

Ⅰ. Introduction
Implants have been widely adopted as an effective method for the aesthetic and functional restoration of missing dental areas.1,2 Titanium abutments have been extensively used owing to their high strength and durability.3,4 However, in cases where aesthetics is particularly important, such as anterior regions, the metallic color of titanium abutments can lead to a grayish appearance owing to thin gingiva or possible gingival recession in the future.5 Moreover, in response to these aesthetic concerns, ceramic abutments, particularly zirconia abutments, have been used for their high biocompatibility and excellent mechanical properties.4,6,7 Nevertheless, there have been reports of fracture risks associated with zirconia abutments.8, 9, 10 These are custom-designed through CAD/CAM (Computer-Aided Design/Computer-Aided Manufacturing) and fabricated via milling. Additionally, the zirconia blocks used for milling possess high fracture toughness owing to transformation toughening. However, zirconia is brittle and vulnerable to tensile force. When tension is applied to titanium abutments, the elasticity of titanium abutments often causes deformation of metal abutments and consequently causes screw fracture. However, when tension is applied to the zirconia abutment, cracks occur in the zirconia abutment itself, causing fracture.11
Zirconia abutments are manufactured either as a one-piece or attached to a titanium base. They are attached to a titanium base offering superior mechanical properties owing to the internal connection of the metal that supports zirconia.12 Consequently, these types that are attached to a titanium base, are favored over the one-piece types.13 Furthermore, zirconia abutment fractures can occur within the walls of the abutments