

Ⅰ. Introduction
For patients with chronic periodontitis and posterior teeth lost over a long period of time, supra-eruption of teeth and occlusal disharmony occur, which may eventually lead to extraction of all remaining teeth.1As implant prostheses have become popular in completely edentulous patients, either fixed prostheses or removable overdentures have become viable options.2 When compared with removable overdentures, fixed implant prostheses are superior in terms of allowing more air escape during speech, a reduced inter-arch space requirement, and fewer excessive gag reflex.3 Not only are function and esthetics recovered, but the treatment also provides psychologically confident treatment results compared to complete denture treatment. Furthermore, there are fewer prosthetic complications and alveolar bone resorption around implants, which leads to more convenient maintenance.4,5 Along with highly rated patient satisfaction and easier maintenance, full-mouth rehabilitation with fixed implant-supported prosthesis is preferred by both patients and clinicians.
Fixed implant prostheses can be restored in single, segmented, or full-arch splinted forms, but there are certain advantages when implants are splinted together. If fabricated in a one-piece superstructure without a cantilever, cross-arch stabilization can be achieved, and less stress is induced on the implants, which leads to less marginal bone loss around the implants.6,7,8 However, the distortion of the maxilla and mandible happens upon biting and mouth opening by the action of masticatory muscles and condyles.9 Picton reported that the mandible shows greater distortion than the maxilla due to contraction of the masticatory muscles.10 The mandibular flexure that is caused by the action of the lateral pterygoid muscle, which serves to protrude the mandible and open the mouth, affects not only the shape and width of the mandible but also the fit and longevity of one-piece implant-supported prosthesis.11,12 In such cases, a wide opening test of the mouth can be applied and observe whether the patient feels any discomfort in the masticatory muscles.13,14
This case report presents a satisfactory treatment outcome of full-mouth rehabilitation in an edentulous patient with one-piece full-arch implant-supported prostheses.
Ⅱ. Case Report
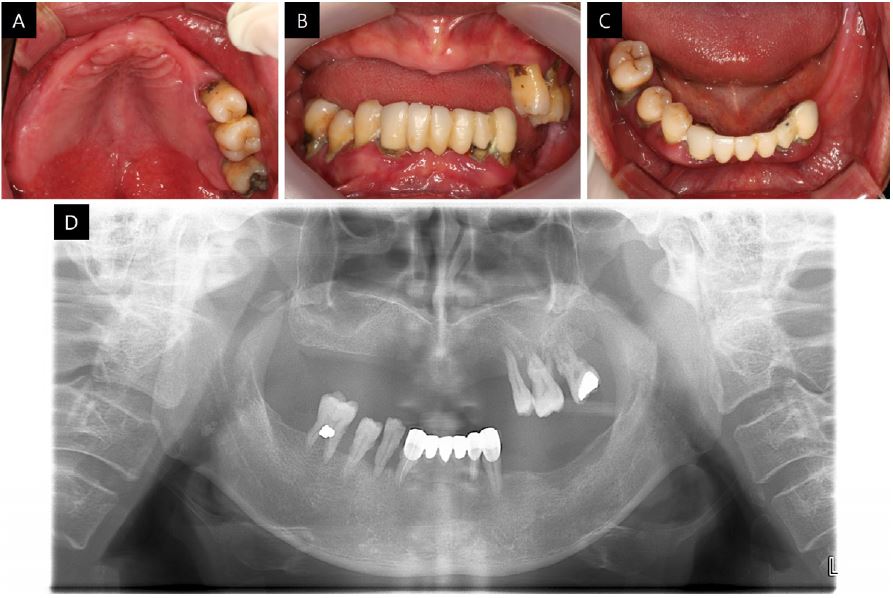
