

Ⅰ. Introduction
Dental implants have emerged as an effective treatment modality for oral rehabilitation of partially or fully edentulous dentition.1 Long-term clinical studies have shown that dental implant survival and success rates are as high as 95%.2
Despite high implant success rates, implant failures do occur. They are broadly classified into early and late failures. Early failure involves failure of integration between the fixture and bone. It mainly occurs due to poor bone quantity, quality, and lack of primary stability. Late failure is the loss of integration between the fixture and bone and mainly occurs due to peri-implantitis.
To remove failed dental implant fixtures, many methods have been introduced by dentists. Failed implants need to be explanted, and over the years a number of techniques have been proposed by dentists, including the use of bur-forceps, trephine drills, high torque wrenches, bone chisels, and peizosurgery.3 Despite being effective, these techniques, except the method of using reverse torque, may damage the surrounding bone, leading to significant morbidity at the surgical site. This can further worsen the chances of placement of a new implant at the explantation site because of the large defect. Thus, less invasive methods are needed for removal of failed implants.
The use of a monopolar electrocautery unit to remove failed dental implants has been introduced.4 The unit causes thermo-necrosis of the surrounding bone and weakening of the bone-implant interface. In our study, we aimed to determine the correlation between monopolar electrocautery settings and reduction of reverse torque in removing of dental implants. Manipulated monopolar electrocautery settings include power of the electrocautery unit and adapted time. The goal of this experiment was to establish a protocol for electrocautery settings when removing dental implants.
Ⅱ. Materials and Methods
The study was conducted on fresh pork ribs. A total of 45 dental implant fixtures were placed into pork rib bones, individually, prior to the experiment. The implant system Dentium (Dentium Comp., Ltd. Gyeonggi-do, Korea), with an Elcomed implant engine (W&H Dentalwerk; Bürmoos, Austria), was used. The Elcomed implant engine can record the torque of the hand piece continuously, and the results can be exported via USB.
