

Ⅰ. Introduction
Dental implants can be a valid prosthetic treatment to replace single tooth.1 Although the 10-year survival rates of tissue-level dental implants has been reported to be greater than 98%,2 complications are another issue. Complications of the implant include osseointegration failure of implant fixture, peri-implantitis, abutment screw loosening, screw fracture, loss of implant prostheses and implant fracture.3, 4, 5 Marcelo et al. (2014)6 suggested implant failures can be classified as early failures and late failures. Early failure occurs during the stage of osseointegration, while late failure occurs after the occlusal load is applied. Fractures of the implant, one of the late failures, are uncommon but once they occur, they are difficult to treat.7
Tissue-level implants are implant types designed to reduce the marginal bone loss after implant placement by placing the platform 1.5 to 3 mm above the bone level. Some studies using finite element analysis have reported that marginal bone loss may be associated with screw fractures and fixture fractures.8, 9 In addition, the ITI standard diameter solid screw fixtures have a thick wall with excellent strength, which can withstand heavy occlusal force.10 In this regard, some clinicians may expect that tissue-level implants are resistant to fractures. Indeed, the reported prevalence of fracture in tissue-level implants is very low.11, 12 However, there was no study to compare the prevalence of fractures between tissue-level and bone-level implants.
Risk factors for implant fractures are the type of prosthetic structure (single crown or fixed partial denture), parafunction, inappropriate occlusion, crestal bone resorption and screw loosening.13, 14, 15
This case report shows fixture fracture that occurred two years after screw fracture in a tissue-level implant.
Ⅱ. Case Report
A 41-year-old male patient visited the clinic with a chief complaint of tooth mobility, and the maxillary left first molar was extracted. Six months later, a tissue-level implant (Straumann® Tissue Level Implant 4×10 mm, Straumann, Basel, Switzerland) was placed with maxillary sinus elevation. The screw-retained prosthesis was applied 5 months after implant placement.
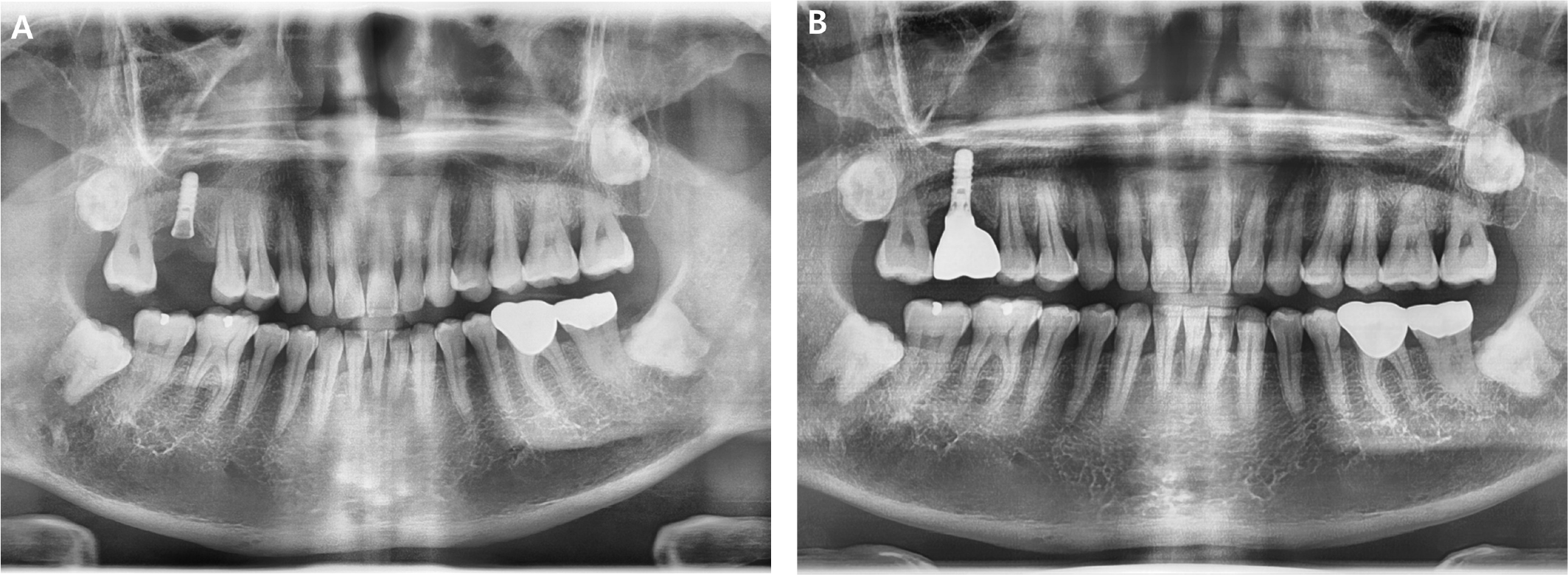
About 10 years later, the patient visited the clinic again with the fractured upper part of the implant. Panoramic radiograph confirmed the fracture of abutment screw (Fig. 1A), but the screw fragment was not visible due to overgrown soft tissue. The screw fragment remaining inside the fixture was removed using a screw retrieval kit (HELP kit® , Dentium, Seoul, Korea) under flap elevation, and a healing abutment was placed. After soft tissue healing, a conventional impression process was performed and the newly made cement type prosthesis with a solid abutment was applied (Fig. 1B).