or between the titanium base and abutment. The causes of zirconia abutment fractures include manufacturing defects in the abutment itself,14 strong internal stresses,1 thin sidewall thickness,8,9 excessive reduction of the mesial wall for adjusting the emergence profile of the implant,15 functional overload,16 and non-functional habits causing overload.17
In this case series, fractures of anterior zirconia-customized abutments were examined, and the underlying causes were discussed.
Ⅱ. Case Reports
1. Case 1
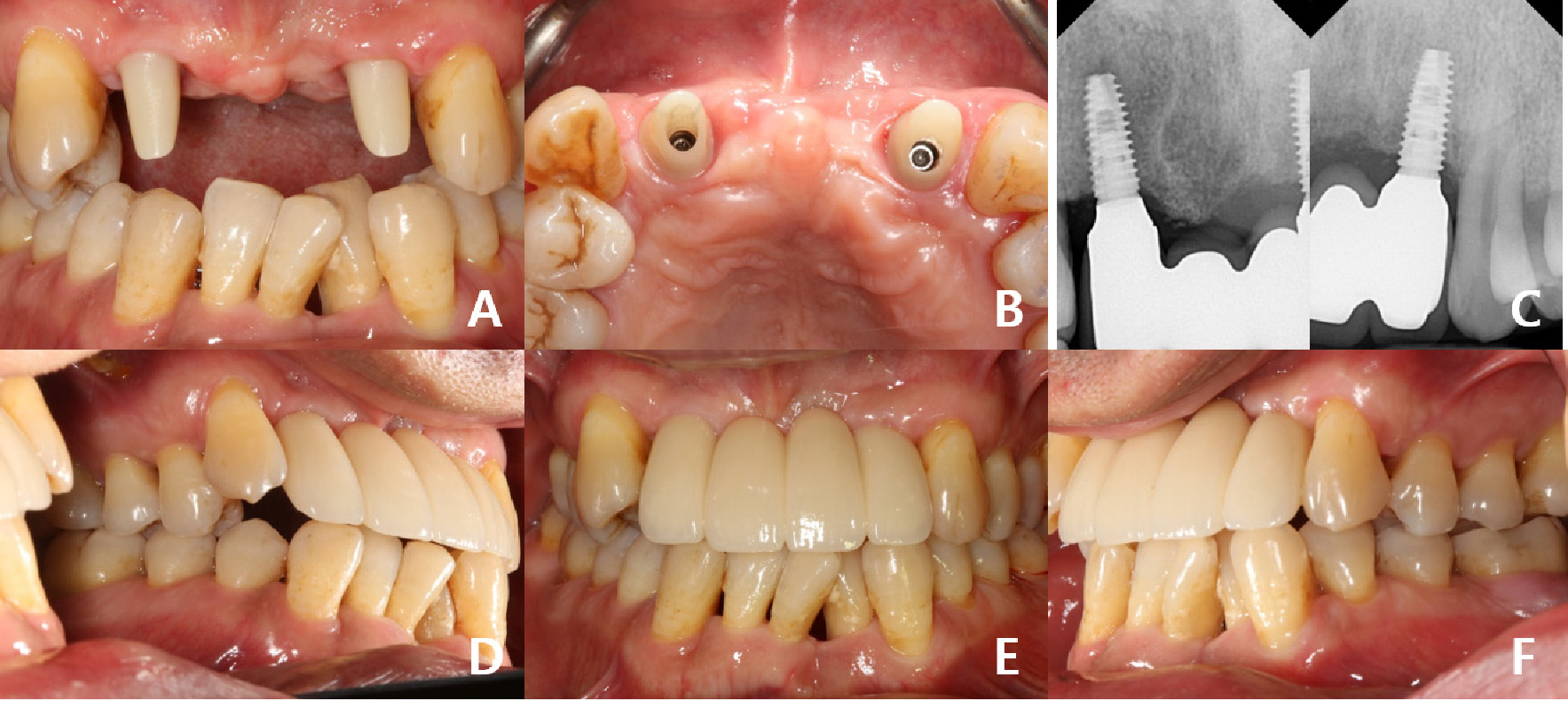
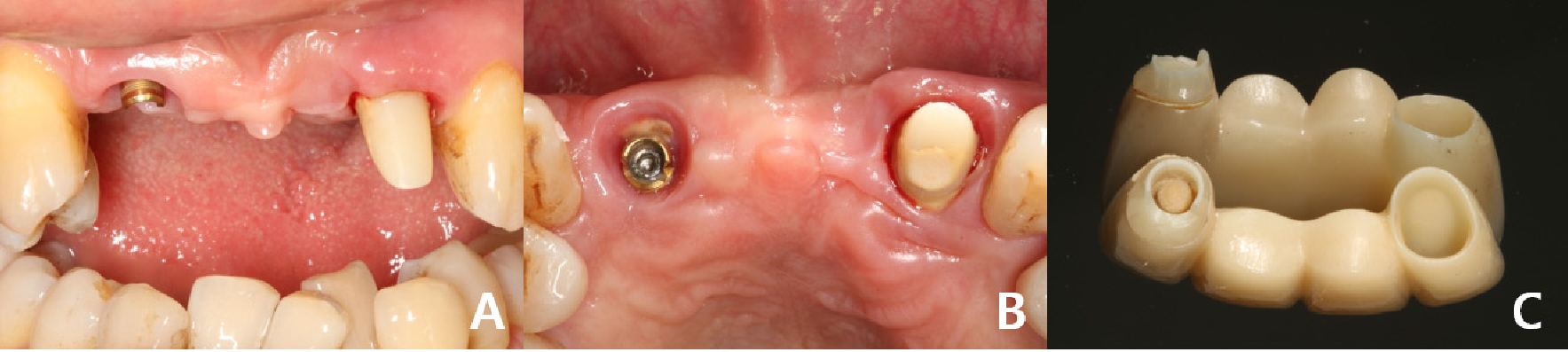
A 53-year-old male patient reported anterior prosthesis mobility as the primary concern. Two years prior, internal type implants (ø4.0×10, Luna®; Shinhung, Seoul, Korea) were positioned both lateralis of the maxilla (#12, #22), and customized zirconia abutments were used to fabricate a screw-cement retained implant prosthesis (SCRP). A 4-unit all-ceramic fixed implant prosthesis (FIP) was cemented with a eugenol-free, elastic polymer cement (Premier® implant cementTM; Premier Dental Co., PA, USA) (Fig. 1). Clinical and radiographic examination indicated no sign of loss of osseointegration of the implants. Abutment screw loosening was not observed. Fracture of the zirconia abutment was observed at the site of the abutment connection to the titanium base on the buccal side of the tooth, with the titanium base slightly exposed and remnants of the abutment fragment. No fracture was observed on the abutment, but adhesive loss was observed on the coronal one-third of the abutment (Fig. 2). The previous restoration was replaced with custom titanium abutments and an all-ceramic FIPs was set using resin-modified glass ionomer cement (Rely X luting; 3M ESPE, MN, USA) (Fig. 3).

