

Ⅰ. Introduction
Buccal bone resorption can pose challenges such as dehiscence or fenestration when preparing for implant placement. Narrow ridges can cause these defects, threatening the long-term stability and survival of dental implants.1
Immediate implant placement in the presence of buccal dehiscence or fenestration results in poor outcomes. Therefore, clinicians should prioritize early or delayed implant placement or ridge reconstruction to preserve alveolar bone and enhance implantation.2
Alveolar ridge preservation (ARP) is aimed at bone regeneration following tooth extraction3 even in compromised extraction sockets.4 ARP and delayed implant placement may be the preferred methods for poor alveolar ridge conditions as they can shorten the rehabilitation period by preventing additional bone resorption, which usually occurs in the first 6 months following tooth extraction.3
This case report describes an ARP method using a combination of xenografts and resorbable membranes, which facilitated successful implant placement under normal conditions.
Ⅱ. Case Report
A 70-year-old male patient visited Seoul National University Dental Hospital in December 2021, with a complaint of severe anterior maxillary tooth mobility and requested extraction and implant placement. Clinical examination revealed Class III mobility according to the Miller classification, and panoramic and apical radiographs revealed severe bone loss around the maxillary right central (#11), lateral (#12), and left lateral (#22) incisors. This severe horizontal bone loss likely exposed more than half of the implant ’s diameter following its placement. Because the patient desired a fixed prosthesis, implant placement following ARP was planned.
1. Surgical procedures
The patient either gargled with 0.12% chlorhexidine gluconate solution for 30 s or his mouth was disinfected with a povidone-iodine ball before each surgery. The skin around the surgical site was disinfected with a chlorhexidine ball, and a sterile surgical drape was applied to prevent potential contamination from extraoral sources.
After tooth extraction, a full-thickness flap was elevated (Fig. 1A) using a crestal incision between #12 and #22. A partial-thickness flap was elevated till the lower part of the mucogingival junction for primary tension-free closure. Collagenated bovine bone mineral (CBBM; Bio-Oss® Collagen, Geistlich Pharma AG, Wolhusen, Switzerland) was used for bone grafting at the extraction socket and buccal area, and non-crosslinked collagen membrane (NCLM; Bio-Gide, Geistlich Pharma AG, Wolhusen, Switzerland) was used and trimmed to provide graft volume (Fig. 1B).
A holding suture of 5/0 Vicryl rapideTM (Johnson & Johnson Medtech, New Jersey, USA) was employed to fix the NCLM (Fig. 1C), and the flap was moved and pulled towards the occlusal surface to achieve tension-free primary closure. The underlying NCLM was fixed with Hidden X suture5 using a 5/0 Vicryl rapideTM, and the buccal and palatal flap were everted and sutured with a single interrupted suture using a 5/0 Monosyn® (B.Braun, Melsungen, Germany) (Fig. 1D).
Postoperative drugs were prescribed, including cefdinir (100 mg, three times a day for 5 days) to prevent postoperative infection, prednisolone (5 mg, three times a day for 3 days) to prevent postoperative edema, and 0.12% chlorhexidine gluconate mouth rinse to prevent plaque formation in the surgical and proximal areas until the sutures were removed. The patient showed no symptoms of edema or infection, and all the sutures were removed after 2 weeks. The patient was referred to the prosthetics department for the fabrication of a removable partial denture in the surgical area 2 months after surgery (Fig. 1E to 1G).
