

Ⅰ. Introduction
Dental implant placement is the treatment of choice for patients with tooth loss. In edentulous patients, dental implants provide better stability than dentures. Implants can also be a satisfactory choice for posterior single-tooth restorations.1 Implants maintain success rates well above 90% in different clinical centers for observation periods of up to 8 years.2 These results could be compared with those for fixed prostheses supported by natural teeth, which are approximately 90% after 5 to 10 years.3
However, over the years, various complications have been observed,4 which can be categorized into three groups based on their origins: biological processes, mechanical inadequacies, and patient adaptation.5 Causes of biological adverse events may include insufficient attached gingiva, poor oral hygiene, infection due to oral microflora, and peri-implant bone resorption.6Mechanical problems with dental implants can be caused by defects in design or material, poor design, nonpassive fit of the prosthetic framework, physiologic or biomechanical overload, occlusal trauma, and undetected screw loosening, which can be attributed to bruxism and malfunction.7 Additionally, the abutment screw may fracture as a result of fatigue.8
Implant-supported restorations may fail due to technical problems, which can be divided into two groups: those related to the implant components and those associated with the prosthesis.9 Technical problems related to implant components include abutment screw fractures, which have been observed at an increasing rate, particularly among individuals who have had their implants for 20 years or more. The occurrence rate of abutment screw fractures has been reported to be as high as 8%.10,11 The primary reason for screw fracture is undetected screw loosening, which can be due to bruxism, an unfavorable superstructure, overloading, or malfunction.12 Abutment screw fractures frequently occur at the junction of the screw head and shank or at the transition point where the threaded section begins.13,14 The ease of removing the fractured screw depends on the level of the fracture. Several dental manufacturers have offered kits designed to manage screw separation. Examples include the Fragment Fork (Dentsply, Sirona, Sweden), Abutment Screw Retrieval Kit (Nobel Biocare, Sweden), and Service Kit (Straumann, Switzerland) for implant maintenance. Using these kits with care to avoid damaging the internal threads of the implant is important.15 However, screws that cannot be removed in this way may necessitate either re-doing the screw hole or removing the implant fixture itself. Several ways to remove implant screws are available, including ultrasonic techniques,16 the use of a self-made screwdriver,8 and a specialized removal kit.17 This study aimed to report dental implant removal due to various instances of implant abutment and screw fracture. In this study, we highlight the indications for implant removal due to mechanical failure.
Ⅱ. Patients and Methods
This study included patients (n=13) who were referred for dental implant removal owing to abutment and screw fractures between 2010 and 2024. The Institutional Review Board of our hospital granted an exemption for this study based on the use of existing collected data in a manner that ensures participants could not be identified directly or indirectly. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and principles of good clinical practice.
Fractured implant screw fragments were removed by an experienced surgeon when the prosthetic department failed to remove them. The surgery was performed under sedation (midazolam, Dormicum®; Roche, Basel, Switzerland) and local anesthesia (2% lidocaine hydrochloride injection; Huons Co., Ltd, Seongnam, Korea). The implant fixture containing the fractured screw was removed using a round bur (1.5 mm diameter) and dental elevator. After removal, immediate or delayed implant placement was performed if the patient expressed a desire to undergo reimplantation at our hospital. Bone grafting or collagen plug implantation (Collagplug; Bioland, O-song City, Chungchungnam-do, Korea) was performed if the bone defect was large after removal. Radiographs and removed implants were analyzed to determine which company and product each implant belonged to, using a website for dental implant identification (https://whatimplantisthat.com/).