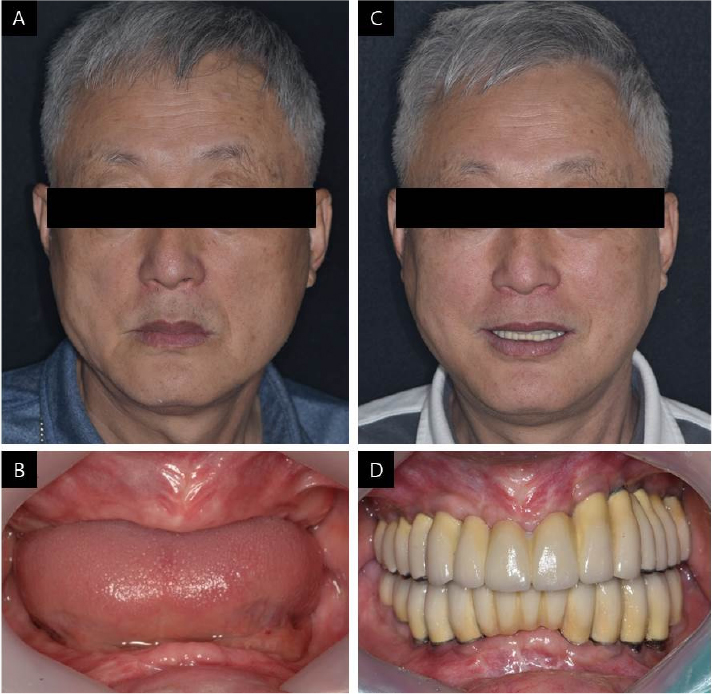
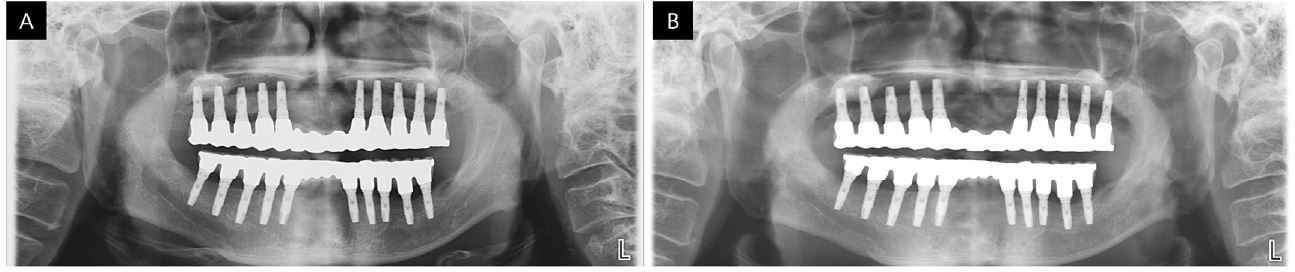
The patient presented in this case was a 64-year-old man with diabetes and hyperlipidemia, with a chief request for implant-supported restoration in the edentulous area. In the intra-oral examination, all remaining teeth had signs of severe chronic periodontitis and had erupted beyond the occlusal plane where extraction was inevitable (Fig. 1). The patient presented with decreased height of the lower third of the face, lack of lip support, wrinkles, and drooping commissures around the corner of the mouth.
After extraction of all remaining teeth, the patient became fully edentulous, and upper and lower provisional dentures were fabricated using the conventional centric jaw-relation record method. Three months after extraction, provisional dentures were duplicated as radiographic stents for dental cone beam computed tomography (CBCT) to evaluate the alveolar bone status. Sinus lift and mandibular block bone grafting were performed at the maxillary and mandibular canine and first premolar sites under general anesthesia. After six months of bone grafting, duplicated dentures were again used to perform CBCT for alveolar bone evaluation, and we decided to place 20 Osstem implant fixtures in total (US II 3.75 × 8 mm and 4.0 × 12 mm; OSSTEM, Seoul, Korea) from the canine to second molar on both the maxilla and mandible. Duplicated dentures were surveyed to fabricate surgical stents with parallel holes. During osseointegration of implants, provisional dentures were adjusted and relined with a tissue conditioner for use, and after six months, second-stage surgery was performed.
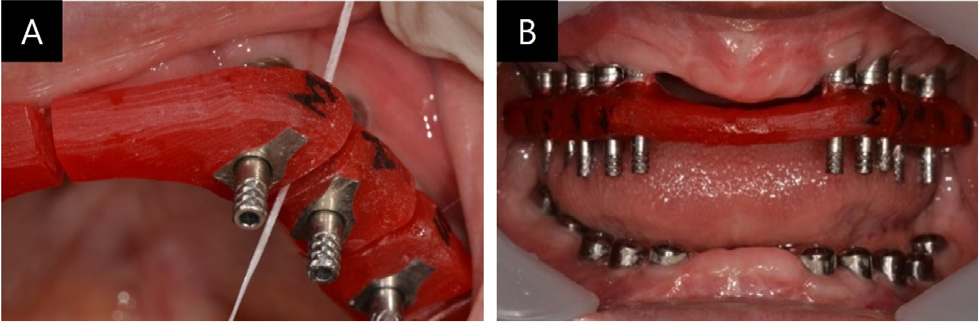
After two months of the second-stage surgery, impressions were taken using individual trays and pick-up type impression copings (US Fixture Pick-up Impression Coping; Osstem Implant, Busan, Korea), with silicone impression material (Imprint II; 3M ESPE, St. Paul, MN, USA) for provisional restoration. For more accurate restoration, the impression copings were splinted with autopolymerizing acrylic resin (Pattern Resin; GC Corporation, Tokyo, Japan) on the master cast from the first impression procedure at least 24 hours before being sectioned to compensate for shrinkage.15,16 Then, they were reconnected in the mouth with Pattern Resin for the second impression procedure (Fig. 2).