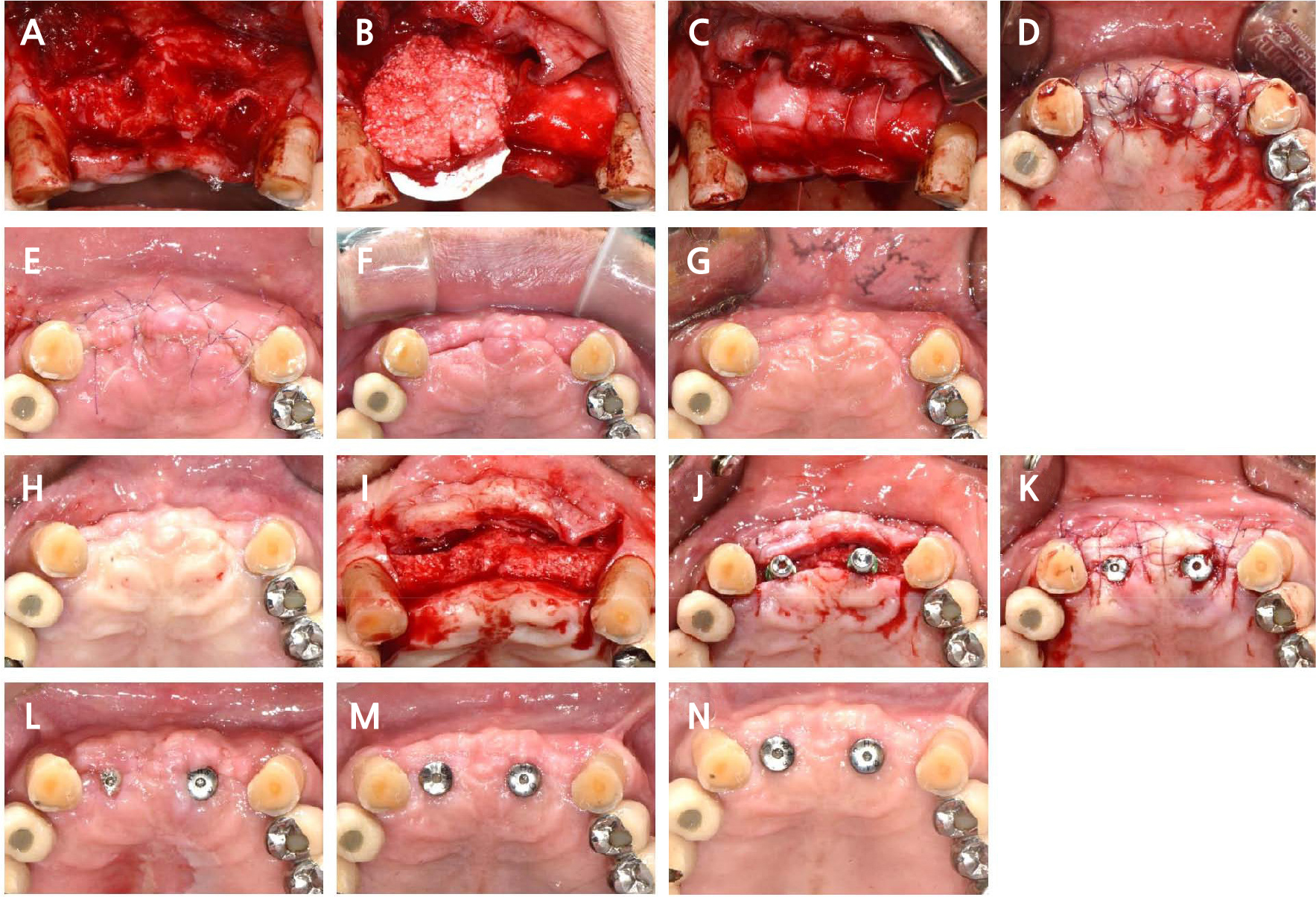
Fig. 1.