Ⅲ. Results
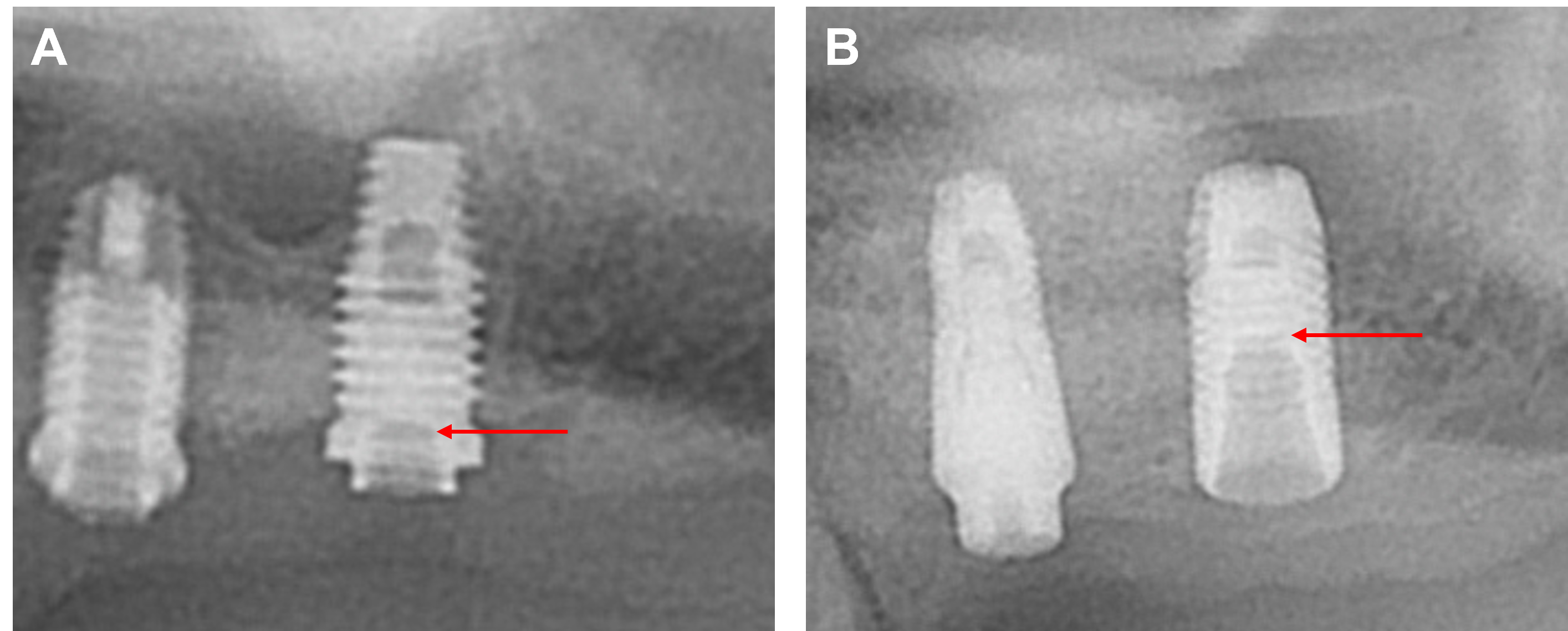
The sex, age, type of implant, implant site, and fracture location of the screw were analyzed for each patient (Table 1). Of the 13 patients, 11 were men and two were women. Patients’ ages ranged from 36 to 74 years, with an average of 63.4 years. The total number of implants removed from the 13 patients was 15. The implant types were divided into external (Fig. 1A) and internal (Fig. 1B). The number of external types of implants and internal connections was five and ten, respectively. Only one abutment fracture was observed (Fig. 2A); the remaining fractures were screw fractures.
Table 1.
