this, maxillary sinus floor elevation (MSFE) was introduced. Based on residual bone height, either lateral or transcrestal MSFE has been recommended.2 With technological and material advancements, the threshold for selecting the MSFE approach has become somewhat equivocal. However, when adequate primary implant stability is difficult owing to limited residual bone, lateral MSFE remains necessary.3
After MSFE, a contained space is created and filled with bone substitute material and a blood clot, surrounded by the sinus bone walls and membrane. Bone formation then initiates within this space. Osteogenic sources predominantly arise from the sinus bone walls, as demonstrated in several clinical studies on endo-sinus bone formation.4,5,6,7 These studies showed that sites with a narrow sinus and greater residual bone thickness exhibited more favorable new bone formation than those with wider sinuses and reduced bone height. Another osteogenic source is the sinus membrane, where mesenchymal stem cells have been shown to contribute to new bone formation.8
Although the sinus provides a favorable environment for bone formation, the augmented space generally undergoes some shrinkage after MSFE. The degree of shrinkage depends on the type and origin of the graft material, sinus size, and the number of missing teeth.9
However, if additional secluded space is created in the maxillary sinus after MSFE owing to specific events, bone formation may occur in that space, independent of shrinkage in the originally bone-inserted area. This space becomes influenced by the adjacent sinus bone wall and membrane, creating conditions favorable for bone formation. Indirect evidence is found in previous case reports.10,11,12 In these studies, after removal of a cyst, tooth, or implant, spontaneous bone formation (SBF) was observed in the newly created cavity. Consistent with these findings, we observed SBF beyond the bone-grafted area following lateral MSFE, a rarely reported occurrence. Therefore, this case series aimed to present unexpected SBF after lateral MSFE, along with relevant radiographic changes.
Ⅱ. Case Presentation
In four patients, lateral MSFE was performed with or without implant placement. Patient demographics are presented in Table 1. A bony access window (approximately 10 × 15 mm) was created on the lateral surface of the maxillary sinus. The sinus membrane was gently detached from the bone wall, followed by grafting with particle-type bone substitute material (OsteonXeno; Genoss, Suwon, Korea) and coverage with a collagen membrane (Collagen membrane 2, Genoss). The apico-coronal extent of membrane elevation was sufficient to accommodate implants of 10–12 mm length. The medial sinus membrane was also carefully detached to avoid uneven medio-lateral graft packing. No sinus membrane perforation was clinically detected during the procedures (via direct visual inspection and the Valsalva maneuver). Bone grafting continued until moderate resistance was felt during insertion. Post-operatively, all patients received antibiotics (Ciprofloxacin 250 mg; Daewoong Pharmaceutical Co., Seoul, Korea) and non-steroidal anti-inflammatory drugs (Anaprox 275 mg; Chong Kun Dang Pharmaceutical Co., Seoul, Korea) for 1 week. Patients reported mild sino-nasal symptoms at 1 week. Cone-beam computed tomography (CBCT) revealed moderate to severe sinus mucosal swelling. Pharmacological treatment was extended for an additional 7 days to prevent complications. Symptoms gradually resolved, and no post-operative infections occurred. Follow-up CBCTs were obtained at final prosthesis insertion and thereafter.
Table 1.
