

I. Introduction
Limited vertical bone height associated with sinus pneumatization and ridge resorption might be the critical factor to be considered in the placement of dental implants at atrophied posterior maxilla. There have been several surgical approaches to overcome this clinical issue and sinus floor elevation (SFE) has been proven to be a reliable method to show predictable survival rate of implants installed with both lateral and transalveolar approach1-3.
Lateral approach first introduced by Boyne in 1969 utilized surgical opening at the lateral wall of the maxillary sinus to have good visual and instrumental access during SFE. However, patient morbidity resulting from bleeding and postoperative swelling
and membrane perforation during the surgery have been the common complications of lateral SFE4. On the other hand, transalveolar approach (Summer’s technique) is a more conservative method as the access to the sinus membrane was prepared within the size of implant diameter to be installed and the extent of elevation was limitedly done around the apex of implant5. Theoretical ideas of the sinus elevation through the crestal access could be explained with hydraulic pressure exerted on the plug comprised of bone chips and blood trapped within6. By pushing up the plug with osteotomes, detachment and ballooning of the sinus membrane appeared in a hemisphere shape.
In conventional Summers’ technique, the access to the sinus cavity was prepared by the upfracture of the sinus floor using osteotomes, in which the malleting of the patients might cause trauma to the inner ear and vertigo7. In addition, unexpected and undetectable perforation of the membrane could occur as the surgery has been done in a blind way and dependent on the surgeon’s experience. Although, the perforation seemed rarely be involved with the failure of implants according to the clinical reviews8, there remains the possibility of loss and infection of the bone graft materials due to the disintegration of the sinus membrane.