Occlusal view of the anterior maxillary area following the surgical procedure and follow-up. (A) After extraction of the anterior maxillary teeth, a flap is elevated, (B) The collagen membrane is fixed on the palatal side and deproteinized bovine bone mineral (DBBM) is placed, (C) The collagen membrane is fixed with a holding suture, (D) The buccal and palatal flaps are closed using a hidden X suture and a single interrupted suture, (E) Occlusal view of the surgical sites 1 week postoperatively, (F) Occlusal view of the surgical sites 1 month postoperatively, (G) Occlusal view of the surgical sites 4 months postoperatively, (H) Occlusal view of the surgical sites before implant placement (almost 9 months after extraction), (I) Bone regeneration is observed upon flap elevation. Note the incorporation of the collagenated bovine bone mineral (CBBM) into the newly augmented bone, (J) The implants are placed after the osteotomies. Occlusal view of implant placement, (K) The buccal and palatal flaps are closed, (L) Occlusal view of the surgical sites 10 days postoperatively, (M) Occlusal view of the surgical sites 1 month postoperatively, (N) Occlusal view of the surgical sites 2.5 months postoperatively.
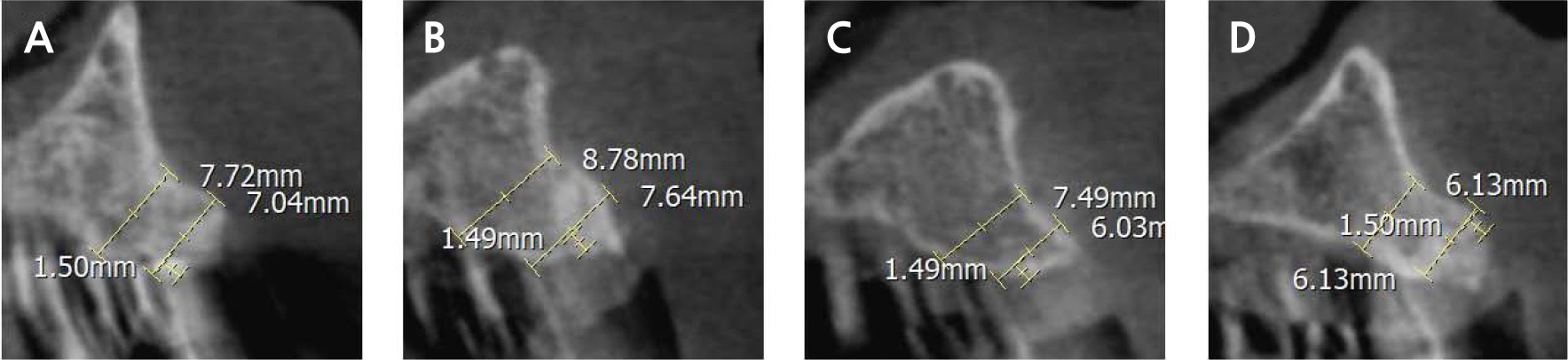
After 8 months of uneventful healing (Fig. 1H), cone-beam computed tomography (CBCT) confirmed that the bucco-palatal width was at least 6 mm (Fig. 2), allowing the placement of a 4 mm diameter implant. A full-thickness flap was raised in the anterior maxillary teeth region, and the bone was augmented under the healthy periosteal and soft tissues (Fig. 1I).
Internal-type implants (Osstem TSIII, Osstem, Seoul, Korea) with a diameter of 4 mm and height of 10 mm were placed at sites #12 and #21 according to the manufacturer's protocol (Fig. 1J). The implants exhibited stability of 30 N, which allowed for a one-stage procedure. Healing abutments measuring 4.0 × 5.0 mm and 4.5 × 5.0 mm were attached to the #12 and #21 implants, respectively (Fig. 1K). To prevent infection and inflammation, the patient was prescribed accordingly (as mentioned previously).
The patient did not show any signs of edema or infection, and all the sutures were removed ten days after surgery (Fig. 1L). The implants were successfully restored using an implant-supported zirconia bridge. The patient reported no adverse reactions, such as foreign body reaction, pain, or abnormal sensory responses (Fig. 1M to 1N).