Demographic information of the included patients
1. Case 1
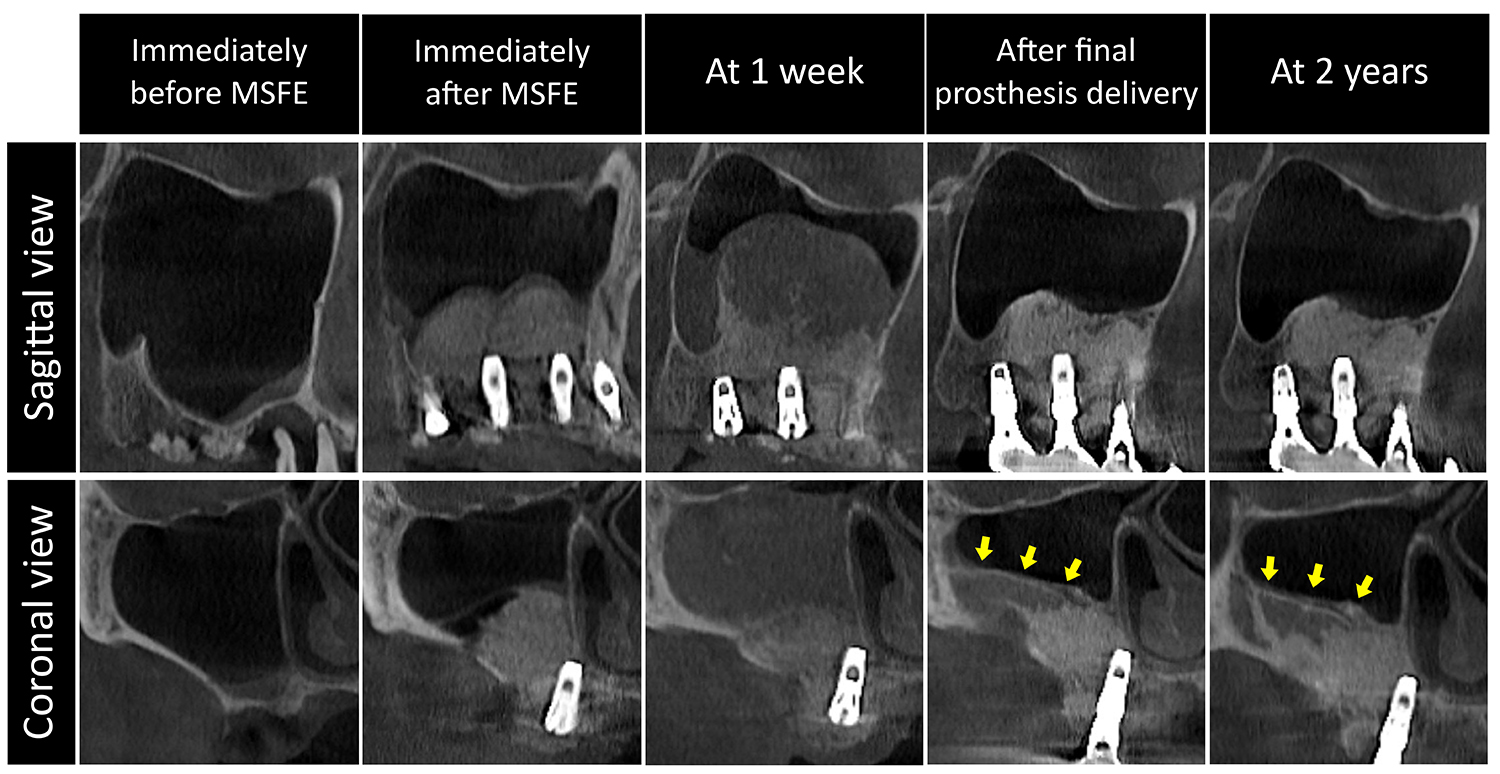
A 55-year-old female smoker underwent simultaneous lateral MSFE and implant placement in the right posterior maxilla. Residual bone height was 5 mm at #15, 2 mm at #16, and 3 mm at #17. After creating a lateral bony access window, xenogeneic bone substitute material was inserted, and three implants (Ø4.3 × 10 mm at all sites, Implantium; Dentium, Suwon, Korea) were placed.
Mild sinus membrane thickening was noted on pre-operative CBCT due to a periodontally compromised tooth at #15. After MSFE, the bone substitute material remained well confined without scattering or displacement. At 1 week, the patient presented with mild facial swelling, and CBCT revealed sinus mucosal swelling with dispersed graft particles within the sinus membrane boundary. The dispersion pattern was pointed coronally, and the ostium was not obstructed. At final prosthesis insertion (8 months), mucosal swelling had resolved, and the sinus membrane was positioned more apically compared to the 1-week scan. Newly formed bone was evident beyond the grafted area, particularly along the lateral sinus wall, as seen in coronal CBCT sections. At 2 years, further ossification with a distinct cortical layer was observed (Fig. 1).
2. Case 2
A 72-year-old non-smoking female required implant treatment in the left posterior maxilla. Residual bone height was 3 mm at #25, 1.5 mm at #26, and 4 mm at #27. Lateral MSFE was performed using a xenogeneic bone substitute. Staged implant placement was performed 6 months after MSFE (Ø4.3 × 10 mm at all sites, Implantium; Dentium).