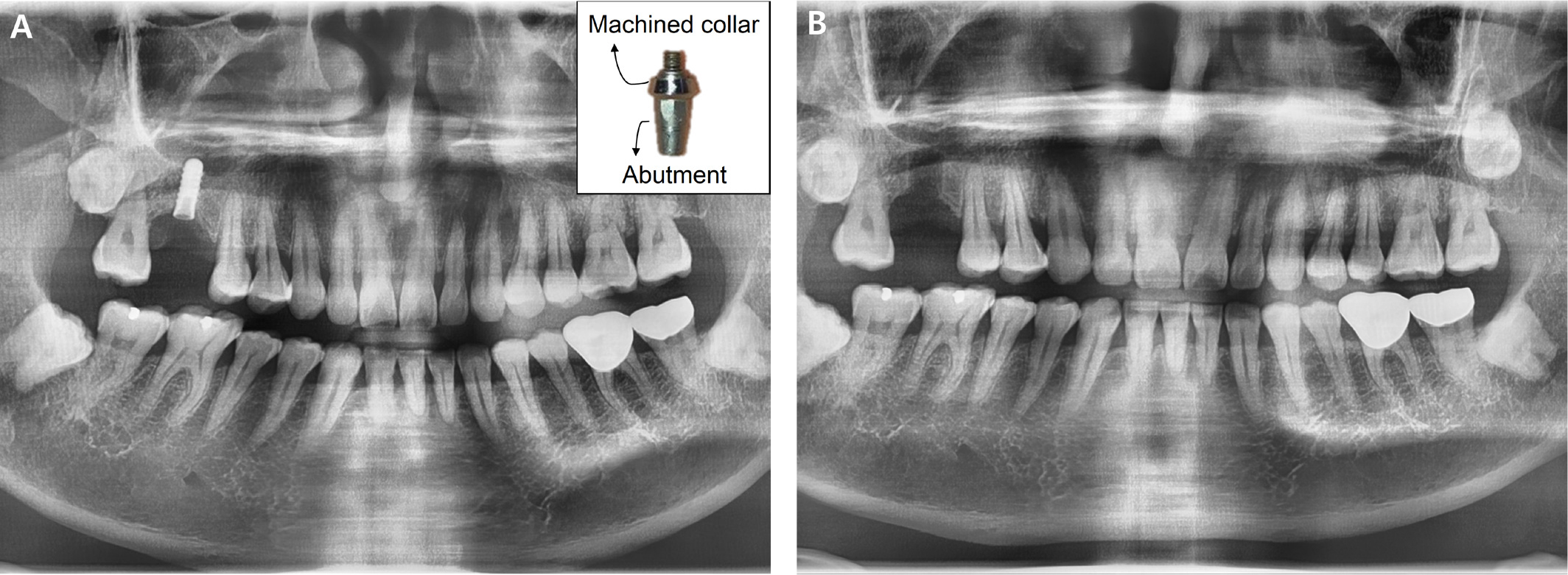
However, only about 1.5 years later, he returned to the clinic with a fractured implant. In addition to abutment and screw fracture, fixture fracture was also observed at the interface between the machined collar and the rough surface (Fig. 2A). The fractured implant was surgically removed using a trephine bur under flap elevation (Fig. 2B). The placement of a new implant wider than the previous one was planned.