There have been innovative surgical tools including specially designed reamers, drills and piezoelectric devices to minimize the trauma while cutting the sinus floor and decrease patient’s discomfort with avoidance in malleting. A modified lateral approach, so called hybrid technique, introduced by Jung et al. is one of the surgical skills for noninvasive and safer elevation, which utilized a linear shaped osteotomy at the lateral wall combined with transalveolar approach9. In brief description of the surgical procedures, a full thickness flap with horizontal and vertical releasing incision was designed and osteotomy at the lateral wall was positioned coronally just above the lower border of sinus floor and ran parallel along the floor. Mesiodistal length was extended to include the installation site planned and apicocoronal dimension was minimized about 3~5 mm just to insert the sinus elevator. Detachment of the sinus membrane was limited in the lining of the internal surface of the floor around the future installation site and a sequential drilling was done in full length of remaining bone height (RBH) to penetrate the floor. While drilling, sinus elevator was inserted through the lateral osteotomy site to protect the membrane. Graft materials were plugged into the drilled passage to elevate and augment the sinus floor with hydraulic pressure and implants were placed.
In the present report, two cases of implant placement using hybrid technique were described and the clinical and radiographic outcomes were discussed.
II. Case reports
1. Case 1
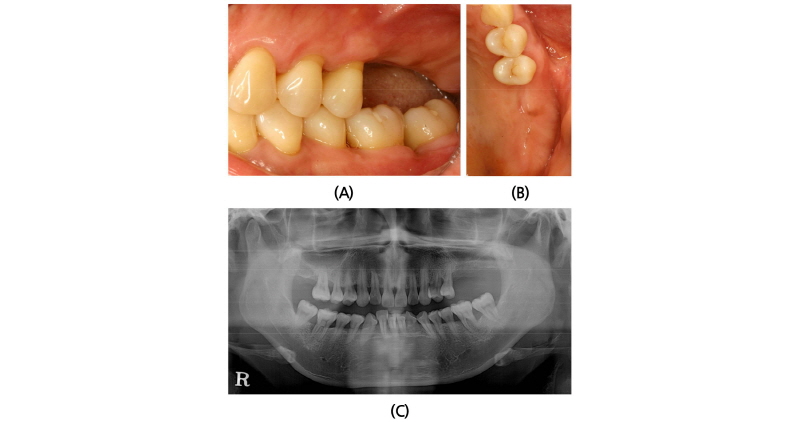
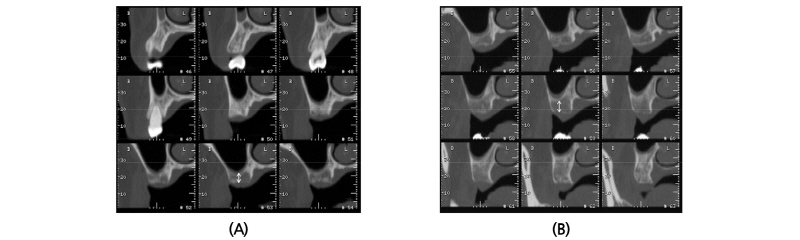
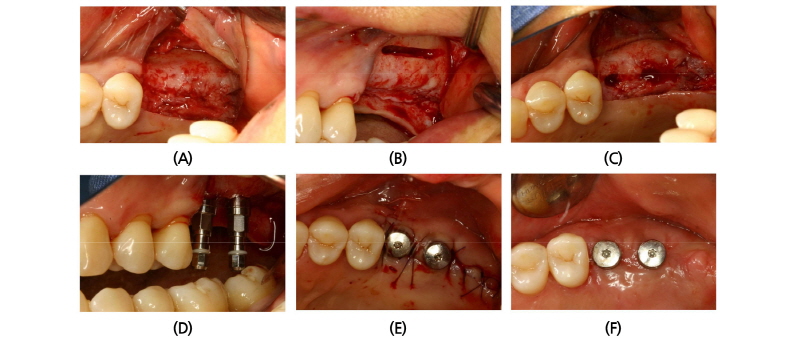
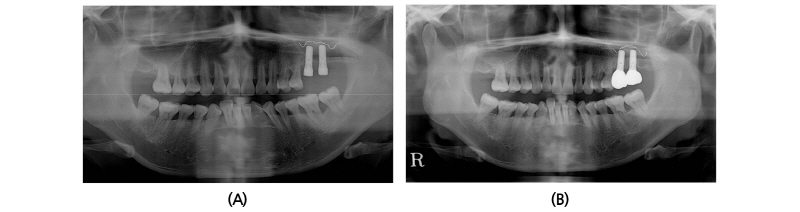
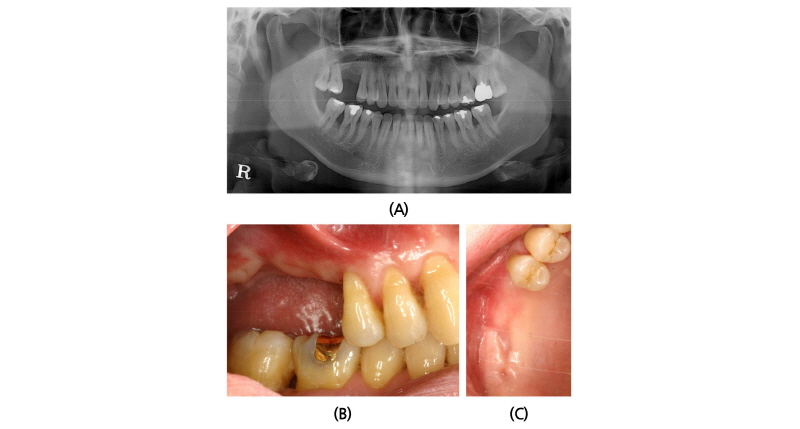
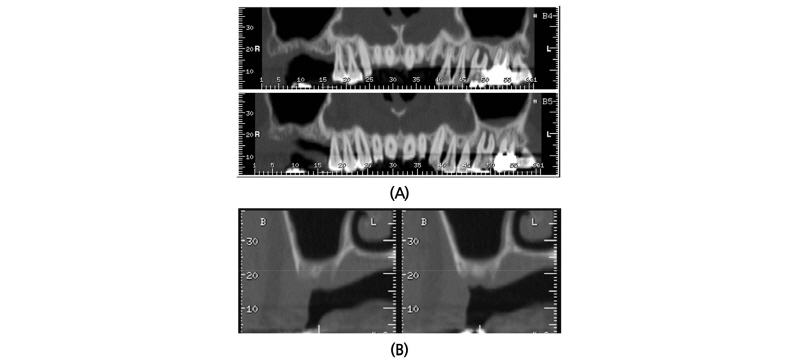
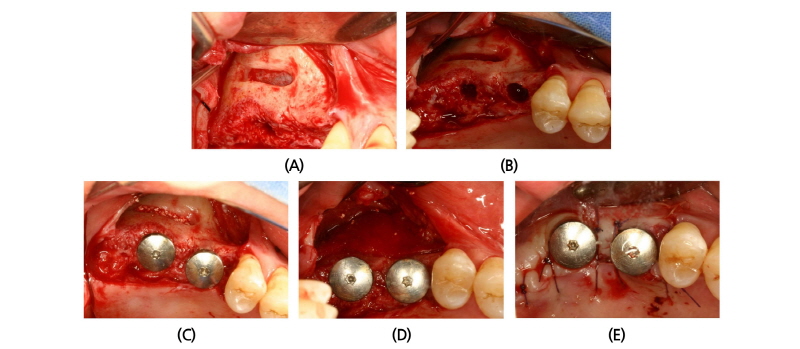
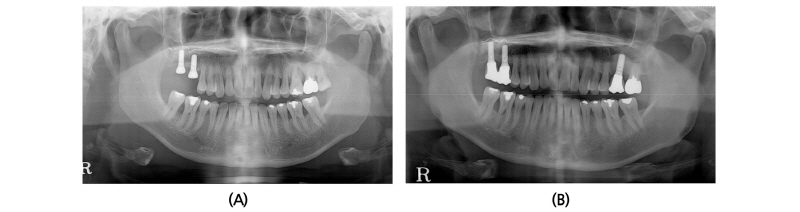