Pre-operative CBCT showed no sinus pathology. After MSFE, a dome-shaped grafted area was observed. At 1 week, mild vestibular tenderness was noted, and CBCT revealed complete sinus opacification with graft particle dispersion. Some dispersed particles were not continuous with the original graft. Following prosthesis delivery, CBCT demonstrated distinct new bone formation along the lateral sinus wall. At 1 year, increased bone volume and density were observed, along with further maturation of spontaneously formed bone along the lateral wall and sinus floor (Fig. 2).
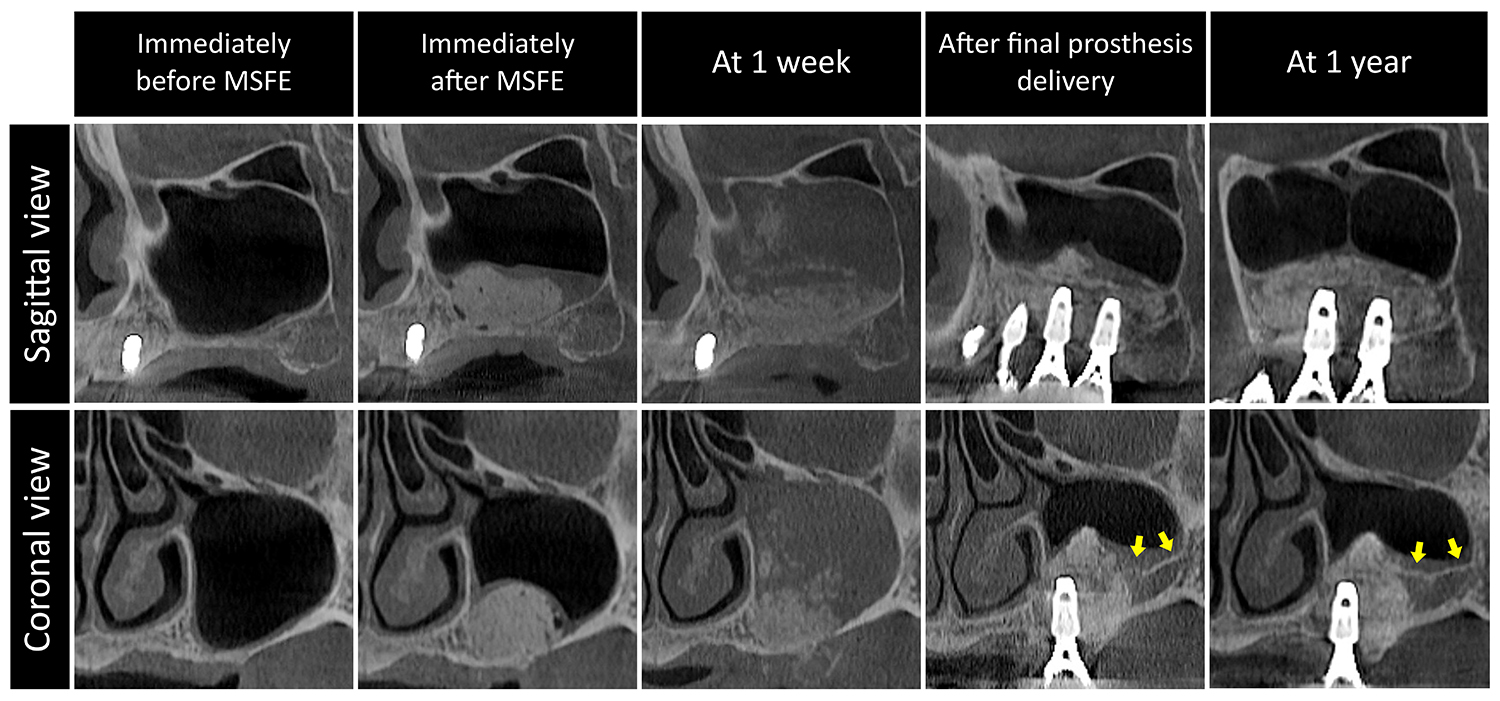
Fig. 2.
Case 2 involving a 72-year-old non-smoking female. Well-positioned bone graft particles were observed immediately after MSFE. At 1 week, sinus opacification and dispersion of bone graft particles were observed. At follow-up visits, SBF was detected beyond the bone-grafted area, with ostium patency. Yellow arrows indicate SBF beyond the bone-grafted area.
3. Case 3
A 49-year-old healthy, non-smoking male required implant treatment in the right posterior maxilla (residual bone height: 5 mm at #15, 2 mm at #16, and 3 mm at #17). Simultaneous lateral MSFE and implant placement (Ø4.3 × 10 mm at all sites, Implantium; Dentium) were performed.