Patient Demographics and Implant Characteristics
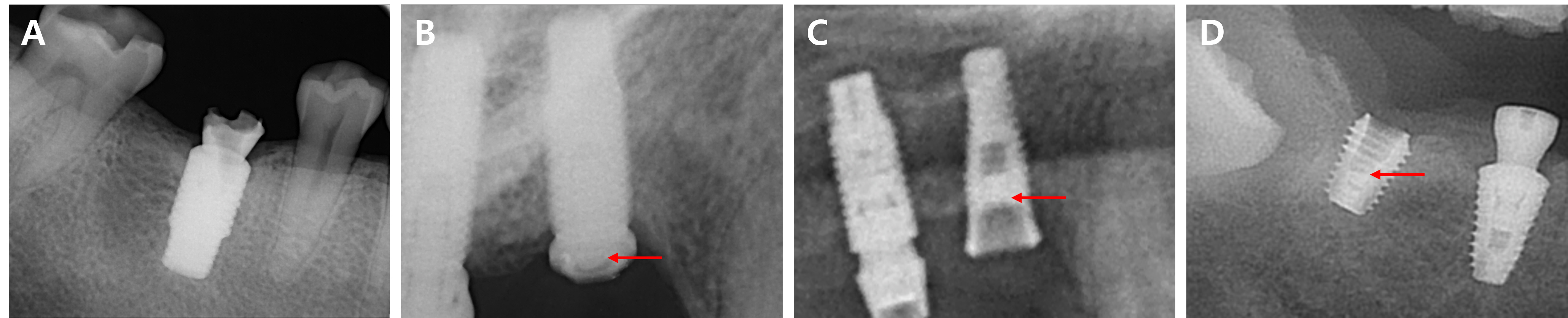
The screw fracture locations were classified as the cervical third (Fig. 2B), middle third (Fig. 2C), or apical third (Fig. 2D). Of the fractured implants, nine were in the maxilla and six were in the mandible. None of the implants involved the anterior part, three involved the premolars, and 12 involved the molar regions. Single implants were more common (n=14) than multiple implants (n=2).
Ⅳ. Discussion
Dental implants have been used for tooth restoration for a considerable amount of time, with some of them being more than a decade old. From the earliest implants, numerous trials and errors have shaped the evolution of implants to their current state, with many products appearing and disappearing along the way.18 Although dental implants provide good retention and support during various treatments to replace missing teeth, they are also vulnerable owing to their structure and environment. In particular, their mechanical structure, which is composed of several parts, can cause them to fracture.19 The implant fixture, the abutment, or the screws connecting the two could experience failure.20 In this study, we analyzed the cases where the abutment or screw fractured leading to the removal of the implant. Furthermore, we identified trends in the cases with severe component failure. Eleven of the 13 cases involved men, which can be explained by the fact that men have a stronger bite force on average than those of women, resulting in increased force on the implant and, therefore frequent fractures.21 The location of the implants that fractured also had an impact, as none occurred in the anterior teeth, all were in the posterior teeth, especially the molars. This suggests that individuals tend to exert greater chewing forces on the molars when hard foods are encountered or when they need a large bite force.22,23
In contrast to simple screw fracture cases, where the screw can be easily removed and replaced with a new one, some attempts to replace fractured abutment screws are successful, necessitating the removal of the implant fixture itself. Of the 15 implants removed for this reason, only two had fracture lines located in the cervical third, which is a relatively shallow location, while the rest had fractures in the middle and apical thirds, indicating that the deeper the fracture, the more difficult it was to remove, primarily due to instrument accessibility issues.