A 45-year old female patient who had missing teeth of first (#26) and second molar (#27) in left maxilla visited the clinic to plan for the reconstruction of both molars (Fig. 1). The edentulous ridge had sufficient buccopalatal width and the vertical dimension was about 8 mm from the soft tissue level (Fig. 1A, 1B). The patient was diagnosed as generalized chronic moderate periodontitis and received nonsurgical periodontal treatment prior to the surgery. In addition, regenerative therapy using bone graft materials was prepared in the intrabony defect of right mandibular first molar (#46). The missing maxillary molars were decided to be placed with implants and the panoramic view showed deficient RBH at #26 and #27 with sinus pneumatization (Fig. 1C). In computed tomography, RBH at #26 and #27 was measured to be 5 mm and 6 mm, respectively, and SFE spontaneously with implant placement using hybrid technique was planned (Fig. 2). Flap including the midcrestal incision and vertical incision at #25 distal line angle was reflected (Fig. 3A), and linear osteotomy was prepared with a piezoelectric device (Piezosurgery®, Mectron, Carasco, Italy) (Fig. 3B). Mesiodistal width of the osteotomy was about 10 mm to include both implantation site planned for #26 and #27, and was positioned about 7~8 mm from the crest paralleled along the sinus floor. Detachment of the Schneiderian membrane was limited in the internal surface of the floor and a serial drilling one step before the final diameter was done under the protection of the membrane with the sinus elevator inserted through the linear osteotomy site (Fig. 3C). Biphasic calcium phosphate (MBCP®, Biomatlante, Vigneux de Bretagne, France) of 0.5 g was grafted via lateral opening and pushed into the floor with osteotomes and final drilling was done. Straumann SLA® (Institute Straumann AG, Waldenburg, Switzerland) diameter 4.8 RN and 10 mm length implant was installed at both #26 and #27 (Fig. 3D). Non-submerged healing with healing abutment connection was done (Fig. 3E) and the stitches were removed after 10 days (Fig. 3F). Dome-shaped radiopacity surrounding the implant apex penetrated into the floor was shown immediately after the surgery (Fig. 4A) and the prosthetic delivery was done within 3 months of healing periods. Augmented sinus floor was maintained through the 6-year of follow-up (Fig. 4B).