Pre-operatively, mild sinus membrane thickening was observed at the mesial sinus area. After MSFE, the bone substitute was well positioned in a dome shape. At 1 week, the patient presented with mild facial swelling. CBCT showed near-complete sinus opacification with loss of graft integrity; the coronal portion appeared irregular. At final prosthesis insertion, CBCT demonstrated consolidation of dispersed graft material and bone formation along the buccal sinus wall, although still immature. At 1 year, marked ossification with cortical thickening was observed (Fig. 3).
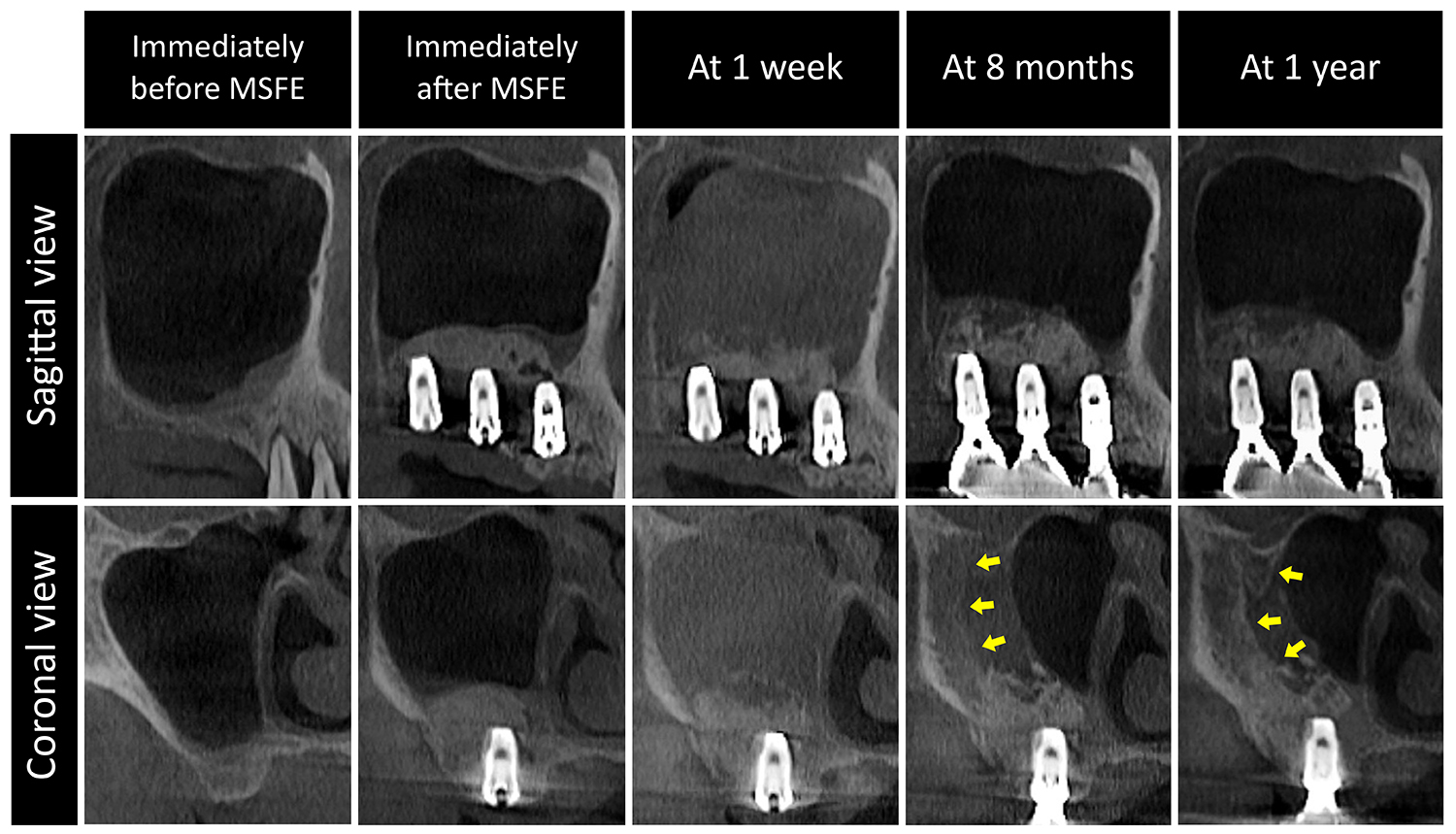
Fig. 3.