2. Case 2
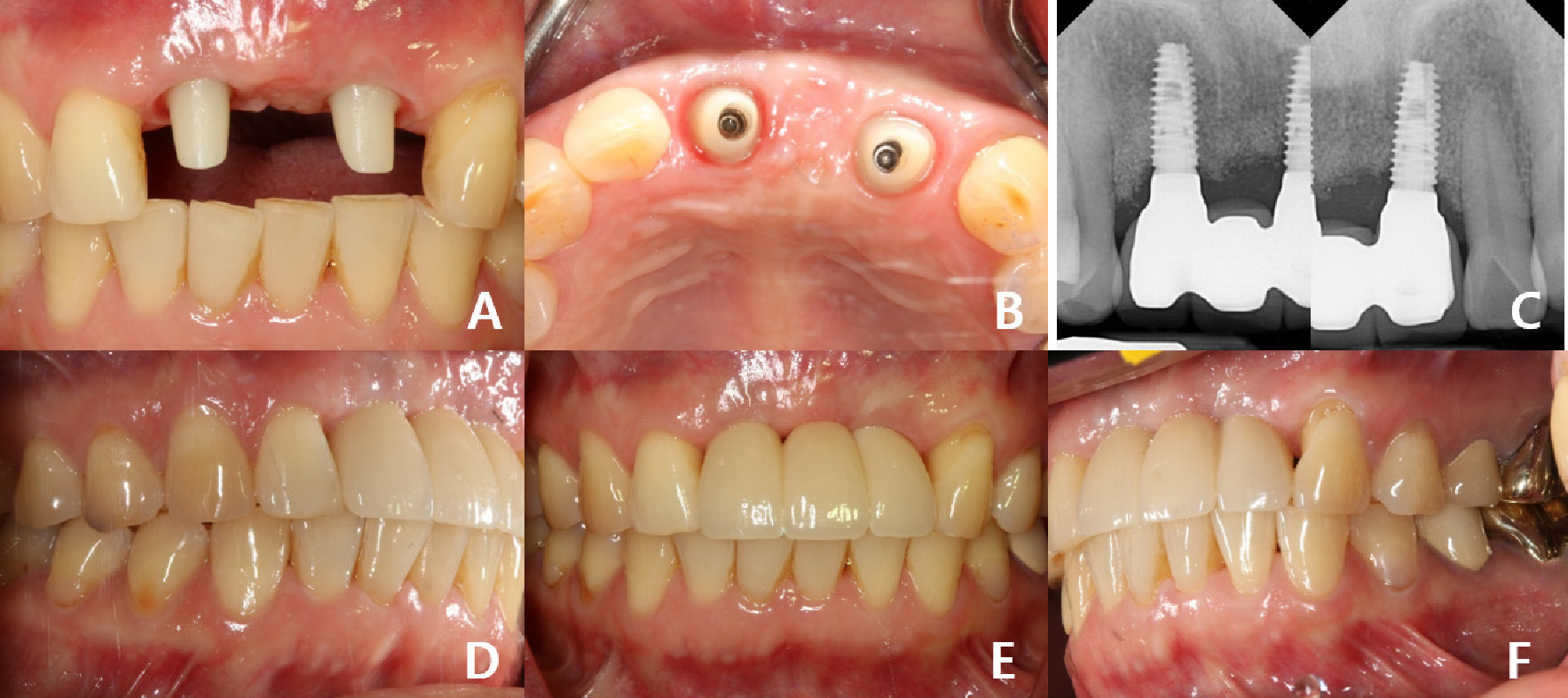
A 60-year-old female patient presented with a chief complaint of a falling out anterior prosthesis during a meal. Internal type implants (ø4.0×10, Luna®; Shinhung, Seoul, Korea) were placed in positions maxillary right centralis (#11) and left lateralis (#22), and customized zirconia abutments were used to fabricate an SCRP. A 3-unit all-ceramic FIP was cemented with a eugenol-free, elastic polymer cement (Premier® implant cementTM; Premier Dental Co., PA, USA) (Fig. 4). Clinical and radiographic examination showed no sign of loss of osseointegration of the implants. Abutment screw loosening was not observed, and fractures of the zirconia abutments for both implants (#11 and #22) were observed. The fracture site for #11 showed complete exposure of the titanium base on the buccal side, whereas the upper part of the titanium base for #22 was exposed, with remnants of abutment fragments adjacent to the titanium base margin (Fig. 5). The previous restoration was replaced with custom titanium abutments and an all-ceramic FIP was set using resin-modified glass ionomer cement (Rely X luting; 3M ESPE, MN, USA) (Fig. 6).


Ⅲ. Discussion
If an abutment fracture occurs, a new abutment and upper prosthesis are required, costing the patient extra money and time, and consequently affecting the quality of life of the patient. Therefore, to prevent zirconia abutment fracture, it is important to have an accurate understanding of the cause, solution, and prevention method of zirconia fracture.
Considering the timing and location of fractures, material characteristics, and manufacturing process errors for both cases, there are six possible causes: (1) manufacturing defects of zirconia blocks,14 (2) thin sidewall thickness of zirconia,8,18 (3) strong internal stress,8 (4) implant angulation,19 (5) concentration of excessive stress according to occlusal aspect,16 and (6) adhesion problem of titanium base and zirconia abutment (Table 1).13
Table 1.