During the intraoral clinical examination, healthy peri-implant mucosa was observed, and no signs of inflammation, such as suppuration, edema, or rash, were observed. The radiograph obtained after connecting the final prosthesis revealed that the implant was located approximately 1–2 mm from the alveolar bone, and no bone loss was observed (Fig. 3). The patient was satisfied with the implant restoration.
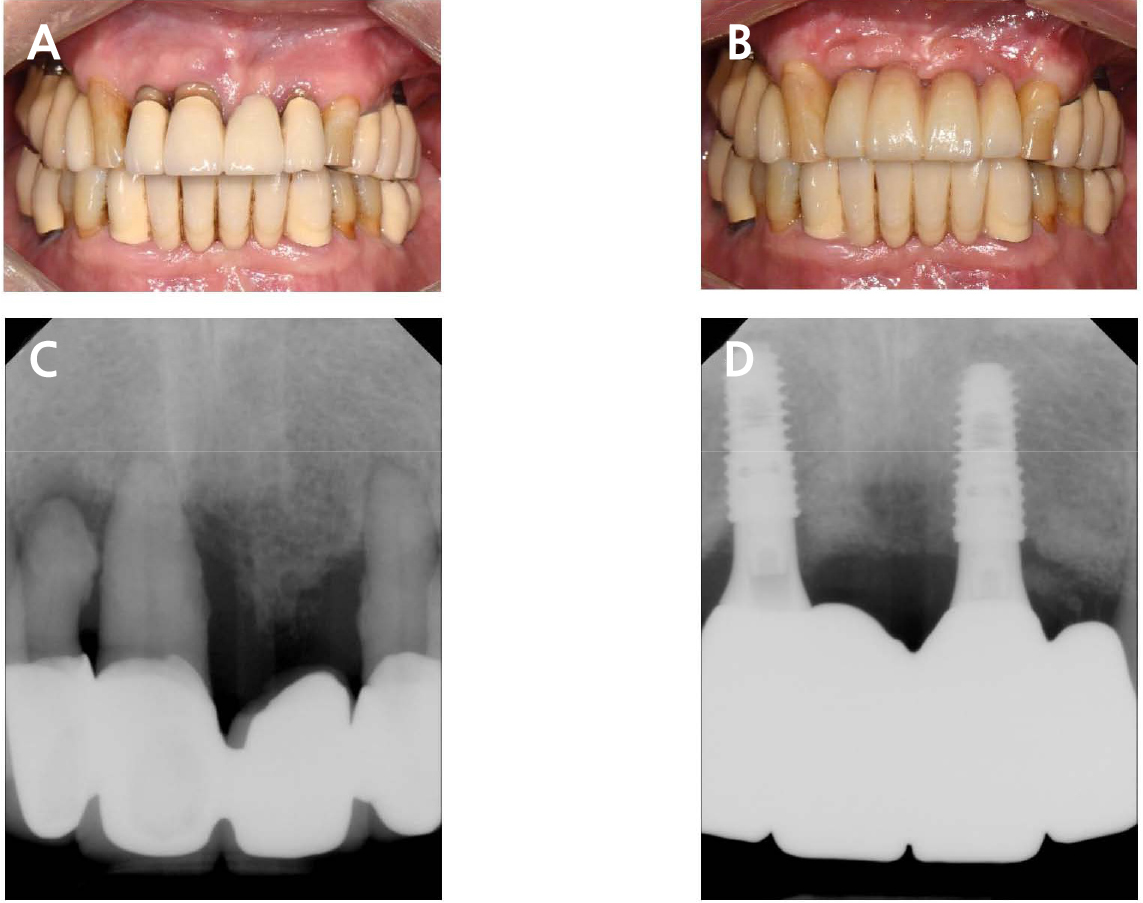
Fig. 3.
Pre- and postoperative buccal views and periapical radiographs of the anterior maxillary area. (A) Preoperative buccal view of the anterior maxillary area, (B) Postoperative buccal view of the anterior maxillary area, (C) Preoperative periapical radiographs of the anterior maxillary area, (D) Postoperative periapical radiographs of the anterior maxillary area.