2. Case 2
A 40-year old male patient who had missing tooth of first molar at right maxilla (#16) and discomfort of chewing in both posterior teeth visited the clinic for the periodontal treatment (Fig. 5A). Vertical tooth mobility was found on right maxillary second (#17), third molars (#18) and left maxillary first molar (#26) with severe bone loss. The patient was diagnosed as generalized chronic advanced periodontitis and #17, 18, 26 and 28 teeth were planned to be extracted. Nonsurgical periodontal treatment in whole mouth and periodontal surgeries at both mandibular posterior teeth were done. After 3 months of healing in the right maxillary edentulous area, sufficient buccopalatal width and vertical dimension about 12 mm from the soft tissue level was shown (Fig. 5B, 5C). Computed tomography revealed deficiency in the RBH with pneumatized sinus floor and horizontal bone loss especially in #17 site (Fig. 6A), which was measured to be 5 mm (Fig. 6B). The RBH of #16 sites was about 7 mm and spontaneous SFE with implant installation in both #16 and #17 using hybrid technique was planned. After flap reflection, a linear osteotomy at the lateral wall was prepared using piezoelectric device (Fig. 7A). Mesiodistal dimension of the opening was about 8 mm centered at the #17 site and slightly extended to the #16 site. The osteotomy positioned at 7~8 mm from the crest in #17 area and ran parallel along the sinus floor which had inclination from the #16 site. After detachment of the Schneiderian membrane limited in the floor, a serial drilling one step ahead of the final diameter was done with sinus elevator inserted through the lateral opening (Fig. 7B). MBCP® of 0.5 g was grafted via lateral osteotomy site and through the drilling site using osteotomes. Drilling of the final diameter was prepared and Straumann SLA® diameter 4.8 WN with 10 mm length implant was installed at both #16 and #17 (Fig. 7C). Absorbable collagen sponge (CollaTape®, Zimmer Dental, Carlsbad, CA) was covered on the lateral osteotomy site (Fig. 7D) and non-submerged healing was done (Fig. 7E). Dome-shaped sinus floor augmentation around the implant apex was shown immediately after the surgery (Fig. 8A) and prosthetic delivery was done within 3 months of healing periods. The level of SFE was maintained through 4-year of follow-up (Fig. 8B).
III. Discussion
Sinus floor elevation through the transalveolar access is a blind technique of which the visual access has been limited and possible yet not detectable laceration of membrane might occur during the surgical procedures. Risk of tearing in transalveolar approach might be involved with the failure in controlling the lifting process against the elasticity of the Schneiderian membrane, the quality of membrane attachment to the maxillary bone, the inter-implant distance of multiple placements and maxillary sinus anatomy including sinus floor inclination and septa10. By preparation of minimized linear osteotomy at lateral wall in hybrid technique, it was possible to reduce the perforation rate due to the direct instrumental access to the floor under surgeon’s view and the protection of membrane while transalveolar penetration with sequential drilling has been done.
Detachment of the sinus membrane was limited to the floor area around the future installation site in hybrid technique and not extended further into adjacent sinus walls, which was different from the conventional lateral approach. The reason for the minimal detachment was that the sinus lifting in hybrid technique basically depended on the same mechanism with the transalveolar approach, which could be explained by hydraulic pressure exerted on the bone plug. Detachment of the membrane prior to SFE might be effective in the distribution of pressure on the membrane while lifting, decrease of the tension focused on a small spot and thereby resulted in an uniform apposition of graft materials around the implant apex penetrated into the sinus cavity. Also, limited detachment might give little chance to cause membrane laceration, of which was highly reported in the lateral approach with the average prevalence of 19.5% (range 0~58.3%)11. The perforation rate in the hybrid technique was reported to be 4.5% (3 of 67 surgical sites) and none of the perforated cases were related to the implant failures12. The perforation sites could be immediately detected and repaired with collagen membrane through the lateral linear osteotomy sites and as a result, the trauma and patient morbidity related to the surgery could be reduced.
In studies of conventional osteotome technique, it has been reported that 4~8 mm of sinus elevation with a perforation rate of 24% was shown in a human cadaver study13, and the average vertical height in bone gain was mostly from 3.5~5 mm14. In the present cases, the hybrid technique was applied in the RBH with 5~7 mm with multiple (two) implants and the vertical bone gain was about 5~6 mm which made it possible to place 10 mm of implant length. Neither of the cases was involved with the membrane perforation. In radiographic evaluation, round dome-shaped radiopaque mass surrounded each apical area of implant and the space between the implants was smoothly overlapped. The augmented bone height was consistently maintained through the follow-up periods and no specific crestal bone resorption around the implants was shown.