Possible causes of zirconia abutment fracture
| 1. Manufacturing defects of zirconia blocks | Bottino et al.14 |
| 2. Thin side wall thickness of zirconia | Aboushelib et al.8 |
| 3. Strong internal stress | Aboushelib et al.8 |
| 4. Implant angulation differences | Thulasidas et al.19 |
| 5. Concentration of excessive stress according to occlusal aspect | Paolantoni et al.16 |
| 6. Adhesion problem of titanium base and zirconia abutment | Linkevicius et al.13 |
Typically, an acute defect in the inner edge of the abutment, especially in the cervical region, can be regarded as the origin of fracture, which is caused by a defect in the block or the manufacturing process. Additionally, all zirconia abutments used in this case report were fabricated from the same block of multilayered zirconia (Perfit ZR STML; Vatechmcis, Seoul, Korea) (Fig. 7). However, given that this particular failure has not been observed in other patients or prosthetic cases, it is difficult to prove whether a defect in the block itself was the cause of failure.

The minimum thickness for zirconia abutment walls ranges between 0.5 and 0.8 mm.8,18 Case 1 was designed with a minimum thickness of 0.82 mm, and Case 2 was designed with a minimum thickness of 0.81 mm, so it is difficult to consider the thickness as the cause of failure (Fig. 8). Also, since the location of the fracture is the connection between the abutment and titanium base, it is expected that the problem is at the connection between the zirconia abutment and titanium base rather than the fracture caused by the insufficient wall thickness of the abutment.
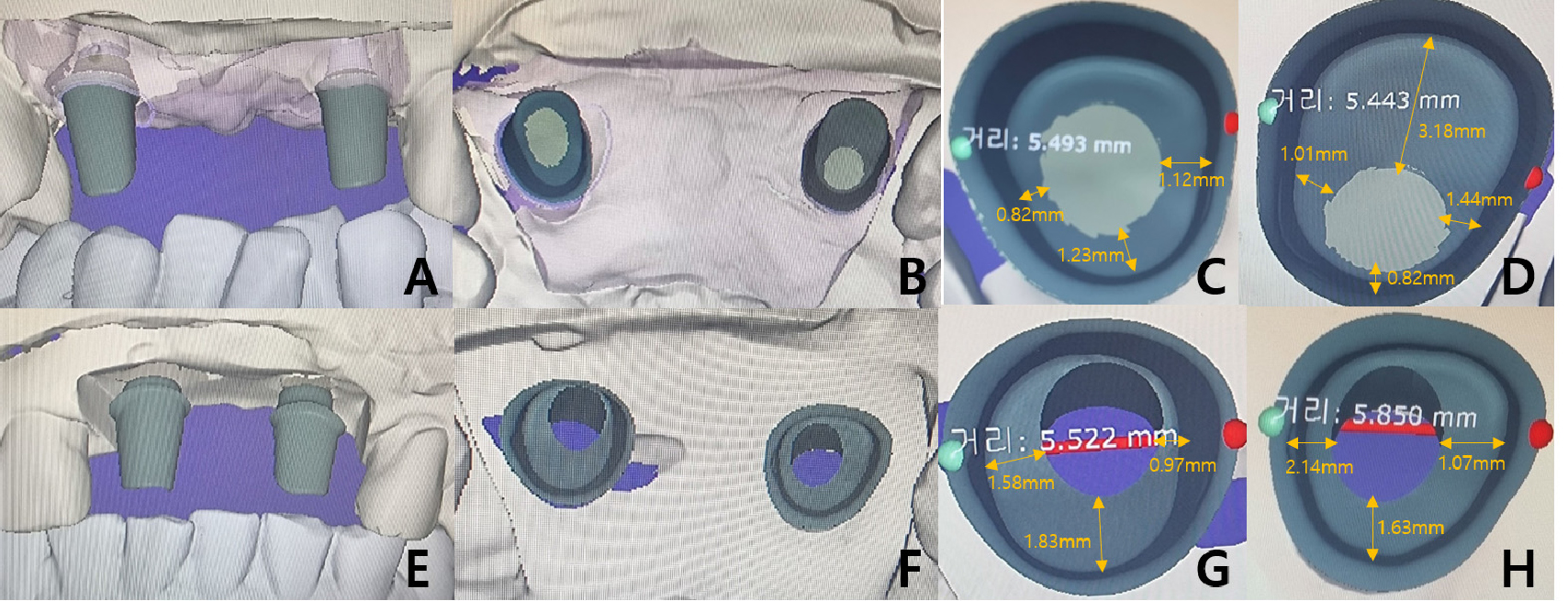
Fig. 8.