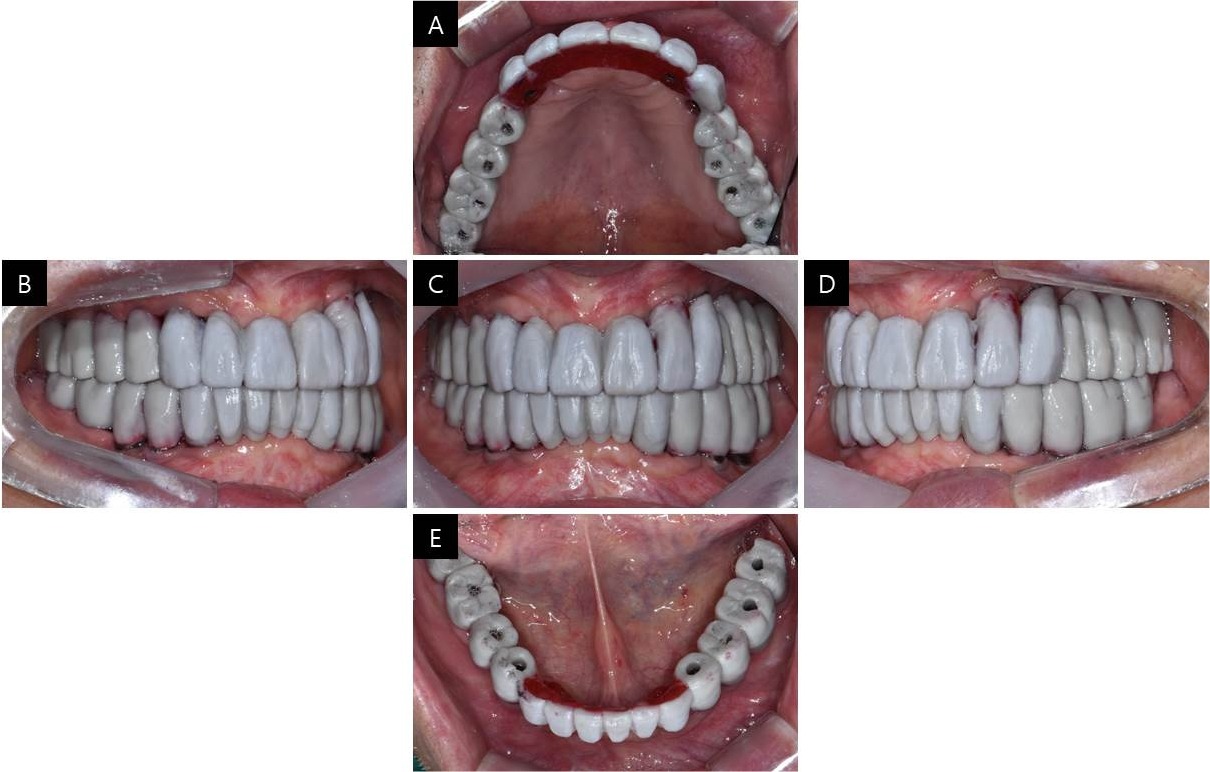
To decide which abutment to select, master casts were fabricated, and implant angulation was found to be parallel enough to restore it in a one-piece superstructure. Since the patient was well adapted to the vertical dimension of the former dentures, it was once again applied on provisional fixed implant prosthesis, and centric relation was guided using lucia jig to be transferred on a semi-adjustable articulator. Provisional restorations were designed through CAD software and delivered in the mouth with temporary cylinders. To verify the vertical dimension of the provisional restoration, a TMJ series was taken, and both condyles were within normal limits.