Case 3 involving a 49-year-old healthy, non-smoking male. Immediately after MSFE, well-contained bone graft particles were observed with some air bubbles. Sinus opacification and the dispersion of bone graft particles were observed 1 week post-MSFE. Marked SBF beyond the bone-grafted area was observed along the lateral wall at 8 months, and further bone maturation was observed at 1 year. Yellow arrows indicate SBF beyond the bone-grafted area.
4. Case 4
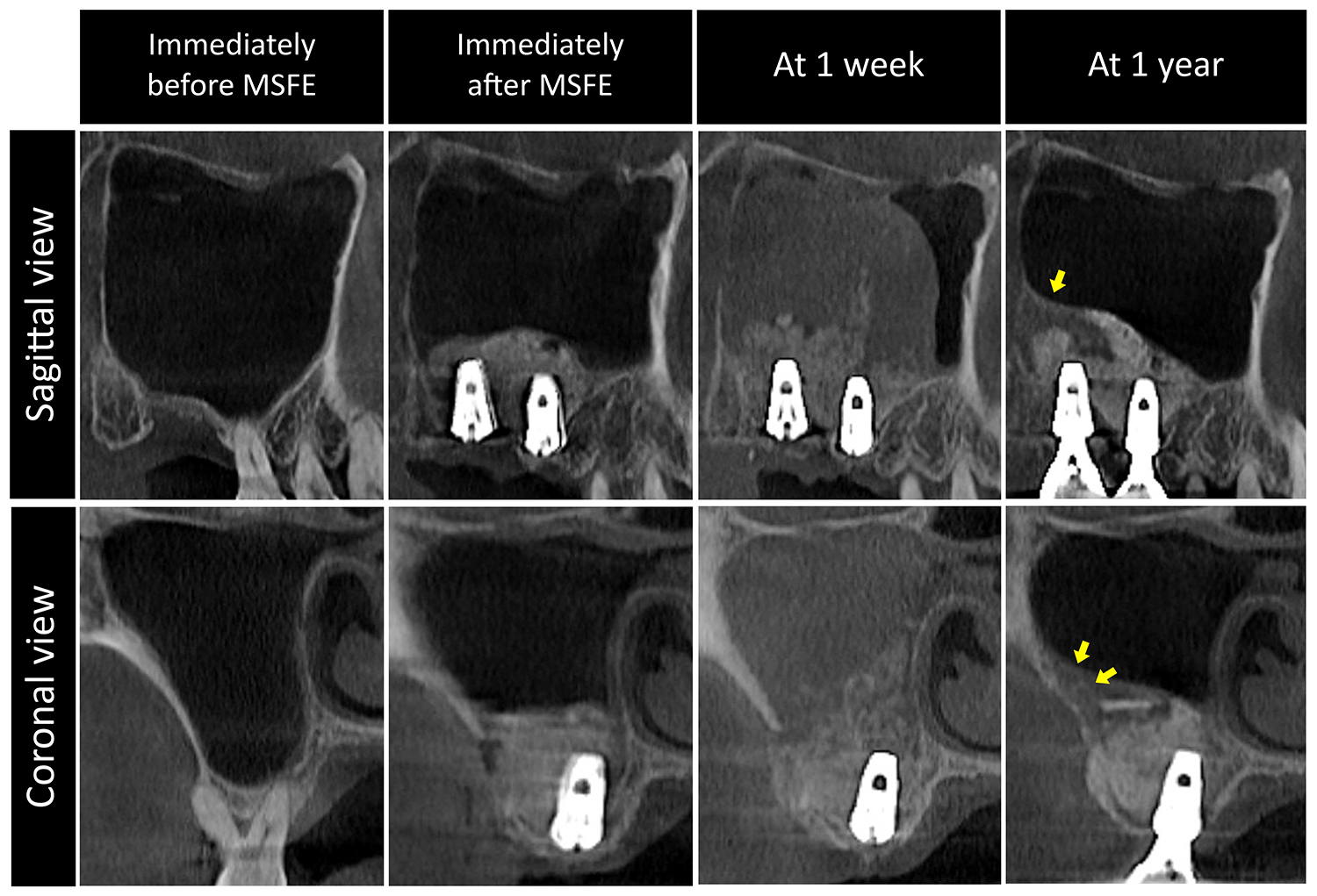
A 72-year-old non-smoking female sought implant treatment in the right posterior maxilla (residual bone height: 4 mm at #16 and 3 mm at #17). Simultaneous lateral MSFE and implant placement (Ø4.8 × 10 mm at #16 and Ø6.0 × 10 mm at #17, Implantium; Dentium) were performed.