Ⅲ. Discussion
Various causes of implant fractures have been reported.13, 14, 15, 16, 17 Chrcanovic et al. (2018)16 and Goiato et al. (2019)17 suggested that implant diameter can influence the incidence of implant fractures. Small diameter implants have a reduced surface area and are mechanically weak.17 Chrcanovic et al. (2018)15also reported that fractures of the ITI tissue-level implants were more frequent than other implants, but were limited to narrow implants with a diameter of less than 3.3 mm. In this case, the diameter of the fixture was 4.0 mm. However, it might not be sufficient for the posterior teeth, since they are subjected to greater occlusal load than the anterior teeth. In addition, the occlusal surface of molar teeth is greater than that of premolar or anterior teeth. Therefore, it is recommended to use wide implant with a diameter of 5 mm or more in the posterior area. Chrcanovic et al. (2018)16 reported small diameter implants were more fractured, especially in the posterior area.
Another cause of implant fracture is excessive bite force.18 The parafunctional habits (bruxism, clenching etc.) and the excessive occlusal forces can cause not only implant failure, but also many other complications. However, no traumatic occlusion or parafunctional habits were observed in this study and tooth wear in all dentition was not severe enough to consider abnormal function. On the contrary, Esquivel-Upshaw et al. (2014)19 reported no association between occlusal force and implant fracture.
The fracture can be resulted from mechanical fatigue failure due to prolonged use. Goiato et al. (2019)17 reported implant fractures usually occur 3-4 years after placement. In this study, a screw fracture occurred 10 years after implant placement and a fixture fracture occurred 1.5 years later. Yokoyama et al. (2002)20 concluded that titanium in a biological environment absorbs hydrogen, which may be the cause of fractures of titanium implants.
It should be noted that the screw fracture occurred before the fixture fracture in this case. In screw-retained implants, the stress produced by the micromovement of screws can apply constant tension on the implant fixtures.14 Therefore, screw loosening often causes implant fracture and can be considered as a warning signal.10, 18 This implies the importance of periodic maintenance. If screw loosening is found during the recall, clinicians should retighten the screw using an appropriate torque.
When screw fracture occurs, it is necessary to remove the fractured screw without damaging the internal threads. Various techniques have been introduced to manage fractured abutment screws, including hand instruments, ultrasonic scalers, and rotary instruments.21 Mizumoto et al. (2018)21 suggested that if the fractured fragment was removed and the fixture was not damaged, a new restoration could be applied. In this case, the remaining fragment was removed and a new restoration was applied. After 1.5 years, however, the screw and the fixture fractured. One possible reason may be that the damage of the internal threads was not recognized. If the internal threads were damaged, the new abutment screw would not fit properly. Non-passive fit of the prosthetic structure is one of the causes of implant fracture.22 In addition, repeated instrumentation to remove the fragment may have applied fatigue stress on the fixture. The fact that the location of fixture fracture was similar to that of screw fracture supports the above explanation.
The location of the fixture fracture was at the crestal bone level, where the interface between the smooth collar and the rough surface was located. The thickness of tissue level implants is usually thinnest at the bone crest level and the lateral bending force applied on the fixture causes fatigue stress.16
Abutment type can also affect the fracture of implants.23 Literatures reported that internal connection types provide better joint stability than external connection types and among the internal type, the conical type provides enhanced resistance to horizontal and oblique forces than the hexagon type. However, there are studies reporting no significant differences between two types.13 In this case, an internal conical abutment was used. It seems that the misfit between abutments and fixtures is more important to implant fractures than the connection type of abutments and implants.
There are some treatment options for managing implant fractures.6, 24 One is to remove the coronal portion of the fractured implant, leaving the remaining part integrated in the bone. However, this approach does not allow the placement of a new implant. In most cases, complete removal of the fractured implants can be the treatment of choice. In the present case, the fractured implant was removed using a trephine bur.
Ⅳ. Conclusion
The most important thing about implant failure is prevention. In the posterior area, it is recommended to choose a wide diameter implant and place it in the center of the occlusion if possible. Regular maintenance is also important. The occlusal adjustment should be necessary to avoid excessive occlusal force and the loosened screw should be retightened. The presence of parafunctional habits should also be examined.