Implantium implants sized Ø4.5 × 10 mm were used. They (n = 45) were categorized into three groups according to monopolar electric cautery power (coagulation mode) and adapted time: 30 watt and 20 second (n = 15), 40 watt and 40 second (n = 15), and control group (n = 15). The torque in the removal of the implant fixture, after monopolar electro cauterization directly inside the implant fixture, was also measured.
In the experiment groups, after applying the monopolar electrocautery tip directly to the internal surface of the dental implant according to electrocautery settings, the dental implants were removed. In the control group, the dental implants were removed without applying the electrocautery unit, immediately after insertion of the implant fixture.
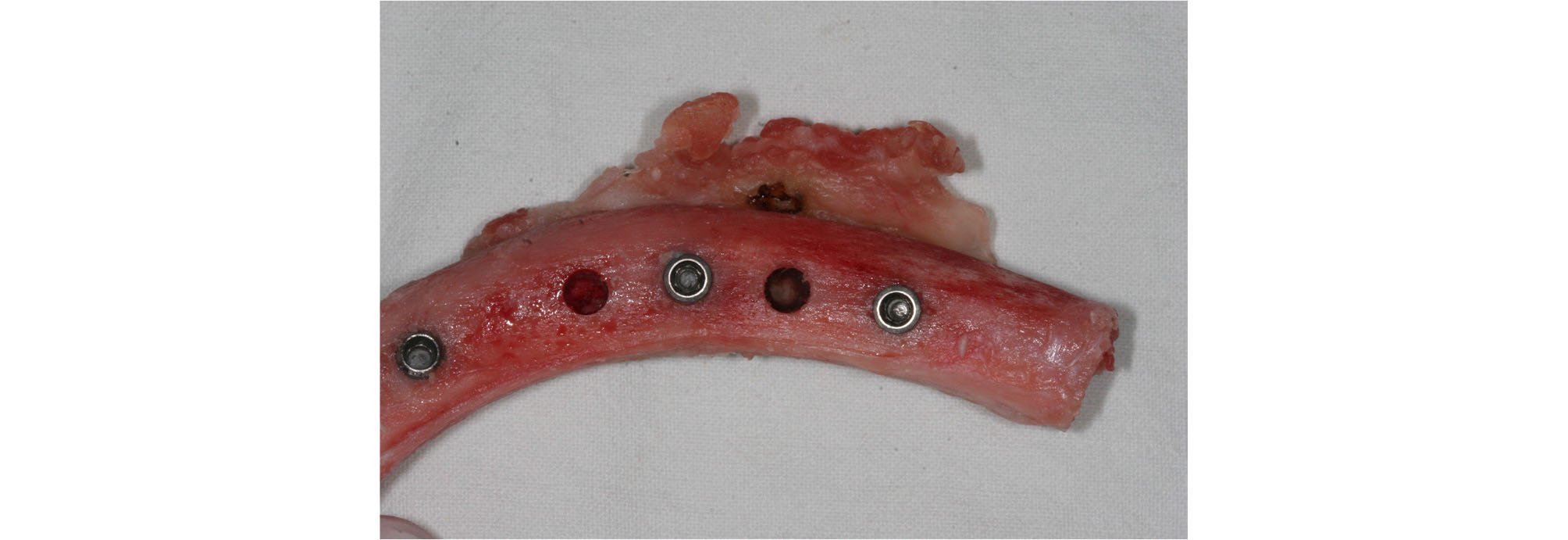
The experimental procedures were as follows. After reflecting the periosteum of the pork rib with a periosteal elevator, the bone was exposed, and implant sites were prepared following the drill sequence and under normal saline solution irrigation. The drilling speed was constant at 1000 rpm for all three groups. After sequential drilling, the dental implants were placed using the standard protocol for Implantium implants sized Ø4.5 × 10 mm. All fixtures were placed and insertion of the implant fixtures stopped, at a constant torque of 40 N·m (Fig. 1). Primary stability of all inserted implant fixtures was confirmed at a constant torque of 40 N·m by the settings of the drilling machine.
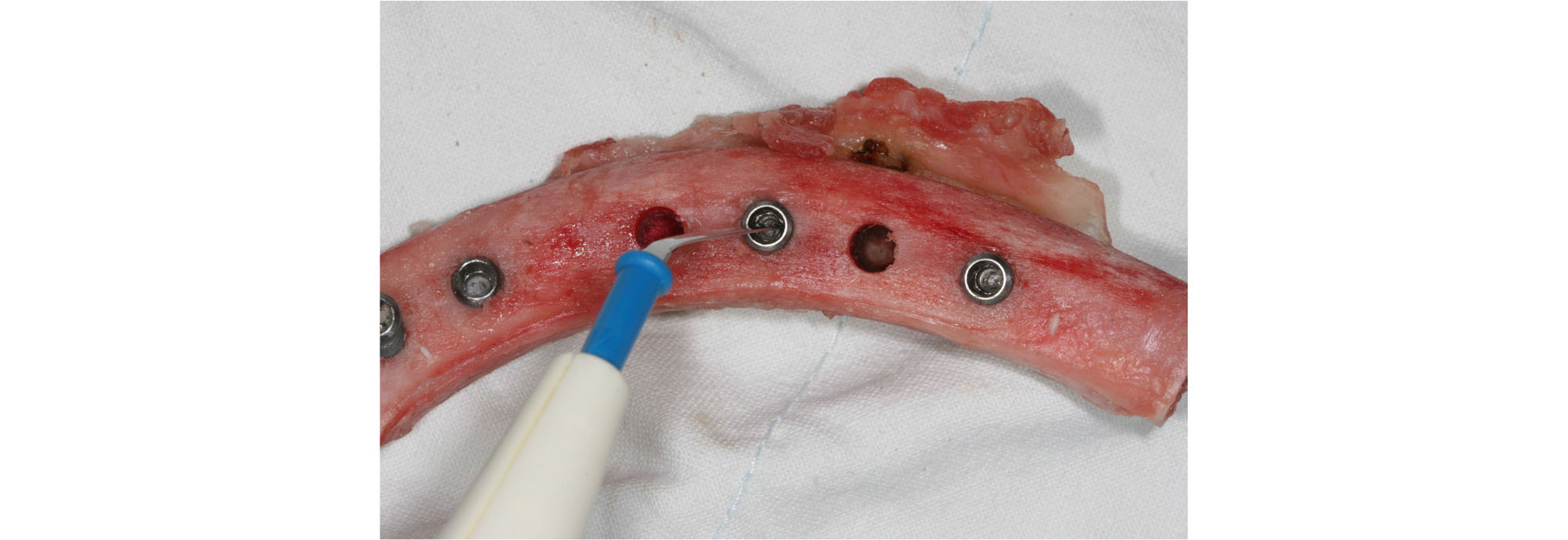
After confirming the primary stability of the implants, the monopolar electrocautery unit was directly applied to the internal surface of the dental implant to cause thermo-necrosis at the bone-implant interface (Fig. 2). The two experimental groups, according to monopolar electric cautery power (coagulation mode) and adapted time, were 30 watt and 20 second (n = 15), and 40 watt and 40 second (n = 15). The control group removed the dental implants without applying the electrocautery unit.