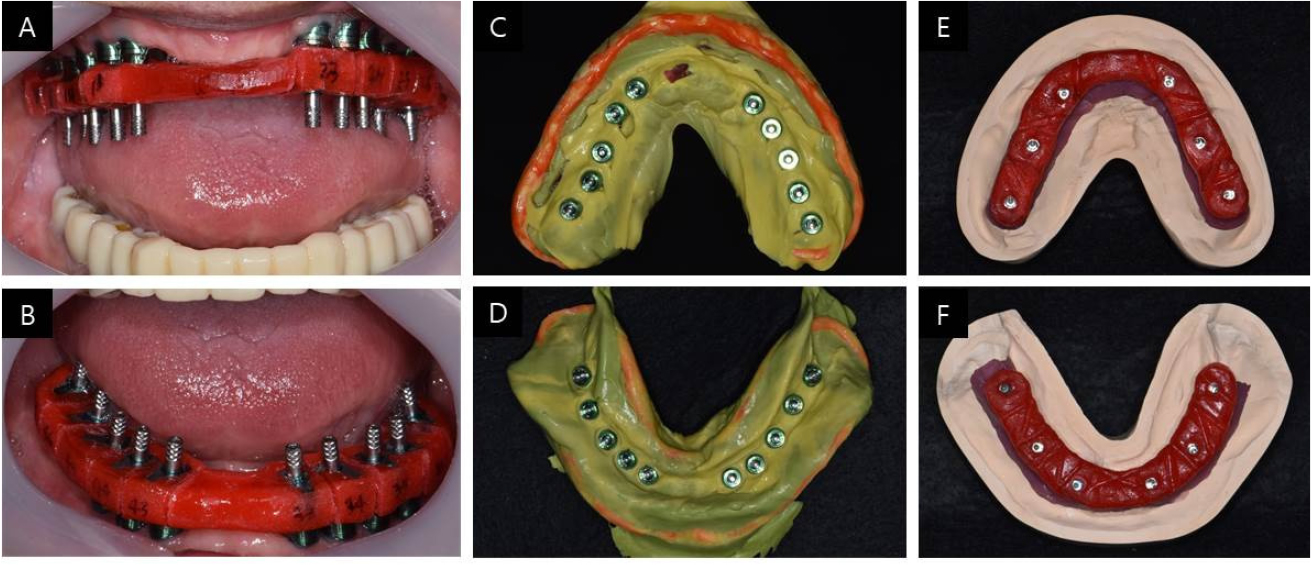
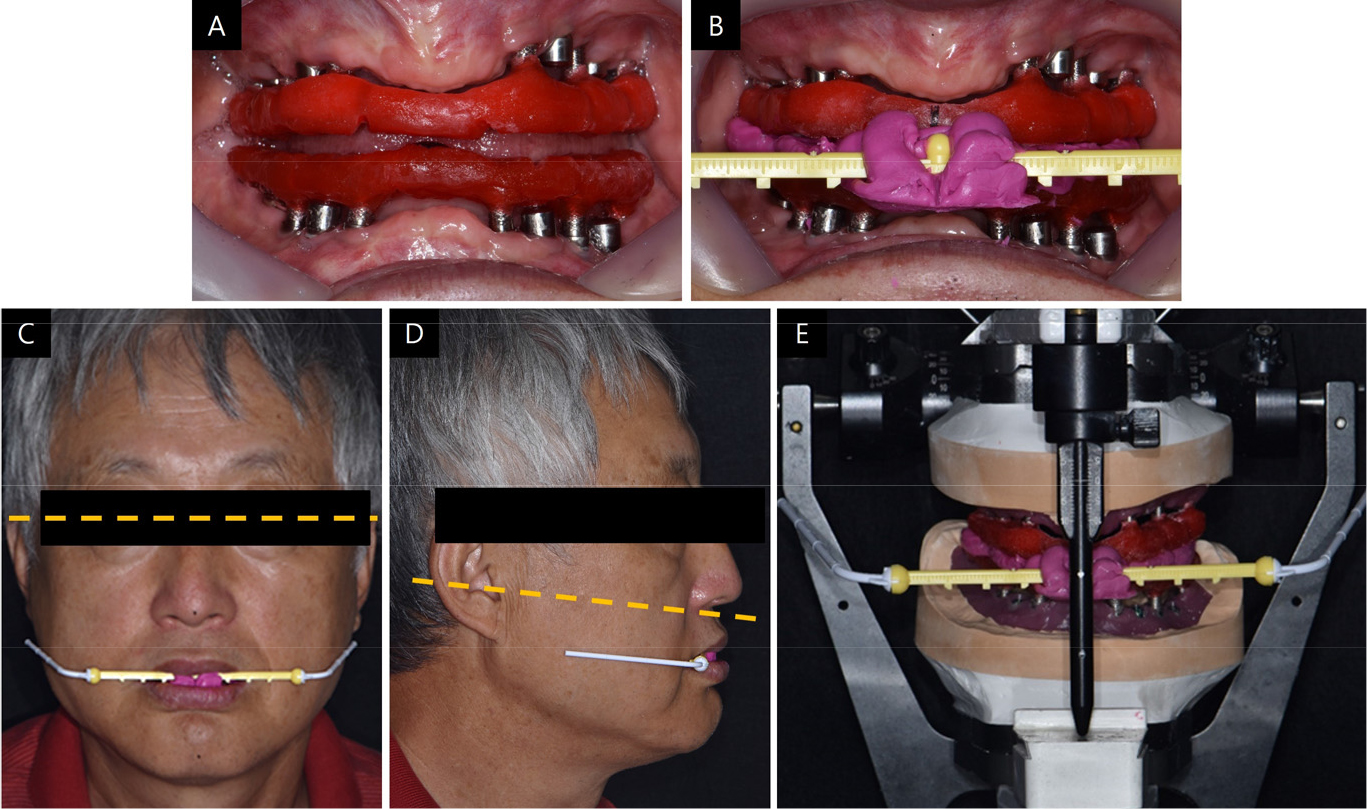
Three months after provisional restoration, a final impression was taken to make a definitive prosthesis using pick-up type impression copings that were splinted together with Pattern Resin on the second master cast that was used for provisional restoration (Fig. 3). The jaw-relation record was acquired using a lucia jig, made with temporary cylinders, and the vertical dimension was set the same as provisional restoration and former dentures. The Willis method was also used for esthetic evaluation, and TMJ checks were performed. The occlusal plane was transferred using the POP bow system, which provides information on the interpupillary line and ala to the tragus line, and then transferred to an articulator (Fig. 4).
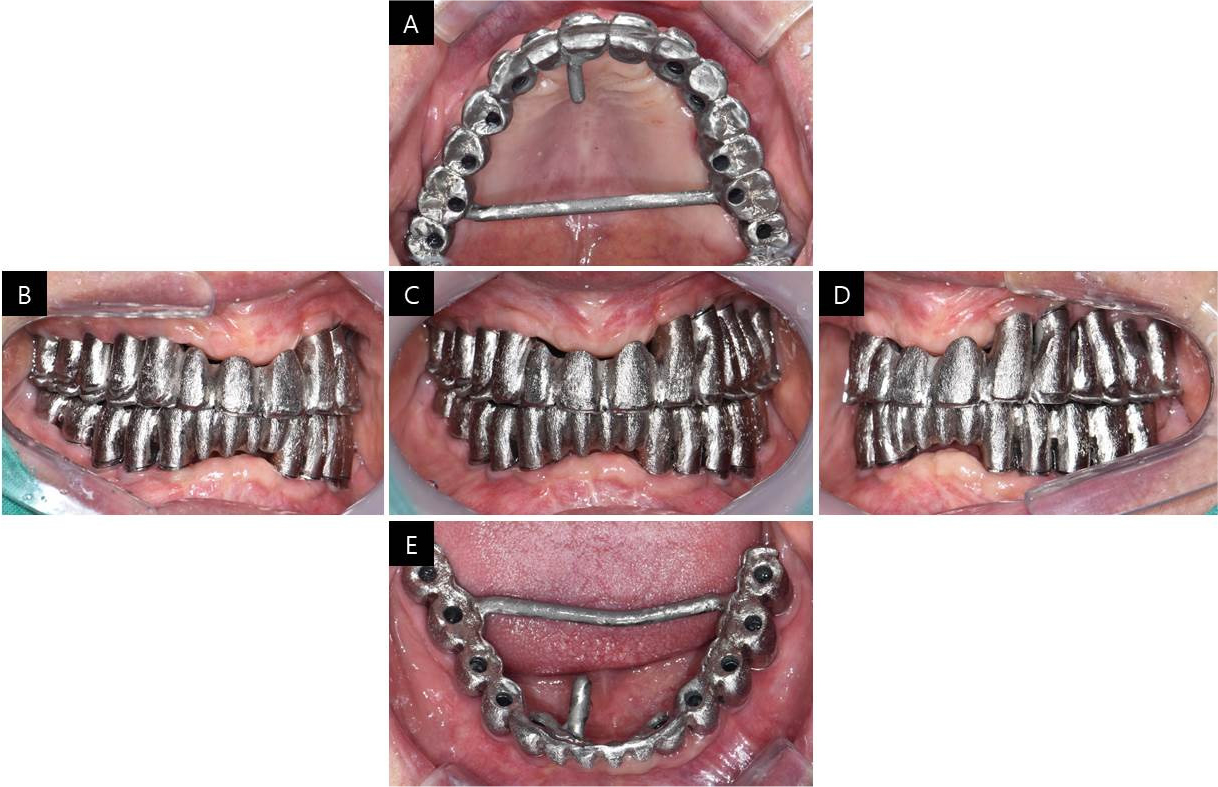