Customized zirconia abutment wall thickness measured via CAD/CAM. (A, B) Case 1 CAD/CAM design (frontal and incisal view), (C) Case 1 (#12) Wall thickness of zirconia abutment (M:1.12 mm, D: 0.82mm, L:1.37 mm, P:1.23 mm), (D) Case 1 (#22) Wall thickness of zirconia abutment (M:1.01 mm, D:1.44 mm, L:3.18 mm, P:0.82 mm), (E, F) Case 2 CAD/CAM design (frontal and incisal view), (G) Case 2 (#11) Wall thickness of zirconia abutment (M:0.97 mm, D:1.58 mm, L:0.85 mm, P:1.83 mm), (H) Case 2(#22) Wall thickness of zirconia abutment(M:2.14 mm, D:1.07 mm, L:0.81 mm, P:1.63 mm).
The possibility of fracture owing to strong internal stress between the crown restoration and zirconia abutment can also be considered. According to Aboushelib et al.8 the generation of strong internal stress can be inferred from the friction landmark observed on the surface of the fixation screw, and the stress generated from the fractured abutments at this time was 978–1228 MPa.8 However, since in both Cases 1 and 2 the fracture occurred at the titanium base joint rather than between the restoration and abutment, the possibility of fracture owing to strong internal stresses is low.
When placing implants in the anterior region, achieving precise alignment and angle congruence for two adjacent implants can be notably challenging. Differences were observed in the placement angle and direction in both Cases 1 and 2, and as an anterior implant, the protrusive guide is made on the prosthetic appliance, which may cause fracture at the prosthetic area where stress is concentrated owing to contact with the tooth during anterior guidance. Also, according to Shreedevi et al.19 when the implant apex was tilted at 20°, 0° facially and 20° lingually, 20° to lingual(42.2%), 0° (70.7%), 20° to facial (90.6%), the fracture frequency was high. In other words, as the implant apex tilts toward the face, the resistance to fracture decreases. In Case 1, the implant apex was 28° (#12) and 19° (#22) as facial, and in Case 2, 36° (#11) and 36° (#22) as facial (Fig. 9).

The last likely cause is a problem in the contact area between the titanium base and zirconia abutment. Zirconium oxide abutments are cemented onto titanium bases. Adhesion between the titanium base and zirconia abutment is a key element of the titanium base zirconia abutment. Therefore, the most likely cause of fracture is expected to be an adhesion problem between the titanium base and zirconia abutment joint.
To maintain the zirconia abutments, the height of the holding part of the titanium base should be 4–6 mm. However, the height of the holding part of the commercially available titanium base is 3.5 mm, which does not provide adequate holding force.20 Additionally, the zirconia prosthesis manufactured by milling is designed as a passive fit and does not have mechanical retention. Therefore, strong adhesion and high holding power are required between the titanium abutment and zirconia abutment. Resin cement is used for this high holding power. In the retention of titanium base and zirconia abutments, the dislodging force of self-adhesive resin cement(G-CEM LinkAce; GC Corporation, Tokyo, Japan) was the highest at 1338 N, and RelyX U200 (3M ESPE, MN, USA) showed a dislodging force of 665 N.13 RelyX U200 (3M ESPE) was used to bond titanium base and zirconia abutment in both cases.
The possibility of occlusion-related abutment fracture in the anterior region may be particularly emphasized if there is inadequate anterior guidance. The exerted force has the potential to induce a fracture in the vulnerable section of the zirconia abutment, specifically at the joint between the titanium abutment and zirconia abutment. In Case 1, protrusive guidance was provided only with the anterior prosthesis alone. Nevertheless, in Case 2, protrusive guidance was provided along with the prosthesis and #12. However, the overjet and overbite of both cases were shallow, and the guidance was verified via fixed provisional restoration (Figs. 1 and 4).
Ⅳ. Conclusion
In this report, Two cases of anterior zirconia abutment fracture were introduced and the causes of fractures were reviewed. To prevent anterior zirconia abutment fracture, it is important to manufacture a successful zirconia implant abutment with an appropriate abutment wall thickness and correct implant placement angle. It is important to closely monitor the abutment wall thickness and placement angle and prevent abutment fracture owing to force overload by considering the adhesion between the abutment and restoration, as well as the solid adhesion between the titanium base and zirconia abutment connection.