After applying the electrocautery unit to the dental implants, they were explanted by the reverse torque technique, using a rotary instrument (Elcomed implant engine; W&H Dentalwerk; Bürmoos, Austria). Torque during explantation was continuously monitored and recorded by the machine. Torque during the removal of the implant fixtures was exported and recorded.
Descriptive statistics were used to determine the effectiveness of electrocautery on implant fixture extraction. The three groups were analyzed separately. All statistical analyses were performed in SPSS v. 23 (IBM Corp., Armonk, NY, USA). Significance was set at p ≤ 0.05. Differences in torque for the removal of the implant fixtures between the groups were compared using ANOVA.
Ⅲ. Results
The torque [unit; N·mm] (mean ± SD) during removal of the dental implant fixtures with the Elcomed implant engine, after monopolar electrocauterization directly inside the implant fixture, was 296 ± 98.5 in the 30 watt and 20 second group and 184 ± 65.9 in the 40 watt and 40 second group (Table 1).
Table 1. Torque in removal of implant fixture after monopolar electrocauterization directly inside the implant fixture
Turkey HSD p-value calculated by post hoc test with Tukey's HSD (honestly significant difference) method
The torque of removal of the dental implant fixtures was 279 ± 121 (mean ± SD) N·mm in the control group. The mean torque (N·mm) was significantly lower in the 40 watt and 40 second group than that in the other groups (p = 0.006). The mean torque was significantly lower in the 40 watt and 40 second group than that in the 30 watt and 20 second group (p = 0.009).
Although thermo-necrosis of the bone was observed in the 30 watt and 20 second group (Fig. 3), the difference in the mean torque between the 30 watt and 20 second group and the control group was not statistically significant (p = 0.884). Definite thermo-necrosis of the bone was observed in the 40 watt and 40 second group (Fig. 4).


Ⅳ. Discussion
Dental implants have emerged as an effective treatment modality for oral rehabilitation of partial or full edentulous dentition. Although implant success rates are high, cases of implant failure are encountered. To eliminate failed dental implant cases, we introduce a technique of using a monopolar electrocautery unit to extract implant fixtures and suggest a protocol of settings for the electrocautery unit.
The experimental group was divided into three groups. The electrocautery unit was used in 2 of the groups. The purpose was to find the standard electrocautery settings for power in watts and time in seconds. The mean torque at removal of the implant fixture immediately after implantation was significantly lower in the 40 watt and 40 second group than that in the other two groups. Although thermo-necrosis of the bone was observed in the 30 watt and 20 second group, the difference in the mean torque between the 30 watt and 20 second group and the control group was not statistically significant. This means that the torque required for removal of the implant fixtures was reduced in electrocautery with settings of 40 watts and 40 seconds, when extracting the implant fixtures immediately after insertion.
This method employed the principle of thermo-necrosis of the surrounding bone and weakening of the bone-implant interface. This implant explantation method, using electrocautery, causes thermo-necrosis of the surrounding bone and weakens the bone-implant interface, which can further lead to delayed wound healing and wide osteonecrosis. This acts as an obstacle for the placement of a new implants and extra bone grafts may be needed. According to a study by Eriksson and Albrektsson (1983) bone is susceptible to thermal damage above 47°C5 . Heat stress at this temperature for more than 1 minute can lead to greater injuries. Surgeon must consider the cumulative temperature gain at the bone surround implant fixture, and heat stress above 47°C when using electrocautery on the implant fixture. Therefore, research for removal of implants, using electrocautery with minimal thermal injury, is needed. Removal of failed implants with electrocautery may be considered for minimal mechanical bone destruction and in cases of inability to remove the failed implant fixture using a manual wrench.