CAD software was used to make customized abutments for a screw-cement retained prosthesis (SCRP). For better esthetics, the abutments were adjusted in the mouth for the equi-gingival margin and anodized to a gold color. A full contour wax-up was performed to fabricate the metal framework and was assayed in the mouth to check the final contours of the restoration and screw access holes (Fig. 5). To fabricate the metal framework, the wax was cut back, and the framework was cast in palladium and gold alloy, suitable for high-fusing porcelain (Fig. 6). The adaptation of the metal framework with abutments was checked with Fit Checker II (GC Corporation, Tokyo, Japan). We also confirmed that there was no muscle discomfort upon wide opening of the mouth, after which we proceeded with a one-piece metal superstructure.
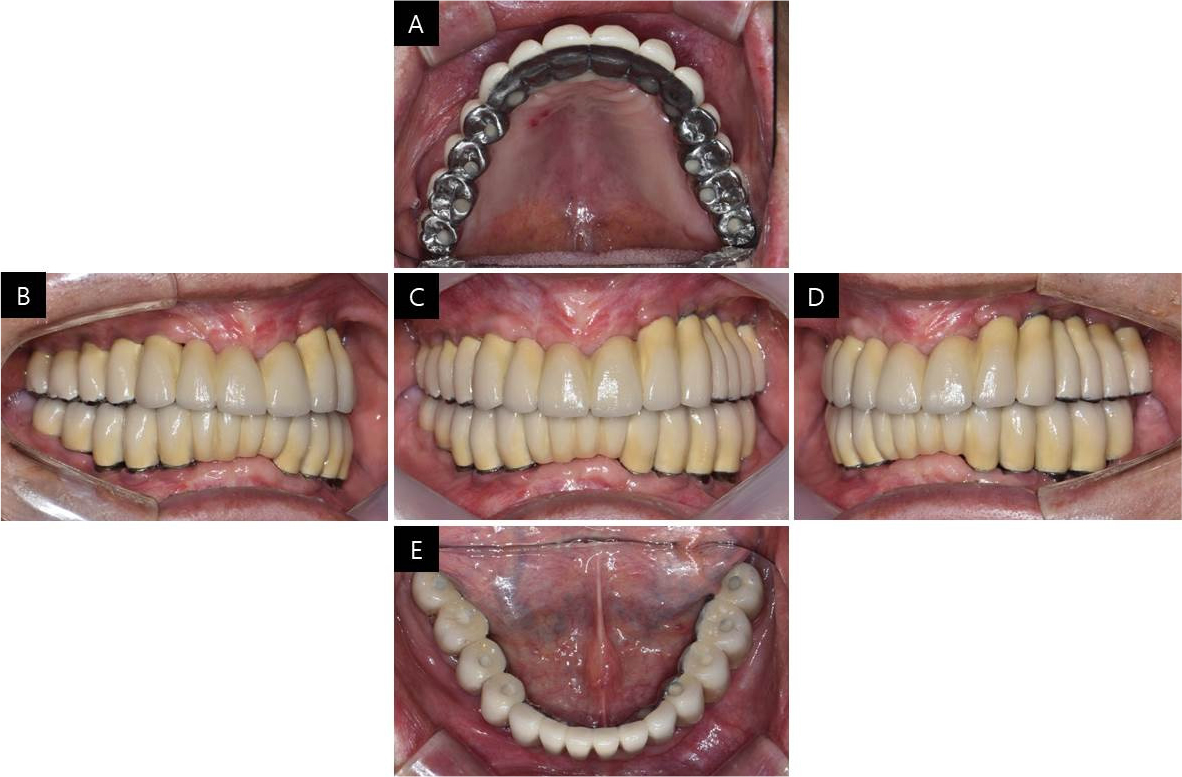
Finally, porcelain build up was performed with metal occlusion in the maxilla and porcelain occlusion in the mandible for esthetics. The abutments and final prosthesis were checked in the mouth and luted together with self-adhesive resin cement (RelyX U200; 3M ESPE) (Figs. 7 and 8). To remove excess resin cement and gain passive fit, the luted prostheses were removed from the mouth and connected to fixture analogs to make a cast, and hexagon surfaces were rounded off until no resistance was felt while tightening the screws. The provisional prostheses were reconnected, and the patient was instructed to visit after one week. Definitive prostheses were delivered to the patient after one week, and occlusal adjustments were made to obtain canine guidance upon eccentric movement and mutually protected occlusion upon anterior guidance. From the panoramic view, it can be seen that the prostheses were well connected to the fixtures (Fig. 9). To protect the porcelain occlusion from chipping, the patient was instructed to use a night guard every night.