Pre-operatively, the sinus was healthy, with no mucosal thickening. Immediate post-MSFE CBCT showed well-confined graft material without signs of sinus membrane perforation. At 1 week, the patient reported mild discomfort around the surgical site. CBCT revealed marked sinus mucosal swelling and graft particle dispersion, particularly medially. At final prosthesis insertion, the pattern of dispersed graft material had changed, and new bone formation was observed along the lateral sinus wall and distal sinus area (Fig. 4).
Ⅲ. Discussion
The present cases demonstrated unexpected SBF beyond the boundary of the grafted bone. This finding may have limited relevance to implant placement, as the grafted bone was sufficient to support implants of adequate length (≥ 8–10 mm). However, the phenomenon is worth reporting to better understand the osteogenic potential of the maxillary sinus.
The maxillary sinus is a closed cavity bounded by multiple bone walls and the sinus membrane, allowing graft material beneath the elevated membrane to contact these structures after MSFE. Moreover, a blood clot integrated with the graft material can be readily stabilized within this space. The adjacent bone walls provide the primary source of ossification, while the sinus membrane also contributes to bone formation.13 Thus, the maxillary sinus can be regarded as a favorable and predictable environment for bone regeneration.
Occasionally, the space beneath the elevated sinus membrane may expand beyond the grafted area owing to post-operative bleeding or transient mucosal thickening.14,15 CBCT findings at 1 week in the present cases support this possibility. A study by Quirynen et al. also reported significant sinus membrane swelling at 1 week after MSFE.16 At this stage, the sinus membrane outline was markedly expanded compared to immediately after MSFE, without clinical evidence of perforation or infection, although varying degrees of graft particle dispersion were observed. Over time, the elevated membrane settled downward, but part of the newly created space appeared to persist. Although not fully explainable, it may be conjectured that the osteogenic potential of adjacent bone walls and the sinus membrane influenced this space, leading to additional bone formation beyond the grafted boundary.
A similar phenomenon has been reported in preclinical and clinical studies. In a rabbit sinus model, hydraulic pressure was used to detach the sinus membrane from the bone walls.17 Micro-computed tomography revealed new bone formation beyond the grafted area. The authors suggested that hydraulic pressure extended beyond the osteotomy site, causing excessive membrane elevation and space formation outside the grafted region, which was subsequently filled with new bone.
Several case reports have described SBF, including cases involving removal of a displaced implant, an impacted premolar, and an intrasinus cyst.10,11,12 A common feature was the unintentional creation of space after removal of a pathological object or lesion, or following extraction. These spaces were left ungrafted and allowed to heal naturally. After 3 to 5 months, they were filled with new bone, and in some cases, sinus augmentation was unnecessary for implant placement. Consistent with these findings, some clinicians have advocated graft-less MSFE using blood clot stabilization without bone substitutes.2,18
In the present cases, undetected sinus membrane perforation cannot be excluded. Dispersed graft particles may serve as indirect evidence, despite the absence of clinical symptoms or endoscopic confirmation. Some particles may have been extruded through the ostium, after which the perforation healed uneventfully without infection.19 A recent case report described sequential radiographic changes after MSFE, showing that despite graft dispersion and sinus opacification, the sinus eventually returned to a healthy state or only minor mucosal thickening, indicating spontaneous resolution.20 However, no SBF was observed in that study, and the membrane ultimately covered the grafted bone. Nonetheless, an atypical healing sequence following membrane perforation cannot be ruled out, as a healed membrane may create additional space beneath it.
It is also possible that space was elevated but not grafted. In such cases, SBF may in areas where bone graft material was not initially placed, following the resolution of transient mucosal swelling.
Ⅳ. Conclusion
In the present cases, unexpected SBF was observed beyond the grafted area. Although the mechanism remains unclear, factors such as post-operative bleeding, transient mucosal thickening, and healing after membrane perforation may be involved. While the clinical significance for implant placement is limited, these findings suggest that space formation itself promotes endo-sinus bone formation due to the influence of adjacent bone walls and the sinus membrane.