Failed implants need to be explanted, and over the years a number of techniques to eliminate failed dental implant fixtures have been proposed, including the use of bur-forceps, trephine drills, high toque wrenches, bone chisels, and peizosurgery.3 Despite being effective, these techniques may damage the surrounding bone, leading to significant morbidity at the surgical site. This could further worsen the chances of placement of a new implant at the explantation site due to a large defect. Thus, less invasive methods are needed for the explantation of failed implants. Furthermore, various methods of removal of failed dental implants in the osseointegrated fixture would be evaluated within each other in the point of the surround bone damage. However, electrocautery may also have a risk for thermal injury to the bone surrounding the implant fixture. Failed or poorly placed dental implants have to be explanted.6 If the implant that requires explantation does not show mobility, removal becomes challenging. Especially electrocautery method may be more effective compared to high torque wrench method, in that the removal kit from implant companies can be broken during removal of implant fixture due to high torque.
Implant explantation, using an electrocautery unit, is easy to perform and less invasive compared to other methods. However, this method poses risks of injury to dental pulp and bone necrosis surround implant fixture. Clinicians should be careful not to touch other teeth or restorations with the electrocautery unit because this can lead to pulp necrosis of teeth or implant failures, especially when the residual bone is thin. According to a study by Krejci et al. (1982) direct contact of the electrocautery unit with class V amalgam restorations for more than 0.4 seconds can lead to pulp necrosis in dogs.7 Another study by Zach and Cohen (1965) on monkeys, reported that increase in the pulp temperature by 5.5°C can led to pulp necrosis or pulpitis in 15% of cases.8 Furthermore, in a preliminary study on thermal injury thresholds in human teeth, the main cause of thermal-necrosis of the pulp was found to be dentin injury.9
Implant failure mainly occurs due to peri-implantitis and lack of osseointegration.10 Peri-implantitis is the inflammation of the surrounding tissues of osseointegrated implants, which is usually accompanied with bone loss and bleeding on probing.11 The success of dental implants was evaluated based on immobility and peri-implant radiolucency. However, dentists consider the gingival biotypes, width of the attached gingiva, width of the implant, and smoking history when evaluating the success rates.12 Osseointegration involves direct bone-to-metal anchorage without interposition of non-bone tissue. Titanium dental implants should be bonded to living bone without fibrous tissue interruption, so that they cannot be separated without fracture.13 Various factors influence osseointegration, such as excessive implant mobility, micromotion, excessive thermal damage by drilling, and patients’ medical history of osteoporosis, diabetes mellitus, old age, nutritional deficiency, or smoking.14 Electrocautery may affect the tissues surrounding the failed implant fixture. Surgeon should consider the above factors associated with implant failure.
In our study, we used a monopolar electrocautery unit and applied it to the internal surface of the implant fixture right after placement of the implant. Thus, secondary stability could not be measured, and the thermo-necrosis broke only the mechanical engagement between the implant and surrounding bone.15 However, electrocautery units can be used to break down the osseointegration in failed dental implants. In a study by Joanne Cunliffe and Barclay (2011) after reflecting the mucoperiosteal flap and identifying the failed dental implant, an electrocautery unit was applied to the internal surface of the neck of the implant to cause thermo-necrosis.4 After one week, the patient returned and the mucoperiosteal flap was reflected again. The implant was easily removed with the use of a hand wrench with torque less than 30 N. Further study for evaluation of the current protocol is needed in removing of the implant fixture which is osseointegrated to the surround bone.
Monopolar electrocautery units are the most commonly used electrocautery instruments because of their versatility and effectiveness. The active electrode is placed at the surgical site and can be used to cut tissue and coagulate bleeding tissues. The second electrode (return electrode) pad is attached to remote sites such as the legs, so the electrical current flows from the generator to the electrode through the target tissue, and then to the patient return pad and back to the generator. Wilcox et al. (2001) measured local heat effects created by the use of an unipolar electrosurgical unit, a bipolar electrosurgical unit, and a neodymium:yttrium-aluminumgarnet (Nd:YAG) laser, in the presence of metallic implants.16 They found that there was a higher potential for thermal damage to the surrounding bone when using a monopolar electrosurgical unit than when using a bipolar electrosurgical unit or Nd:YAG laser because the cumulative temperature gains exceeded more than 10°C (the theoretical limit). Further clinical studies are warranted for incorporating these electrosurgical units in dental practice.
V. Conclusion
Monopolar electrocautery can be considered as an alternative method for the removal of failed or poorly positioned dental implants without the grinding of the bony tissue surrounding the implant fixture. Further clinical studies should be conducted to validate our study findings. Delayed removal of implant fixtures after electrocauterization, considering the biological responses and the minimum energy settings for the electrocauterization, should be validated for the standards of removing implant fixtures using electrocautery.