Ⅲ. Discussion
According to a systematic review,6 this case involved a Class IV defect with reduced ridge width, threatening primary stability when the implant was placed in the correct position prosthetically. In such cases, a staged approach for bone regeneration and implant placement involving the use of autologous bone blocks (either alone or in combination with bone substitutes and/or collagen membranes) prior to implant placement is often preferred.6 This approach has been reported to be reliable and successful for the treatment of large bone defects.7 This procedure, known as ARP, involves the application of a bone graft material and a membrane immediately after tooth extraction. However, the absorbable membrane used in this procedure rapidly degrades when exposed to the oral cavity. Therefore, to maximize the lifespan of the absorbable membrane, a primary closure should be performed, similar to a guided bone regeneration procedure.
The bone regeneration area, along with the surrounding pristine bone, exhibited radiopacity on CBCT imaging. Furthermore, the regenerated bone area demonstrated hardness similar to that of the adjacent pristine bone. In addition, implant placement was feasible at #12–22 sites, as they exhibited adequate bucco-palatal widths (Fi. 2). However, caution was exercised to ensure the exclusion of the proximity to the nasopalatine canal in the case of #11 site and proximity to the tilted #23 implant in the case of #22 site.
According to a recent review on bone augmentation,8 no disparity exists in the survival rate of implants when using bone grafts or autologous bone blocks. Moreover, successful cases of ridge augmentation using deproteinized bovine bone mineral (DBBM) and collagen membranes, as used in this case for esthetic implant placement in the anterior maxilla, have been reported in the literature.9
Research on the use of DBBM without autologous bone has shown that bone augmentation procedures typically require a healing period of 7–10 months based on clinical and histological studies.9,10 In this study, the duration between augmentation and implant placement ranged from 9 to 10 months. In the present case, the extent of the buccal bone loss necessitated an approach that ensured bone augmentation rather than ARP. A healing period of 9–10 months was selected for the current case based on a previous study9 that used the same type of collagen membrane and DBBM.
Two categories of membranes are used for bone regeneration: nonabsorbable and absorbable membranes. Among these, nonabsorbable membranes pose a common complication known as postoperative exposure.11 Exposure of the membrane significantly increases the risk of infection and jeopardizes bone formation.12
Collagen membranes, which offer several advantages, such as promoting hemostasis,13 chemotaxis of gingival fibroblasts,14 and ease of handling,15 are widely utilized in bone regeneration. A systematic review16 comparing the clinical outcomes of two types of resorbable collagen membranes revealed that in the majority of studies, bone augmentation results were comparable between non-crosslinked and crosslinked membranes during–4–6 months of reentry surgery. However, crosslinked membranes are more likely to be exposed to the membrane. In the current study, a non-crosslinked collagen membrane was chosen to minimize the risk of membrane exposure, as it could potentially impact the process of bone regeneration. In this case, no exposure to the NCLM was observed.
There is an ongoing debate regarding the optimal timing for bone augmentation, and the decision is based on various factors, such as the patient's specific characteristics and the nature of the lesion.3 Ultimately, dental professionals should carefully evaluate the advantages and disadvantages of this procedure at different time points during the treatment plan. By adopting a patient-centered approach and tailoring the timing of bone augmentation according to each patient's specific needs and circumstances, dental professionals can ensure the best possible outcomes and optimal long-term dental health.
This case had several limitations, including long clinical crowns, loss of the interdental papilla at the midline, and poor pink esthetics. To address these concerns, it is crucial to maintain an appropriate distance between the contact point of the prosthesis and the bone crest.17 This allows for a potential rebound of the interdental papilla. Soft tissue augmentation18 and replicating the shape of the gums in a prosthesis19 are also viable considerations for enhancing the overall outcomes. These measures can contribute to improving esthetics and achieving satisfactory results in terms of both form and function.