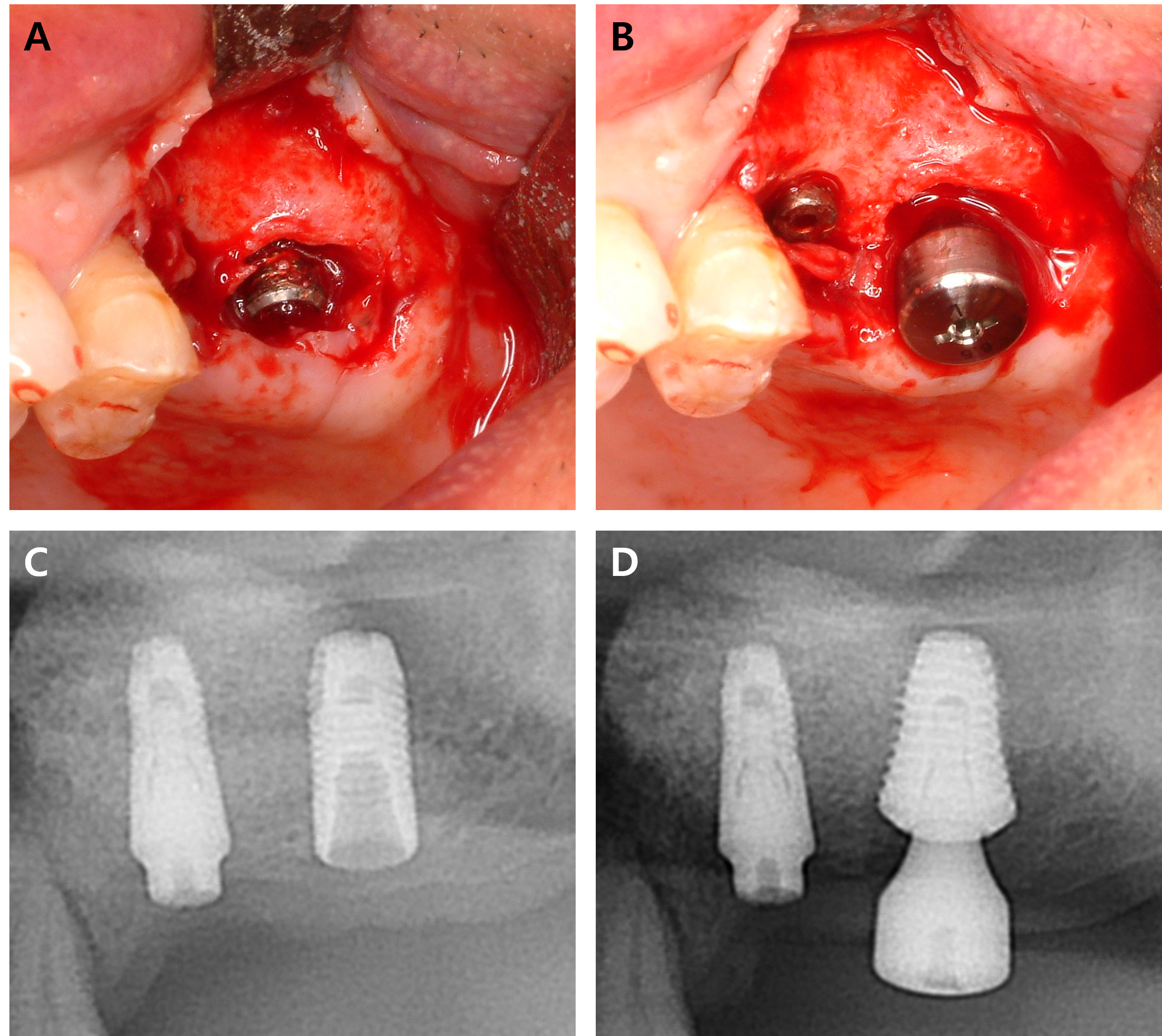
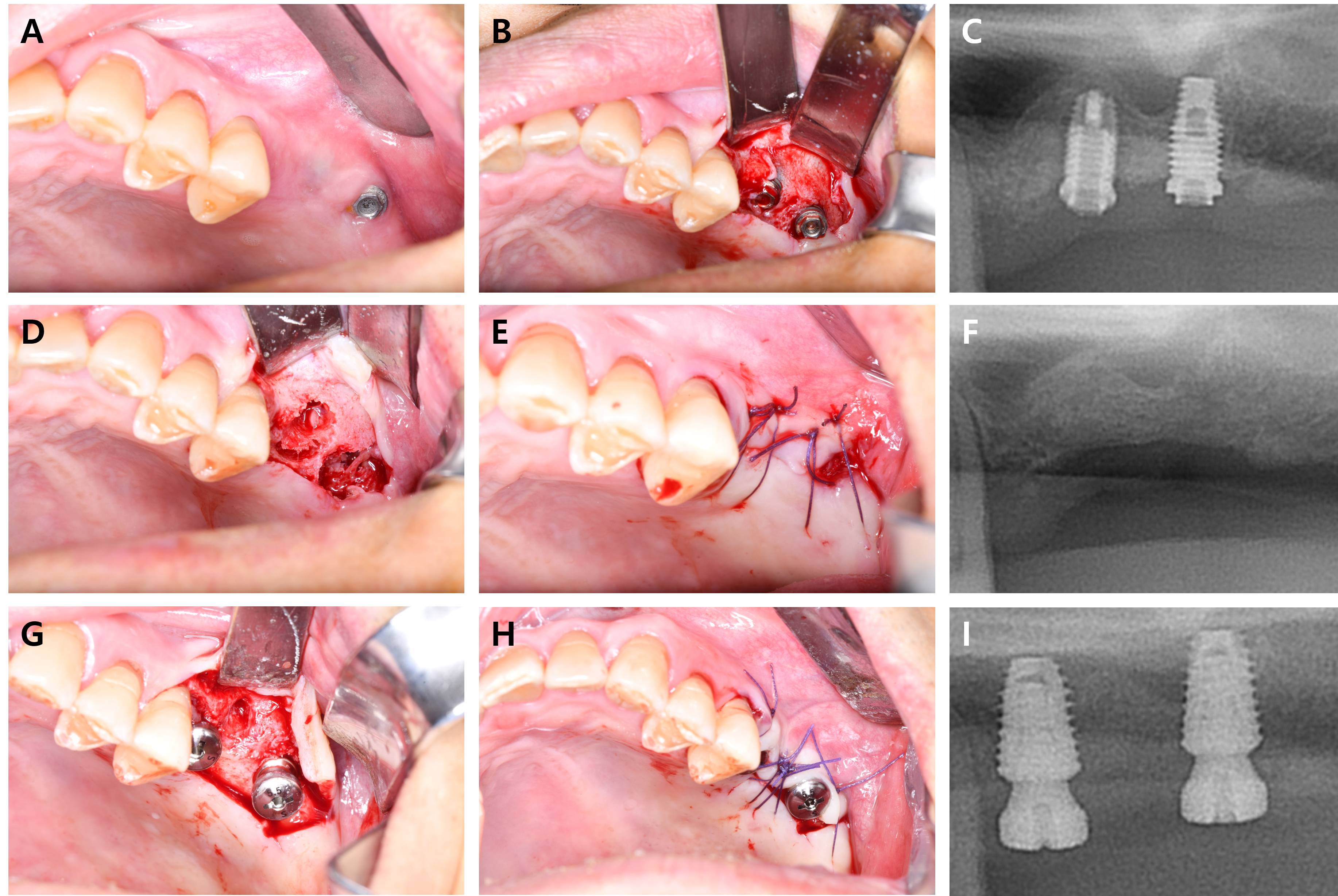
When the patient desired re-implantation after the implant fixture was removed, delayed implantation was usually performed; however, cases where immediate implantation was performed have also been observed. Fig. 3 represents immediate re-implantation and Fig. 4 displays delayed implant placement after 4-months of bone healing. Immediate implant placement resulted in significantly lower implant survival than that observed with delayed implant placement (94.9% versus 98.9%), resulting from a lack of osseointegration.24 However, when a fixture with a wide diameter is implanted, the probability of early failure is relatively low.25 Moreover, the number of patient visits and discomfort can also be reduced.
However, determining whether the fracture was challenging to remove solely because of its location was difficult, as the removed implants were of various products, and in some cases, ascertaining the specific product was challenging. In this situation, special techniques are required to remove the screws.26 Notably, abutment screws from systems not commonly used in the prosthesis department are relatively difficult to pull. In addition, although various implant systems from different companies are available, no particular company's implants show a tendency to be more prone to damage. A limitation of this study is that the number of patients analyzed was not sufficient; therefore, a statistically meaningful analysis could not be performed owing to a lack of data.
Ⅴ. Conclusion
When an implant screw fracture occurs in the lower third of a dental implant, removal is often difficult. Regular check-ups and periodic screw tightening are mandatory to prevent severe complications such as screw or abutment fractures. Failed implants should be removed and replaced with new dental implants.