Ⅲ. Discussion
In completely edentulous patients, either fixed or removable implant prostheses should be considered according to the patient’s preference, financial status, and residual ridge. If the quality of the edentulous residual ridge is favorable and the patient can afford bone grafting, fixed implant prosthesis can be selected.17 In this case, the superstructure was fabricated as SCRP type for its passivity, retrievability, and ease of excess cement removal, since the implants were placed parallel enough to allow an ideal path of prosthesis insertion.18
Additionally, splinting the superstructure as a rigid one-piece prosthesis can be considered for cross-arch stabilization and less marginal bone resorption around implants. Cross-arch splinting has the advantage of enhancing the retention and resistance of the restoration upon lateral forces during functional and non-functional movements and distributing occlusal forces evenly, which leads to fewer mechanical complications.7In this case, because of insufficient anterior bone volume to allow implant placement, the implants were placed in the posterior area and restored as a one-piece splinted superstructure. However, it may be more difficult to obtain a passive fit of the splinted prosthesis compared to a fixed segmented prosthesis. In order to achieve a passive fit in this case, the hexagonal connections of the abutments that were luted with the superstructure were rounded off until no resistance was felt while tightening the abutment screws. This technique reduced preload stress in the abutment interface.19 For long-term success of implant prostheses and fewer prosthetic complications, periodic observation and maintenance of the implant-abutment interface must be followed.
Splitting a one-unit fixed implant prosthesis must be considered when maxilla and mandible distortion upon mastication and opening of the mouth occurs due to the activation of the mandibular condyles and masticatory muscles. There is more flexure and a greater reduction in the width of the mandible while the maxilla shows little to no measurable changes. Therefore, a subjective evaluation of patient comfort must be performed with a one-piece fixed implant prosthesis in the mandible to determine whether the patient feels any discomfort in mouth opening muscles when asked to open the mouth.9,10In order to resolve this mandibular flexure issue in splinted implant prosthesis, Paez et al. introduced a way to split the prosthesis in half at its midline.13 It was reported that by splitting the metal framework in half at its mandibular midline, there was less screw loosening and marginal bone resorption around the implants. This technique not only compensates for the mandibular flexure, but also relieves stress in the metal framework and extends implant longevity.20
In the present patient, the SCRP-type fixed implant prosthesis, which provided ease of maintenance, passive fit, and esthetics, was fabricated in a one-piece splinted metal substructure to achieve cross-arch stabilization. However, no significant marginal bone resorption or patient discomfort was observed during the two-year follow-up period. For the long-term success rate of implant-supported prostheses, regular check-ups must be provided along with appropriate patient education on oral hygiene and maintenance care.
Ⅳ. Conclusion
In this case, a patient with chronic periodontitis who became completely edentulous was successfully treated using a one-piece full-arch fixed implant-supported prosthesis. Confirmation of the passive fit between abutments and superstructure, and comfort upon opening the mouth with a one-piece prosthesis must be performed to obtain cross-arch stabilization and less alveolar bone resorption around implants. The patient was also satisfied with the definitive prosthesis, regarding esthetics and functional recovery. This suggests that the one-piece superstructure not only gives patient satisfaction but also a good prognosis.
